Pharmacotherapeutic group: Bacterial and viral vaccines combined.
ATC code: J07CA02.
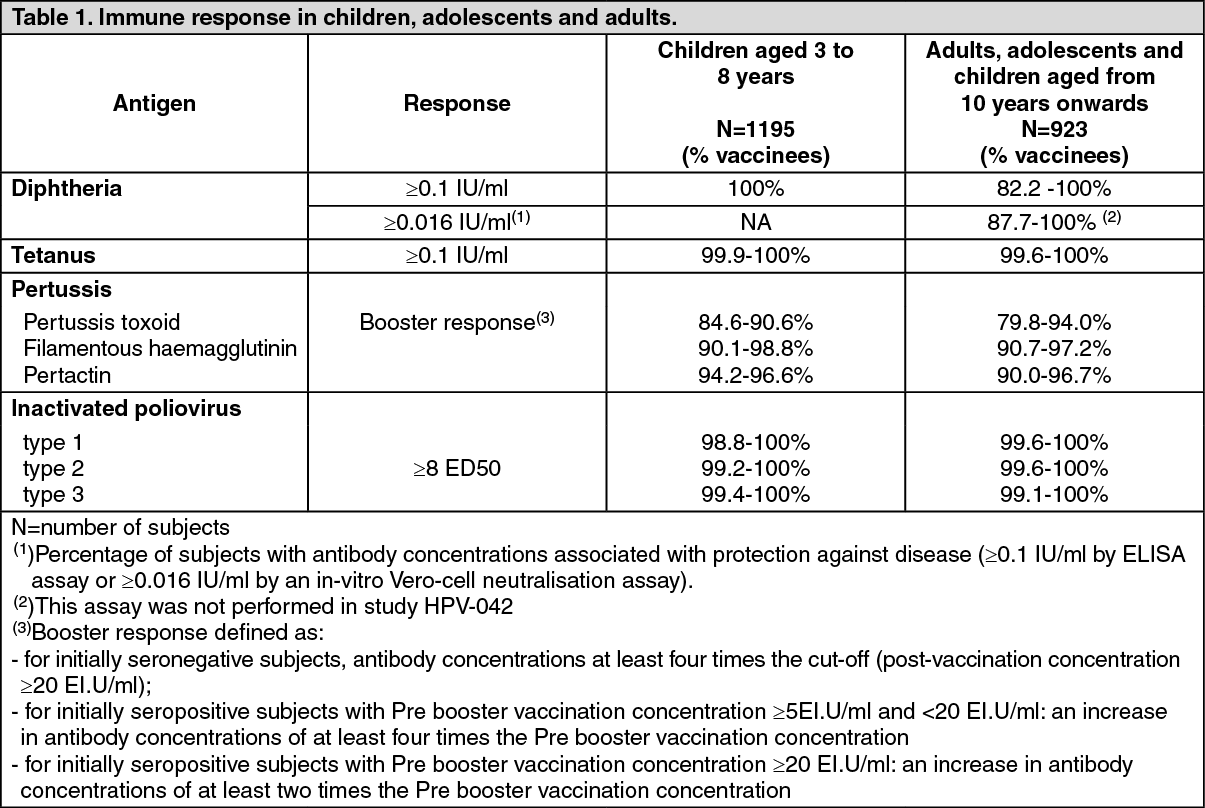
Pharmacology: Pharmacodynamics: Immune response: The immune responses to Boostrix Polio were evaluated in clinical trials carried out in subjects of different ages having different vaccination histories (see Adverse Reactions).
The following immune responses were observed across studies one month post vaccination with Boostrix Polio in children, adolescents and adults (see Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
As with other adult-type Td vaccines, Boostrix Polio induces higher seroprotection rates and higher titres of both anti-D and anti-T antibodies in children and adolescents as compared to adults.
Persistence of the immune response: The following seroprotection/seropositivity rates were observed five years after vaccination with Boostrix Polio in children and 10 years after vaccination with Boostrix Polio in adolescents and adults (see Table 2).
