The following undesirable effects have been reported for enalapril: Very common (≥ 1/10); common (≥ 1/100 to < 1/10); uncommon (≥ 1/1,000 to < 1/100); rare (≥ 1/10,000 to < 1/1,000); very rare (< 1/10,000), not known (cannot be estimated from the available data).
Blood and the lymphatic system disorders: Uncommon: Anaemia (including aplastic and haemolytic).
Rare: Neutropenia, decreases in haemoglobin, decreases in haematocrit, thrombocytopenia, agranulocytosis, bone marrow depression, pancytopenia, lymphadenopathy, autoimmune diseases.
Endocrine disorders: Not Known: Syndrome of inappropriate antidiuretic hormone secretion (SIADH).
Metabolism and nutrition disorders: Uncommon: Hypoglycaemia.
Psychiatric disorders: Common: Depression.
Uncommon: Confusion, insomnia, nervousness.
Rare: Dream abnormality, sleep disorders.
Nervous system disorders: Very common: Dizziness.
Common: Headache, syncope, taste alteration.
Uncommon: Somnolence, paresthesia, vertigo.
Eye disorders: Very common: Blurred vision.
Ear and Labyrinth disorders: Uncommon: Tinnitus.
Cardiac disorders: Common: Chest pain, rhythm disturbances, angina pectoris, tachycardia.
Uncommon: Palpitations, myocardial infarction or cerebrovascular accident
#, possibly secondary to excessive hypotension in high risk patients.
#Incidence rates were comparable to those in the placebo and active control groups in the clinical trials.
Vascular disorders: Common: Hypotension (including orthostatic hypotension).
Uncommon: Flushing, orthostatic hypotension.
Rare: Raynaud's phenomenon.
Respiratory thoracic and mediastinal disorders: Very common: Cough.
Common: Dyspnea.
Uncommon: Rhinorrhea, sore throat and hoarseness, bronchospasm/asthma.
Rare: Pulmonary infiltrates, rhinitis, allergic alveolitis/eosinophilia pneumonia.
Gastro-intestinal disorders: Very common: Nausea.
Common: Diarrhoea, abdominal pain.
Uncommon: Ileus, pancreatitis, vomiting, dyspepsia, constipation, anorexia, gastric irritations, dry mouth, peptic ulcer.
Rare: Stomatitis/aphthous ulcerations, glossitis.
Very rare: Intestinal angioedema.
Hepatobiliary disorders: Rare: Hepatic failure, hepatitis - either hepatocellular or cholestatic hepatitis including necrosis, cholestasis (including jaundice).
Skin and subcutaneous tissue disorders: Common: Rash, hypersensitivity/angioneurotic oedema: angioneurotic oedema of the face, extremities, lips, tongue, glottis and/or larynx has been reported.
Uncommon: Diaphoresis, pruritus, urticaria, alopecia.
Rare: Erythema multiforme, Stevens-Johnson syndrome, exfoliative dermatitis, toxic epidermal necrolysis, pemphigus, erythroderma.
Not known: A symptom complex has been reported which may include some or all of the following: fever, serositis, vasculitis, myalgia/myositis, arthralgia/arthritis, a positive ANA (Antinuclear Antibodies), elevated ESR (Erythrocyte Sedimentation Rate), eosinophilia, and leuko-cytosis. Rash, photosensitivity or other dermatologic manifestations may occur.
Musculoskeletal, connective tissue, and bone disorders: Uncommon: Muscle cramps.
Renal and urinary disorders: Uncommon: Renal dysfunction, renal failure, proteinuria.
Rare: Oliguria.
Reproductive system and breast disorders: Uncommon: Impotence.
Rare: Gynecomastia.
General disorders and administration site conditions: Very common: Asthenia.
Common: Fatigue.
Uncommon: Malaise, fever.
Investigations: Common: Hyperkalaemia, increases in serum creatinine.
Uncommon: Increases in blood urea, hyponatremia.
Rare: Elevations of liver enzymes, elevations of serum bilirubin.


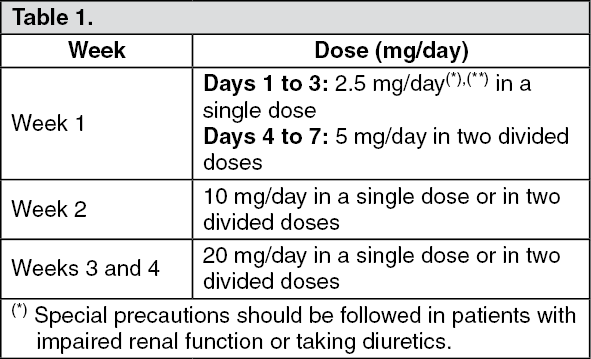 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image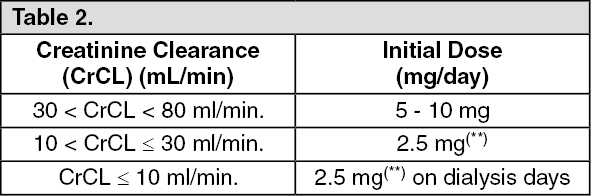 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out