Pharmacotherapeutic group: Drugs used in diabetes, glucagon-like peptide-1 (GLP-1) analogues.
ATC code: A10BJ01.
Pharmacology: Pharmacodynamics: Mechanism of action: Exenatide is a glucagon-like peptide-1 (GLP-1) receptor agonist that exhibits several antihyperglycaemic actions of glucagon-like peptide-1 (GLP-1). The amino acid sequence of exenatide partially overlaps that of human GLP-1. Exenatide has been shown to bind to and activate the known human GLP-1 receptor
in vitro, its mechanism of action mediated by cyclic AMP and/or other intracellular signalling pathways.
Exenatide increases, on a glucose-dependent basis, the secretion of insulin from pancreatic beta cells. As blood glucose concentrations decrease, insulin secretion subsides. When exenatide was used in combination with metformin and/or a thiazolidinedione, no increase in the incidence of hypoglycaemia was observed over that of placebo in combination with metformin and/or a thiazolidinedione which may be due to this glucose-dependent insulinotropic mechanism (see Precautions).
Exenatide suppresses glucagon secretion which is known to be inappropriately elevated in patients with type 2 diabetes. Lower glucagon concentrations lead to decreased hepatic glucose output. However, exenatide does not impair the normal glucagon response and other hormone responses to hypoglycaemia.
Exenatide slows gastric emptying, thereby reducing the rate at which meal-derived glucose appears in the circulation.
Administration of exenatide has been shown to reduce food intake, due to decreased appetite and increased satiety.
Pharmacodynamic effects: Exenatide improves glycaemic control through the sustained effects of lowering both postprandial and fasting glucose concentrations in patients with type 2 diabetes. Unlike native GLP-1, prolonged-release exenatide has a pharmacokinetic and pharmacodynamic profile in humans suitable for once weekly administration.
A pharmacodynamic study with exenatide demonstrated in patients with type 2 diabetes (n = 13) a restoration of first phase insulin secretion and improved second phase insulin secretion in response to an intravenous bolus of glucose.
Clinical efficacy and safety: The results of two studies with Bydureon BCise and six long-term clinical studies of prolonged-release exenatide are presented as follows; these studies comprised 1766 subjects (556 treated with Bydureon BCise), 53 % men and 47 % women, 304 subjects (17 %) were ≥ 65 years of age.
In addition, a double-blind, placebo-controlled cardiovascular outcome study (EXSCEL) enrolled 14,752 subjects with type 2 diabetes and any level of CV risk when added to the current usual care.
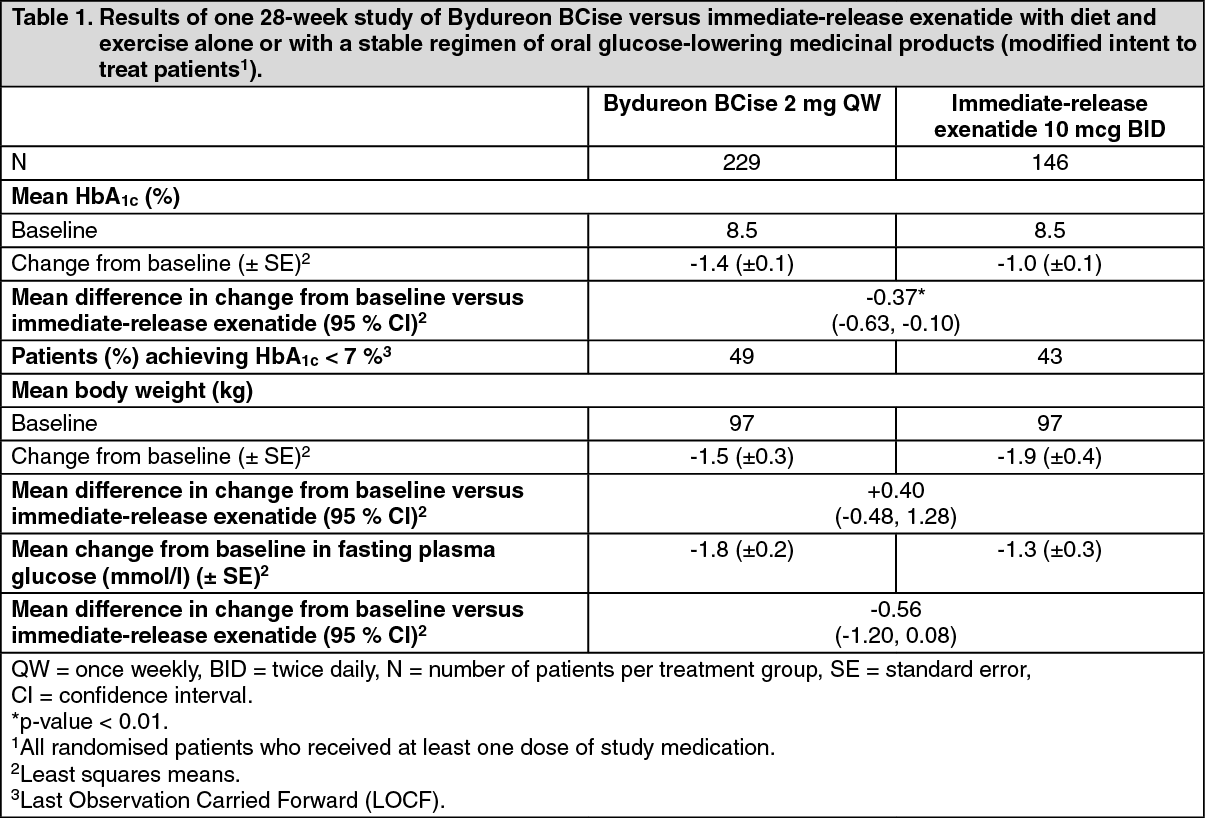
Glycaemic control: Bydureon BCise: In a 28-week open-label study, Bydureon BCise was compared to immediate-release exenatide in subjects on a diet and exercise programme alone or with a stable regimen of oral glucose-lowering medicinal products. Both treatment groups had a reduction in HbA
1c compared to baseline. Bydureon BCise demonstrated superiority to immediate-release exenatide in reducing HbA
1c from baseline to Week 28 (Table 1). The 28-week comparator-controlled period of the study was followed by a 24-week extension period during which all participating subjects received treatment with this medicinal product. The effect on HbA
1c remained clinically significant over 52 weeks but partially diminished over time in the group that had initially received Bydureon BCise.