Click on icon to see table/diagram/image
Immune response after a repeat dose: The immunogenicity of Boostrix Polio, administered 5 years after a first booster dose of Boostrix Polio at 4 to 8 years of age, has been evaluated. One month post vaccination, >99 % of subjects were seropositive against pertussis and seroprotected against diphtheria, tetanus and all three poliovirus types.
In adults, one dose of Boostrix Polio administered 10 years after the previous dose, elicited a protective immune response in >96.8% of the subjects (for the diphtheria antigen) and in 100% of the subjects (for the tetanus and polio antigens). The booster response against the pertussis antigens was between 74.2 and 98.4%.
Immune response in subjects without prior or with unknown vaccination history: After administration of one dose of Boostrix (dTpa component of Boostrix Polio) to 83 adolescents aged from 11 to 18 years, without previous pertussis vaccination and no vaccination against diphtheria and tetanus in the previous 5 years, all subjects were seroprotected against tetanus and diphtheria. The seropositivity rate after one dose varied between 87% and 100% for the different pertussis antigens.
After administration of one dose of Boostrix Polio to 140 adults ≥40 years of age (including those who have never been vaccinated or whose vaccination status was unknown), that had not received any diphtheria and tetanus containing vaccine in the past 20 years, more than 96.4% of adults were seropositive for all three pertussis antigens and 77.7% and 95.7% were seroprotected against diphtheria and tetanus respectively.
Efficacy in protecting against pertussis: The pertussis antigens contained in Boostrix Polio are an integral part of the paediatric acellular pertussis combination vaccine (Infanrix), for which efficacy after primary vaccination has been demonstrated in a household contact efficacy study. The antibody titres to all three pertussis components following vaccination with Boostrix Polio are at least as high or higher than those observed during the household contact efficacy trial. Based on these comparisons, Boostrix Polio would provide protection against pertussis, however the degree and duration of protection afforded by the vaccine are undetermined.
Passive protection against pertussis in infants (below 3 months of age) born to mothers vaccinated during pregnancy: In a randomised, cross-over, placebo-controlled study, higher pertussis antibody concentrations were demonstrated at delivery in the cord blood of babies born to mothers vaccinated with Boostrix (dTpa group; N=291) versus placebo (control group; N=292) at 27-36 weeks of pregnancy. The cord blood geometric mean concentrations of antibodies against the pertussis antigens PT, FHA and PRN were 46.9, 366.1 and 301.8 IU/ml in the dTpa group, and 5.5, 22.7 and 14.6 IU/ml in the control group. This corresponds to antibody titres that are 8, 16 and 21 times higher in the cord blood of babies born to vaccinated mothers versus controls. These antibody titres may provide passive protection against pertussis as shown by observational effectiveness studies.
Immunogenicity in infants and toddlers born to mothers vaccinated during pregnancy: The immunogenicity of Infanrix hexa (diphtheria, tetanus, pertussis, hepatitis B, inactivated poliovirus, Haemophilus influenzae type b conjugate vaccine in infants and toddlers born to healthy mothers vaccinated with Boostrix at 27-36 weeks of pregnancy was evaluated in two clinical studies.
Infanrix hexa was co-administered with a 13-valent pneumococcal conjugate vaccine to infants for primary vaccination (n=268); and to the same infants/toddlers from 11 to 18 months as booster dose (n=229).
Post-primary and post-booster vaccination, immunological data did not show clinically relevant interference of maternal vaccination with Boostrix on the infant's and toddler's responses to diphtheria, tetanus, hepatitis B, inactivated poliovirus, Haemophilus influenzae type b or pneumococcal antigens.
Lower antibody concentrations against pertussis antigens post-primary (PT, FHA and PRN) and post-booster (PT, FHA) vaccination were observed in infants and toddlers born to mothers vaccinated with Boostrix during pregnancy. The fold-increases of anti-pertussis antibody concentrations from the pre-booster to the 1-month post-booster time point were in the same range for infants and toddlers born to mothers vaccinated with Boostrix or with placebo, demonstrating effective priming of the immune system. In the absence of correlates of protection for pertussis, the clinical relevance of these observations remains to be fully understood. However, current epidemiological data on pertussis disease following the implementation of dTpa maternal immunisation do not suggest any clinical relevance of this immune interference.
Effectiveness in the protection against pertussis disease in infants born to women vaccinated during pregnancy: Boostrix or Boostrix Polio vaccine effectiveness (VE) was evaluated in three observational studies, in UK, Spain and Australia. The vaccine was used during the third trimester of pregnancy to protect infants below 3 months of age against pertussis disease, as part of a maternal vaccination programme.
Details of each study design and results are provided in Table 3. (See Table 3.)
Click on icon to see table/diagram/image
If maternal vaccination occurs within two weeks before delivery, vaccine effectiveness in the infant may be lower than the figures in the table.
Pharmacokinetics: Evaluation of pharmacokinetic properties is not required for vaccines.
Toxicology: Preclinical safety data: Reproductive toxicology: Fertility: Non-clinical data obtained with Boostrix Polio reveal no specific hazard for humans based on conventional studies of female fertility in rats and rabbits.