Both Bydureon BCise and immediate-release exenatide patients achieved a reduction in weight at Week 28 compared to baseline (Table 1). The difference between the two treatment groups was not significant. The reductions in body weight were sustained at Week 52. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In a 28-week open-label study (oral medication-blinded), Bydureon BCise was compared to sitagliptin and placebo in subjects also using metformin ≥ 1,500 mg daily. Bydureon BCise demonstrated superiority to both sitagliptin and placebo in reducing HbA
1c from baseline to Week 28 (Table 2).
Both Bydureon BCise and sitagliptin patients achieved a reduction in weight at Week 28 compared to baseline (Table 2). The difference between the two treatment groups was not significant. (See Table 2.)
Click on icon to see table/diagram/image
Prolonged-release exenatide: In two studies prolonged-release exenatide 2 mg once weekly has been compared to immediate-release exenatide 5 mcg given twice daily for 4 weeks followed by immediate-release exenatide 10 mcg given twice daily. One study was of 24 weeks in duration (n = 252) and the other of 30 weeks (n = 295) followed by an open labelled extension where all patients were treated with prolonged-release exenatide 2 mg once weekly, for a further 7 years (n = 258). In both studies, decreases in HbA
1c were evident in both treatment groups as early as the first post-treatment HbA
1c measurement (Weeks 4 or 6).
Prolonged-release exenatide resulted in a statistically significant reduction in HbA
1c compared to patients receiving immediate-release exenatide (Table 3).
A clinically relevant effect of prolonged-release exenatide and immediate-release exenatide treated subjects was observed on HbA
1c, regardless of the background anti-diabetic therapy in both studies.
Clinically and statistically significantly more subjects on prolonged-release compared to immediate-release exenatide patients achieved an HbA
1c reduction of ≤ 7 % or < 7 % in the two studies (p < 0.05 and p ≤ 0.0001 respectively).
Both prolonged-release and immediate-release exenatide patients achieved a reduction in weight compared to baseline, although the difference between the two treatment arms was not significant.
In the uncontrolled study extension, evaluable patients who switched from immediate release to prolonged-release exenatide at week 30 (n = 121), achieved the same improvement in HbA
1c of -2.0 % at Week 52 compared to baseline as patients treated with prolonged-release exenatide. For all patients completing the uncontrolled study extension of 7 years (n = 122 of 258 patients included in the extension phase), HbA
1c gradually increased over time from week 52 onwards, but was still reduced compared to baseline after 7 years -1.5%). Weight loss was sustained over 7 years in these patients. (See Table 3.)
Click on icon to see table/diagram/image
A study of 26-week duration has been conducted, in which prolonged-release exenatide 2 mg is compared to insulin glargine once daily. Compared with insulin glargine treatment, prolonged-release exenatide demonstrated a superior change in HbA
1c, significantly lowered mean body weight and was associated with fewer hypoglycaemic events (Table 4). (See Table 4.)
Click on icon to see table/diagram/image
The 156-week results were consistent with those previously reported in the 26-week interim report. Treatment with prolonged-release exenatide persistently significantly improved glycaemic control and weight control, compared to the insulin glargine treatment. Safety findings at 156 weeks were consistent with those reported at 26 weeks.
In a 26-week double-blind study prolonged-release exenatide was compared to maximum daily doses of sitagliptin and pioglitazone in subjects also using metformin. All treatment groups had a significant reduction in HbA
1c compared to baseline. Prolonged-release exenatide demonstrated superiority to both sitagliptin and pioglitazone with respect to change in HbA
1c from baseline.
Prolonged-release exenatide demonstrated significantly greater weight reductions compared to sitagliptin. Patients on pioglitazone gained weight (Table 5). (See Table 5.)
Click on icon to see table/diagram/image
In a 28-week, double-blind study, the combination of prolonged-release exenatide and dapagliflozin was compared to prolonged-release exenatide alone and dapagliflozin alone in subjects also using metformin. All treatment groups had a reduction in HbA
1c compared to baseline. The prolonged-release exenatide and dapagliflozin treatment group showed superior reductions in HbA
1c from baseline compared to prolonged-release exenatide alone and dapagliflozin alone (Table 6).
The combination of prolonged-release exenatide and dapagliflozin demonstrated significantly greater weight reductions compared to either medicinal product alone (Table 6). (See Table 6.)
Click on icon to see table/diagram/image
In a 28-week double-blind study, prolonged-release exenatide added to insulin glargine alone or with metformin was compared to placebo added to insulin glargine alone or with metformin. Insulin glargine was dosed targeting a fasting plasma glucose of 4.0 to 5.5 mmol/L (72 to 99 mg/dL). Prolonged-release exenatide demonstrated superiority to placebo in reducing HbA
1c from baseline to Week 28 (Table 7).
Prolonged-release exenatide was superior to placebo in reducing body weight at Week 28 (Table 7). (See Table 7.)