Pregnancy: Non-clinical data obtained with Boostrix Polio reveal no specific hazard for humans based on conventional studies of embryo-foetal development in rats and rabbits, and also of parturition and postnatal toxicity in rats (up to the end of the lactation period).
Animal toxicology and/or pharmacology: Preclinical data reveal no special hazard for humans based on conventional studies of safety and of toxicity.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image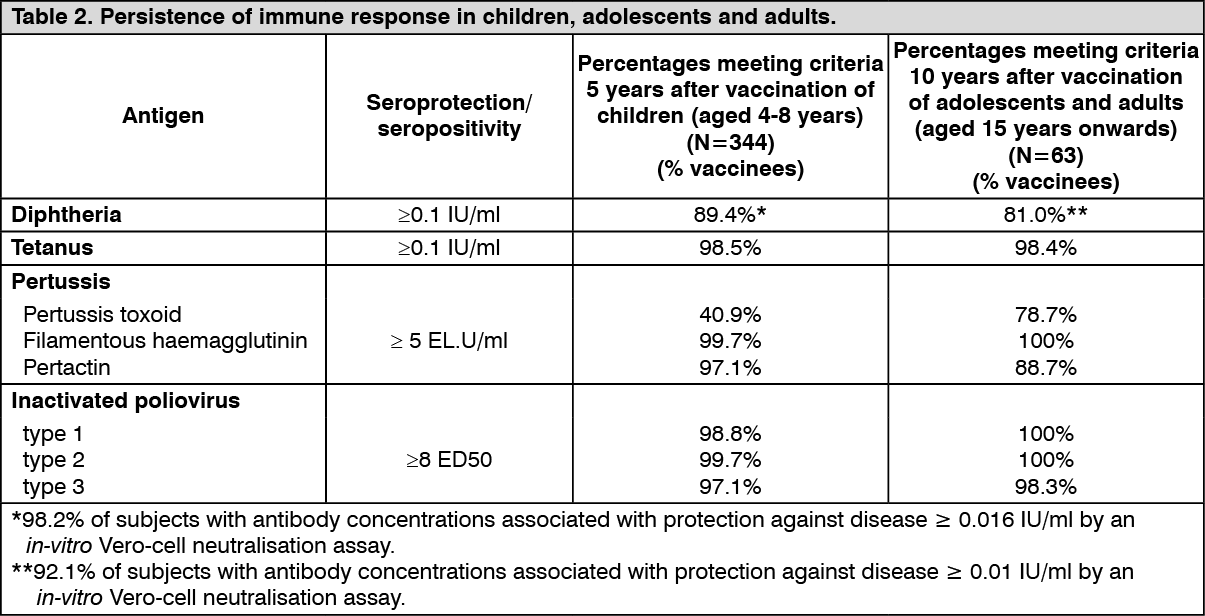 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image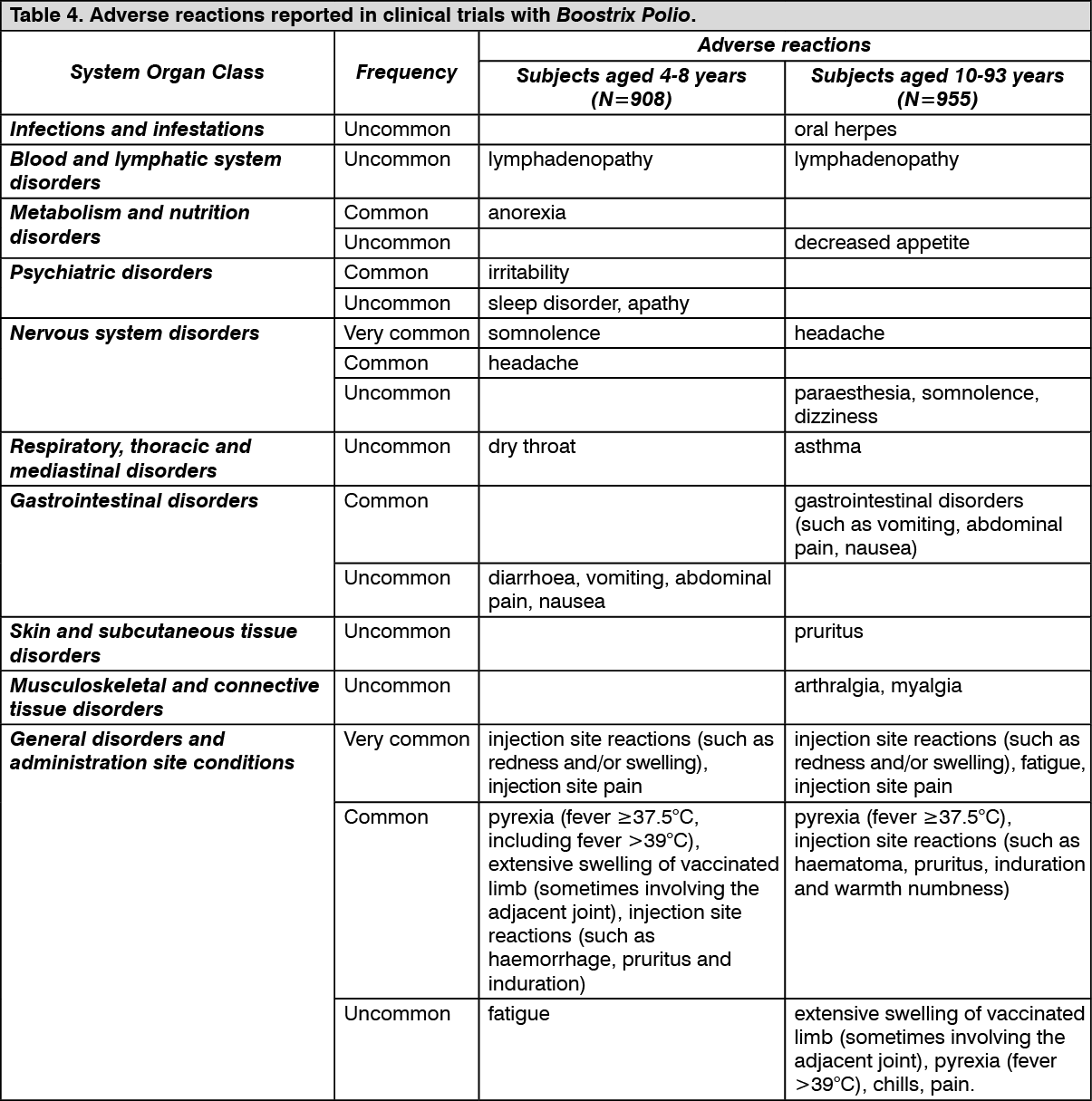 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image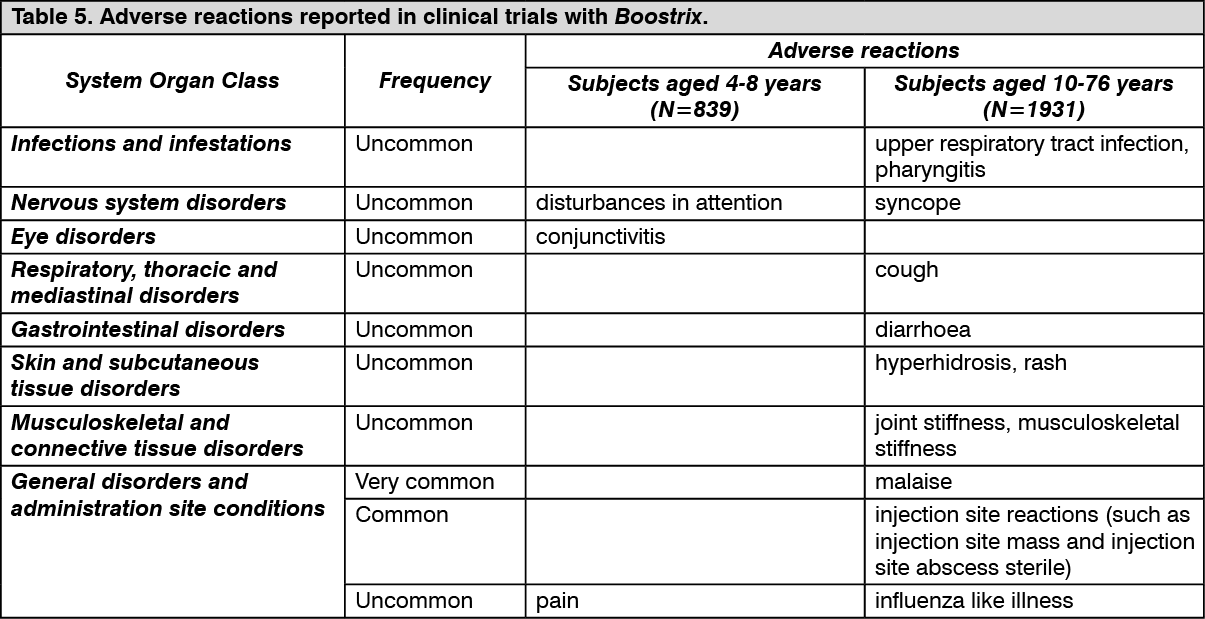 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image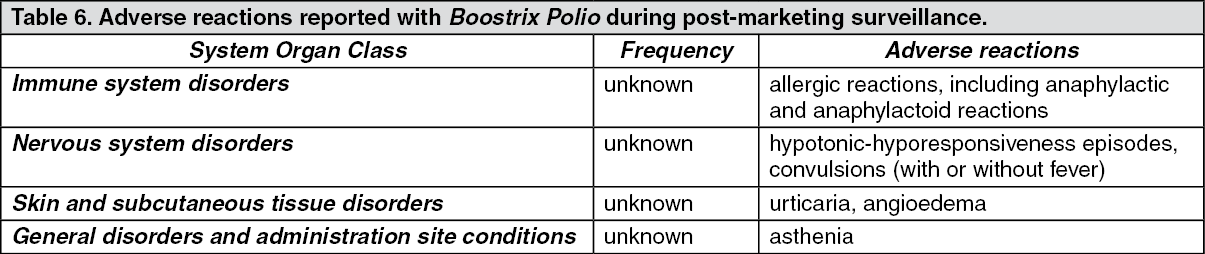 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