Click on icon to see table/diagram/image
Cardiovascular evaluation: EXSCEL was a pragmatic cardiovascular (CV) outcome study in patients with type 2 diabetes and any level of CV risk. A total of 14,752 patients were randomized 1:1 to either prolonged-release exenatide 2mg once weekly or placebo, added to the current usual care which could include SGLT2 inhibitors. Patients were followed as in routine clinical practice for a median of 38.7 months with a median treatment duration of 27.8 months. The vital status was known at the end of the study for 98.9% and 98.8% of the patients in the prolonged-release exenatide and placebo group, respectively. The mean age at study entry was 62 years (with 8.5% of the patients ≥ 75 years). Approximately 62% of the patients were male. The mean BMI was 32.7 kg/m
2 and the mean duration of diabetes was 13.1 years. The mean HbA
1c was 8.1%. Approximately 49.3% had mild renal impairment (estimated glomerular filtration rate [eGFR] ≥ 60 to ≤ 89 mL/min/1.73 m
2) and 21.6% had moderate renal impairment (eGFR ≥ 30 to ≤ 59 mL/min/1.73 m
2). Overall, 26.9% of patients did not have any prior CV event, 73.1% had at least one prior CV event.
The primary safety (noninferiority) and efficacy (superiority) endpoint in EXSCEL was the time to first confirmed Major Adverse Cardiac Event (MACE): cardiovascular (CV)-related death, nonfatal myocardial infarction (MI) or nonfatal stroke. All-cause mortality was the initial secondary endpoint assessed.
Prolonged-release exenatide did not increase the cardiovascular risk in patients with type 2 diabetes mellitus compared to placebo when added to current usual care (HR:0.91; 95% CI: 0.832, 1.004; P<0.001 for non-inferiority) see Figure 1.
In a pre-specified subgroup analysis in EXSCEL, the HR for MACE was 0.86 (95% CI: 0.77-0.97) in patients with baseline eGFR ≥ 60 mL/min/1.73 m2 and 1.01 (95% CI: 0.86-1.19) in patients with baseline eGFR < 60 mL/min/1.73 m2. The results of the primary composite and secondary cardiovascular endpoints are shown in Figure 2. (See Figures 1 and 2.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The need for additional antihyperglycaemic medication was reduced by 33% with the prolonged-release exenatide group (exposure-adjusted incidence of 10.5 per 100 pt-year) compared to the placebo group (exposure-adjusted incidence of 15.7 per 100 pt-year). A reduction in HbA
1c was observed over the course of the trial with an overall treatment difference of -0.53% (prolonged-release exenatide vs. placebo).
Body weight: A reduction in body weight compared to baseline has been observed in studies with prolonged-release exenatide formulations. This reduction in body weight was seen irrespective of the occurrence of nausea although the reduction was larger in the group with nausea (mean reduction of -1.9 kg to -5.2 kg with nausea versus -1.0 kg to -2.9 kg without nausea).
Plasma/serum glucose: Treatment with prolonged-release exenatide resulted in significant reductions in fasting plasma/serum glucose concentrations, these reductions were observed as early as 4 weeks. In the placebo-controlled study with insulin glargine, the change from baseline to Week 28 in fasting plasma glucose was -0.7 mmol/L for the prolonged-release exenatide group and -0.1 mmol/L for the placebo group. Additional reductions in postprandial concentrations were also observed.
For both prolonged-release exenatide formulations, the improvement in fasting plasma glucose concentrations was sustained through 52 weeks.
Beta-cell function: Clinical studies with prolonged-release exenatide formulations have indicated improved beta-cell function, using measures such as the homeostasis model assessments (HOMA-B). The effect on beta-cell function was sustained through 52 weeks.
Blood pressure: A reduction in systolic blood pressure was observed in the studies with prolonged-release exenatide formulations (0.8 mmHg to 4.7 mmHg). In the 30-week immediate-release exenatide comparator study both prolonged-release and immediate-release exenatide significantly reduced systolic blood pressure from baseline (4.7±1.1 mmHg and 3.4±1.1 mmHg respectively); the difference between the treatments was not significant. Improvements in blood pressure were maintained through 52 weeks.
In the placebo-controlled study with insulin glargine, the change from baseline to Week 28 in systolic blood pressure was -2.6 mmHg for the prolonged-release exenatide group and -0.7 mmHg for the placebo group.
Treatment with prolonged-release exenatide and dapagliflozin combination at Week 28 resulted in a significant mean change reduction of -4.3±0.8 mmHg in systolic blood pressure compared to prolonged-release exenatide alone of -1.2±0.8 mmHg (p<0.01) or to dapagliflozin alone of -1.8±0.8 mmHg (p<0.05).
Fasting lipids: The prolonged-release exenatide formulations have shown no negative effects on lipid parameters.
Paediatric population: The European Medicines Agency has deferred the obligation to submit the results of studies with prolonged-release exenatide formulations in one or more subsets of the paediatric population in type 2 diabetes mellitus (see Dosage & Administration for information on paediatric use).
Pharmacokinetics: The absorption properties of exenatide reflect the extended release properties of the prolonged-release exenatide formulation. Once absorbed into the circulation, exenatide is distributed and eliminated according to its known systemic pharmacokinetic properties (as described as follows).
Absorption: Following weekly administration of 2 mg Bydureon BCise, mean exenatide concentrations exceeded minimal efficacious concentrations (~ 50 pg/mL) in 2 weeks with gradual increase in the average plasma exenatide concentration up to Week 8. Subsequently, exenatide concentrations of approximately 153-208 pg/mL were maintained, indicating that steady state was achieved. Steady-state exenatide concentrations are maintained during the one-week interval between doses with minimal peak to trough fluctuation from this average therapeutic concentration.
Distribution: The mean apparent volume of distribution of exenatide following subcutaneous administration of a single dose of exenatide is 28 L.
Biotransformation and elimination: Nonclinical studies have shown that exenatide is predominantly eliminated by glomerular filtration with subsequent proteolytic degradation. The mean apparent clearance of exenatide is 9 L/h. These pharmacokinetic characteristics of exenatide are independent of the dose. Approximately 10 weeks after discontinuation of prolonged-release exenatide therapy, mean plasma exenatide concentrations fell below minimal detectable concentrations.
Special populations: Renal impairment: No clinically meaningful differences were observed in steady state exenatide concentrations or tolerability in patients with mild to moderate renal impairment (eGFR 30 to 89 mL/min/1.73m
2) receiving Bydureon BCise, compared to those with normal renal function.
Hepatic insufficiency: No pharmacokinetic study has been performed in patients with hepatic insufficiency. Exenatide is cleared primarily by the kidney; therefore hepatic dysfunction is not expected to affect blood concentrations of exenatide.
Gender, race and body weight: Gender, race and body weight have no clinically relevant influence on exenatide pharmacokinetics.
Elderly: Data in elderly are limited, but suggest no marked changes in exenatide exposure with increased age up to about 75 years old.
In a pharmacokinetic study of immediate-release exenatide in patients with type 2 diabetes, administration of exenatide (10 mcg) resulted in a mean increase of exenatide AUC by 36 % in 15 elderly subjects aged 75 to 85 years compared to 15 subjects aged 45 to 65 years likely related to reduced renal function in the older age group (see Dosage & Administration).
Paediatric population: In a single-dose pharmacokinetic study of immediate-release exenatide in 13 patients with type 2 diabetes and between the ages of 12 and 16 years, administration of exenatide (5 mcg) resulted in slightly lower mean AUC (16 % lower) and C
max (25 % lower) compared to those observed in adults. No pharmacokinetics study of prolonged-release exenatide has been conducted in the paediatric population.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazards for humans based on conventional studies of safety pharmacology, repeat-dose toxicity, or genotoxicity conducted with immediate-release exenatide or prolonged-release exenatide formulations.
Thyroid tumours have been observed in rats and mice with long acting GLP-1 receptor agonists. In a 2-year rat carcinogenicity study with prolonged-release exenatide, an increased incidence of C-cell adenomas and C-cell carcinomas was observed at doses ≥ 2-fold the human systemic exposure based on AUC. The clinical relevance of these findings is currently unknown.
Animal studies with exenatide did not indicate harmful effects with respect to fertility; high doses of exenatide caused skeletal effects and reduced foetal and neonatal growth.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image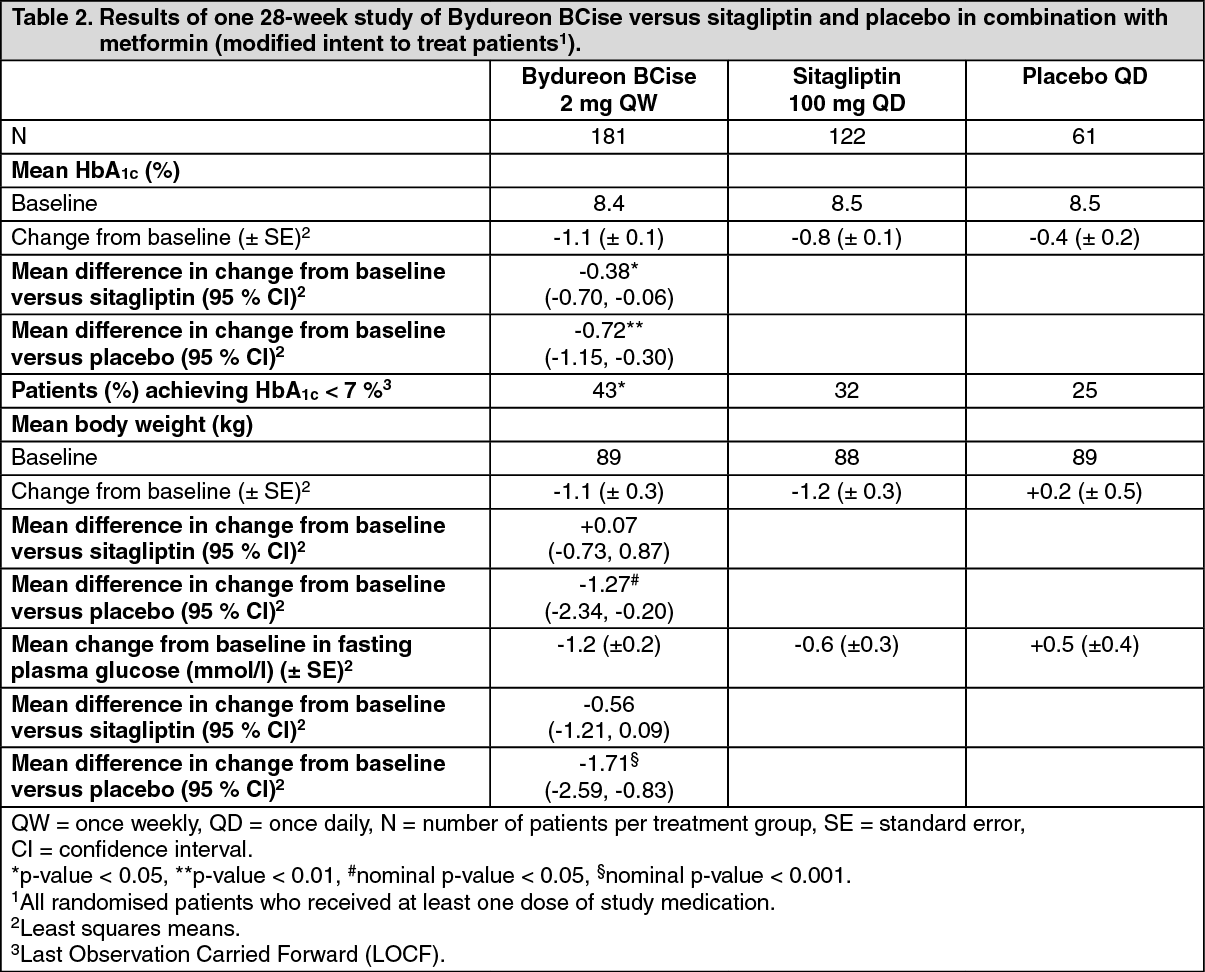 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image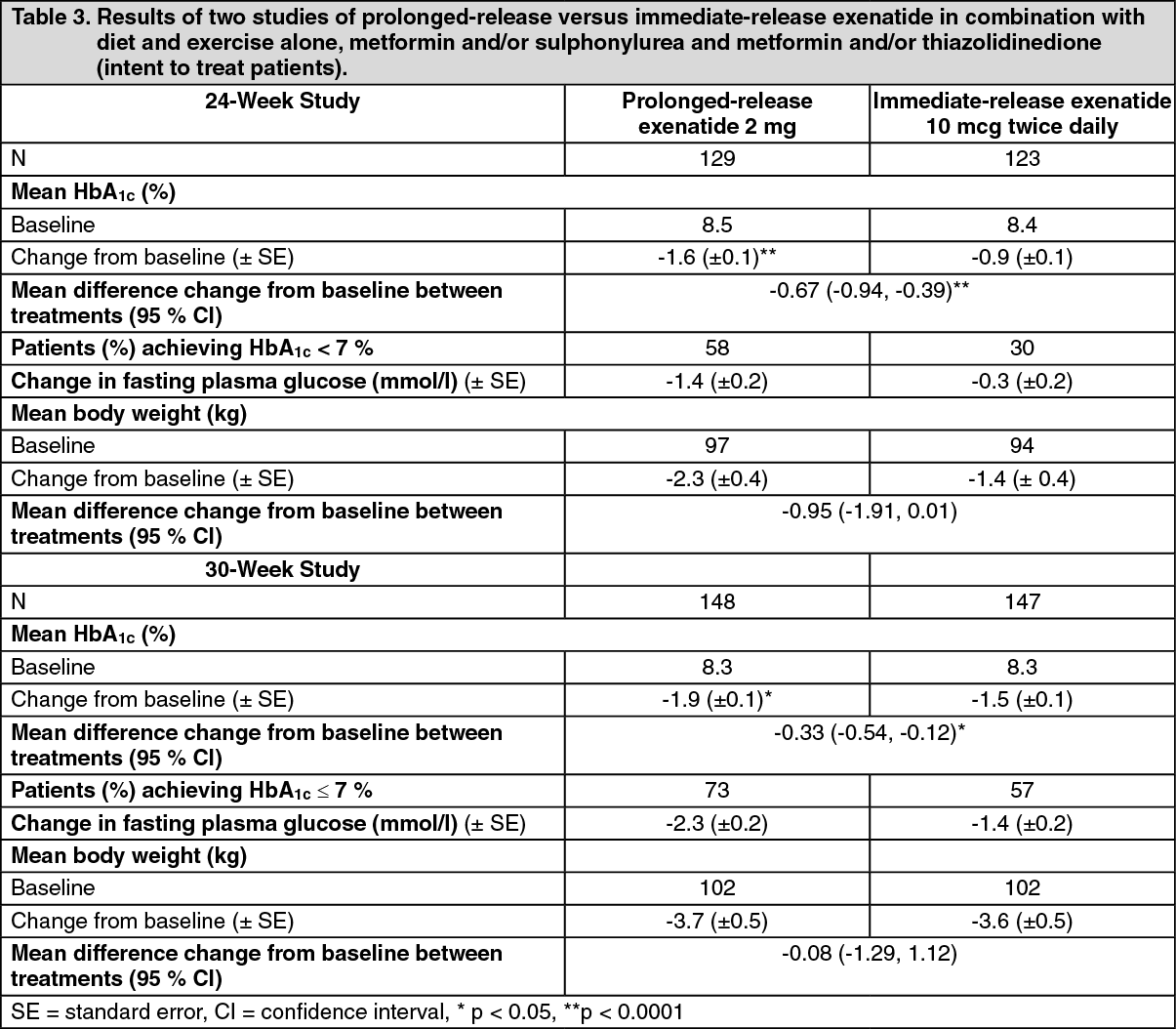 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image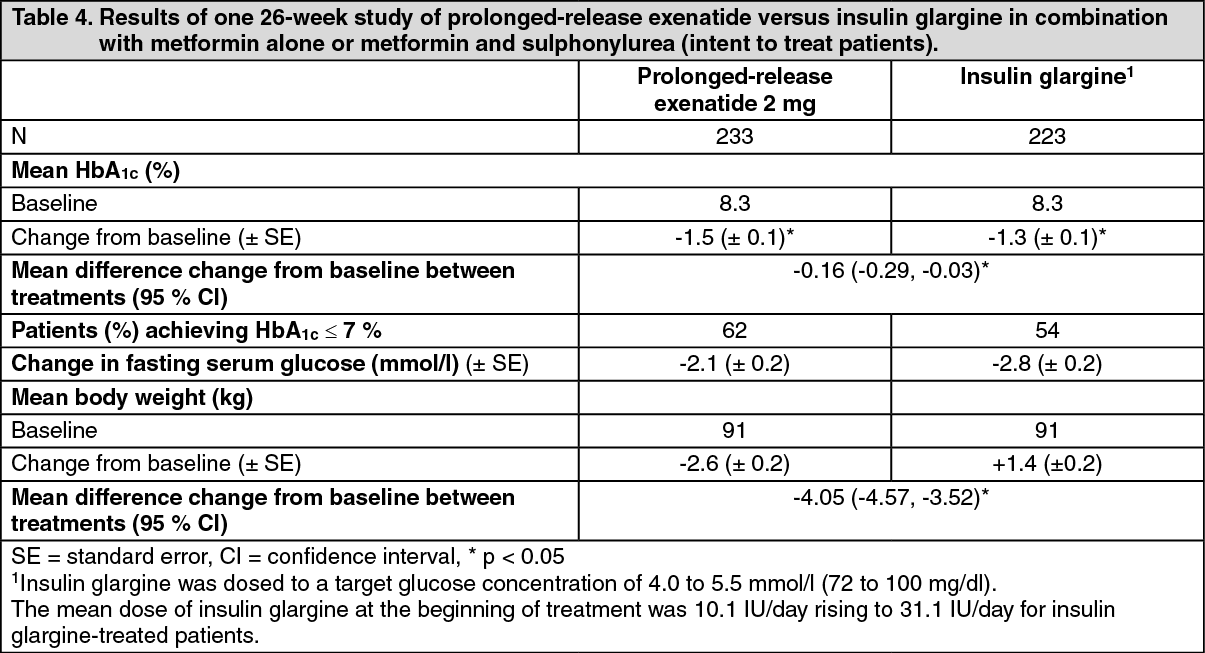 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image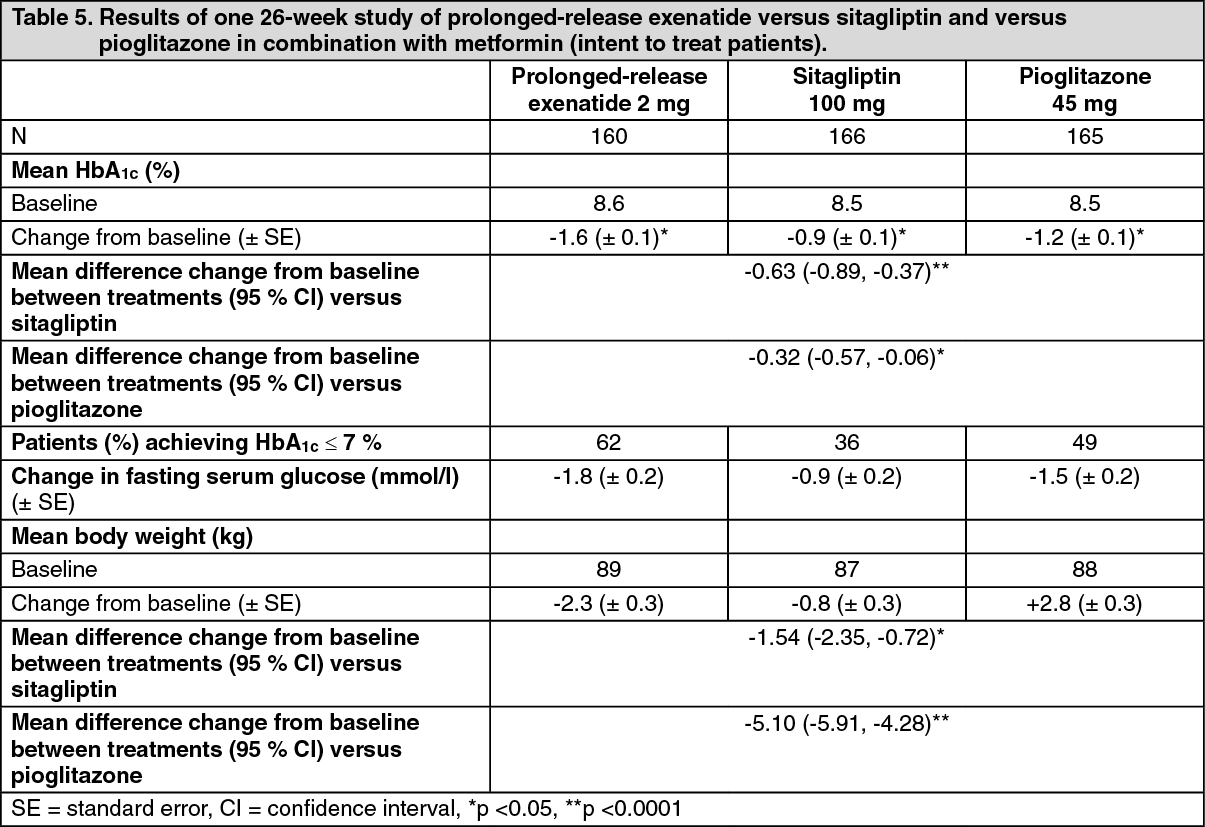 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image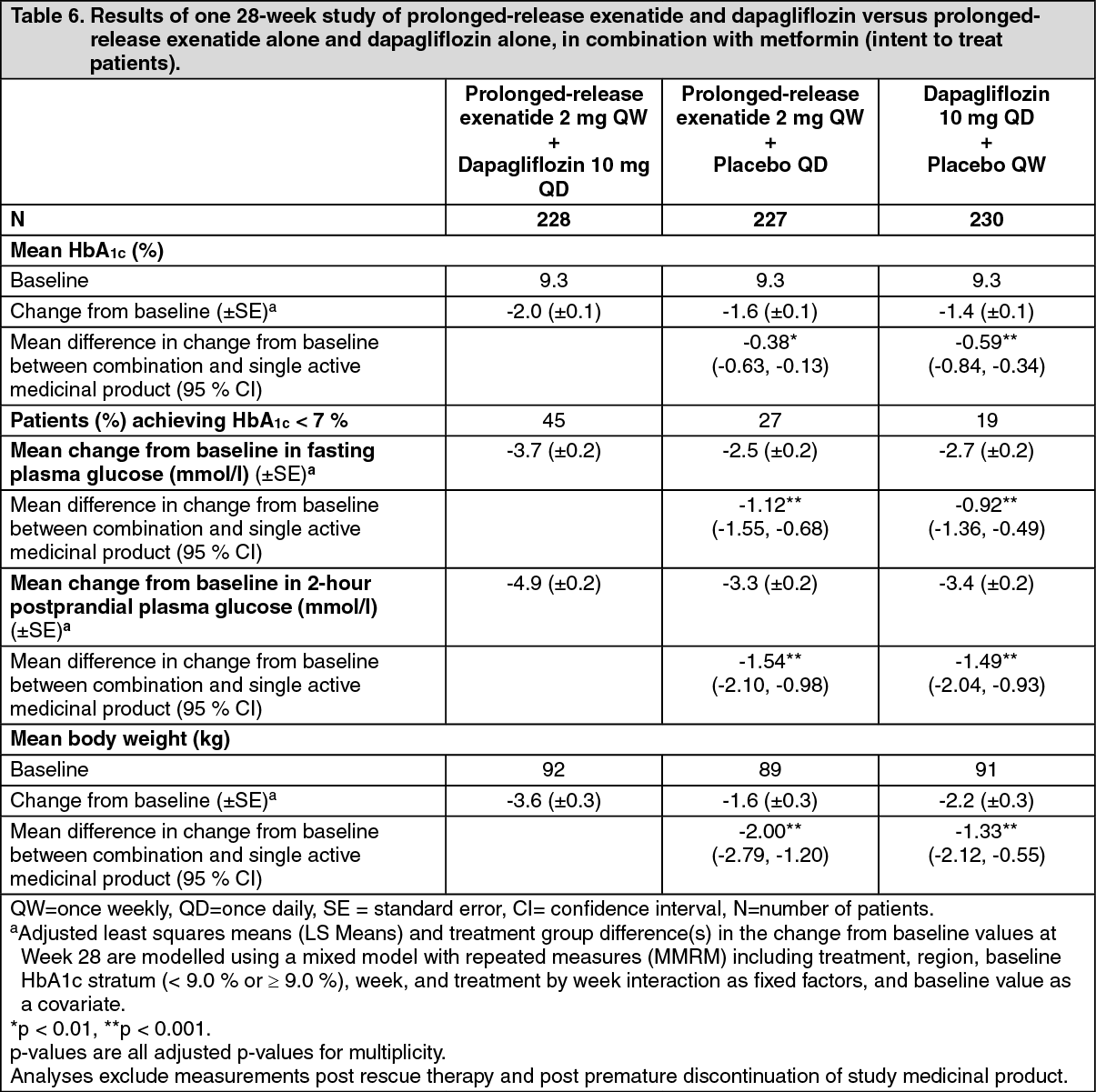 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image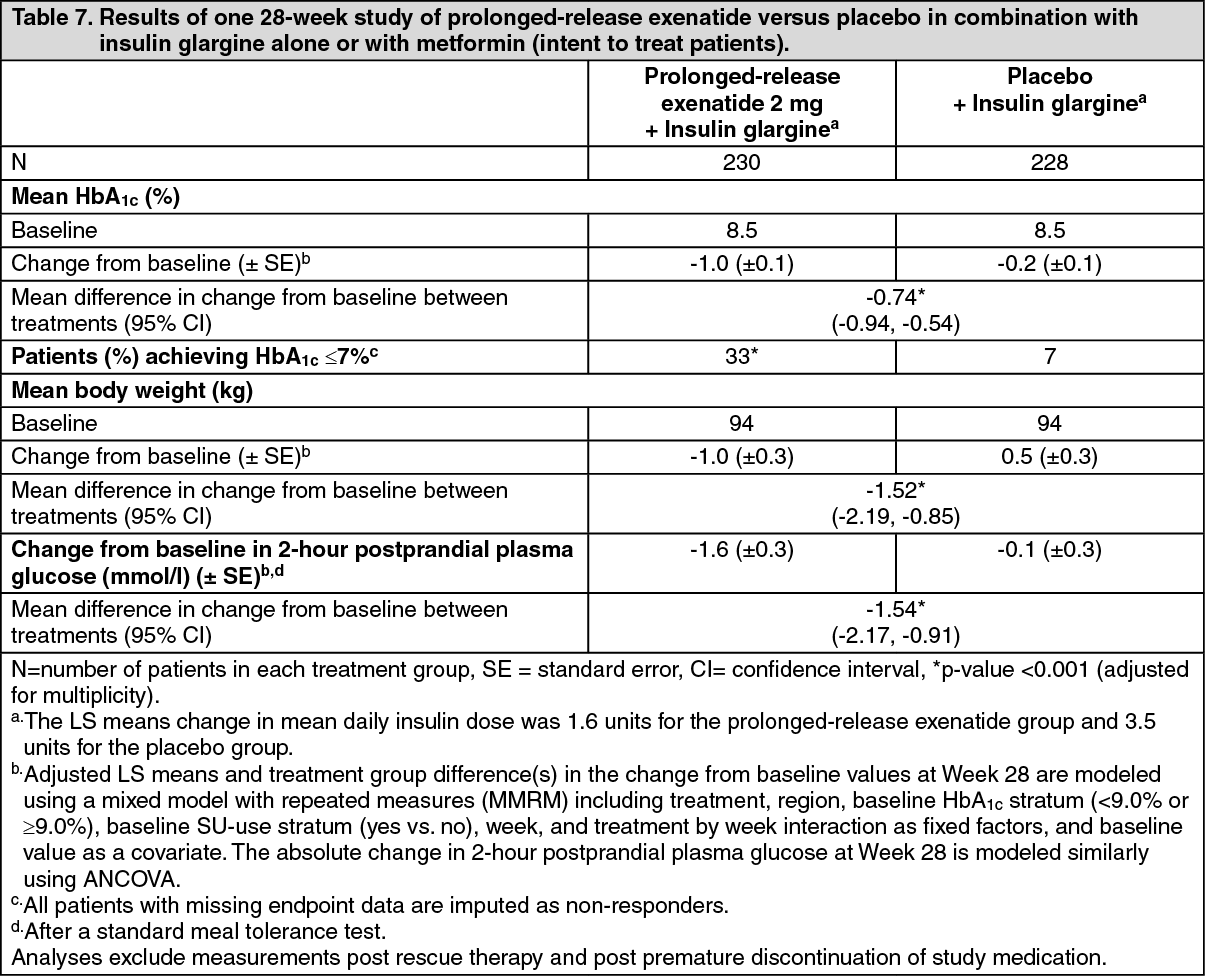 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image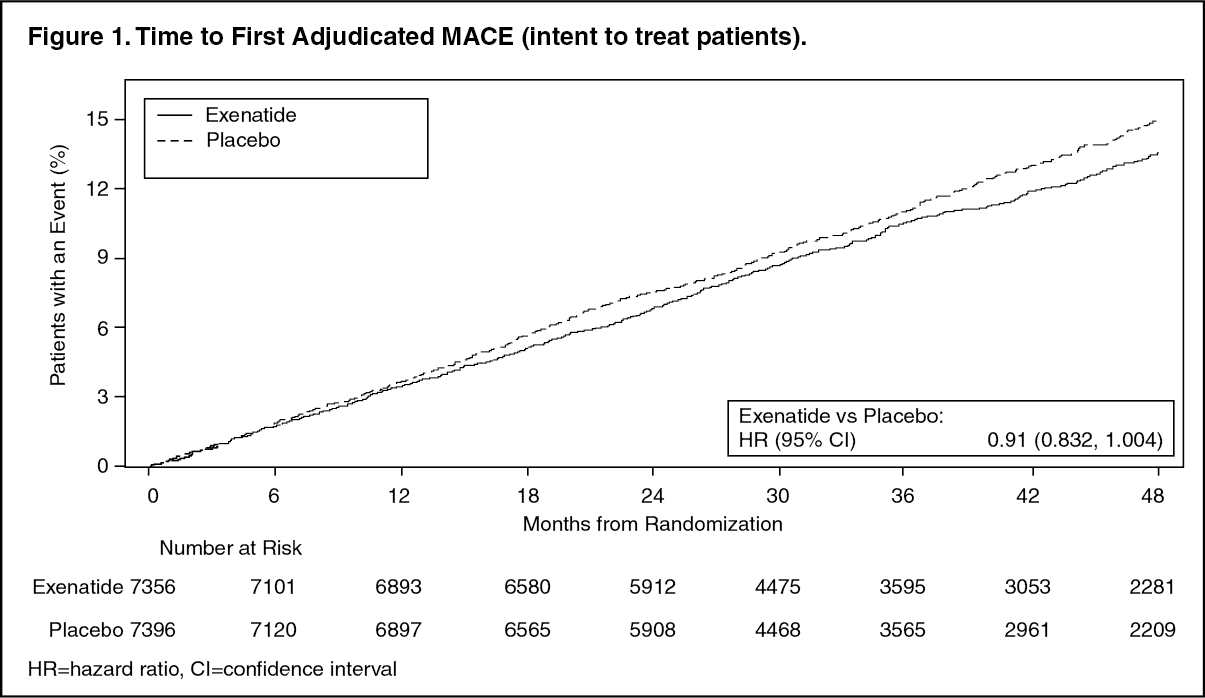 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image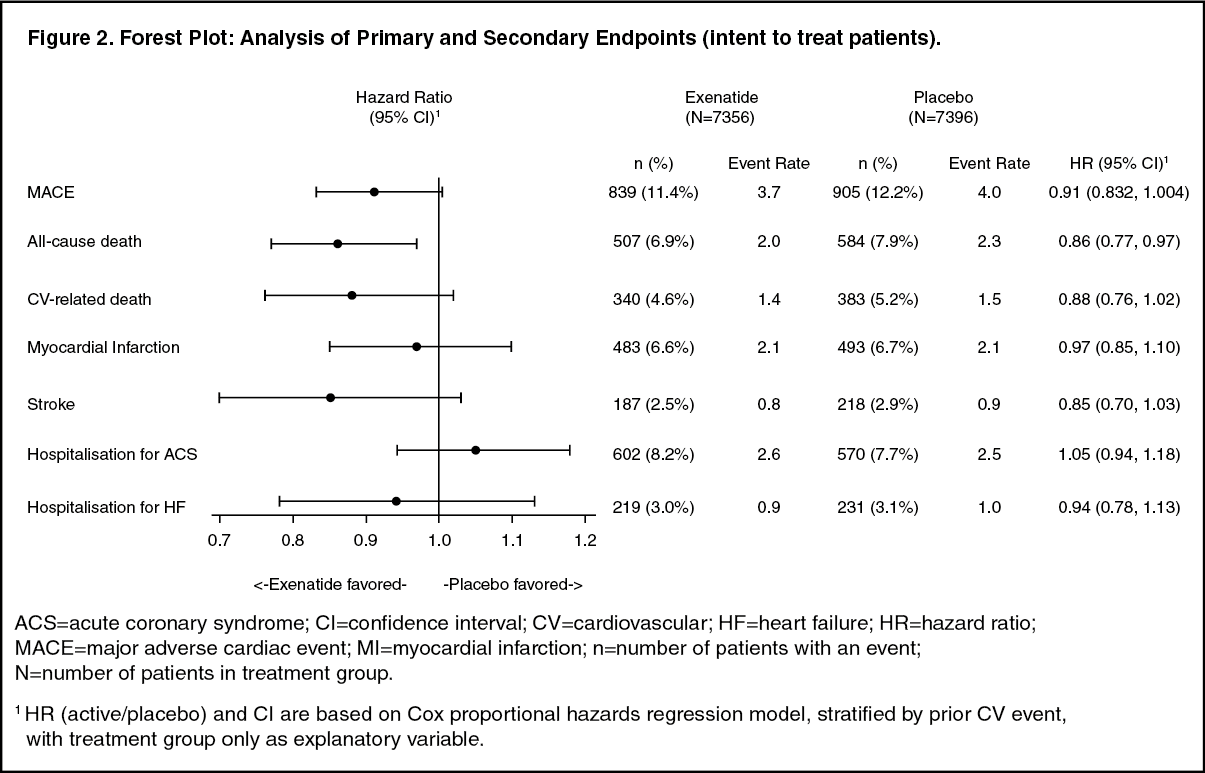 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out