Each film coated tablet contains Exemestane 25 mg.
Excipients/Inactive Ingredients: Mannitol, Copovidone, Crospovidone, Microcrystalline cellulose, Sodium Starch Glycolate, Magnesium stearate, Hypromellose, Macrogol 400 and Titanium Dioxide.
Pharmacotherapeutic group: hormone antagonists and related agents, enzyme inhibitors. ATC: L02BG06.
Pharmacology: Pharmacodynamics: Exemestane is an irreversible, steroidal aromatase inhibitor, structurally related to the natural substrate androstenedione. In post-menopausal women, oestrogens are produced primarily from the conversion of androgens into oestrogens through the aromatase enzyme in peripheral tissues. Oestrogen deprivation through aromatase inhibition is an effective and selective treatment for hormone dependent breast cancer in postmenopausal women. In postmenopausal women, Exemestane significantly lowered serum oestrogen concentrations starting from a 5 mg dose, reaching maximal suppression (>90%) with a dose of 10-25 mg. In postmenopausal breast cancer patients treated with the 25 mg daily dose, whole body aromatization was reduced by 98%.
Exemestane does not possess any progestogenic or oestrogenic activity. A slight androgenic activity, probably due to the 17-hydro derivative, has been observed mainly at high doses. In multiple daily doses trials, Exemestane had no detectable effects on adrenal biosynthesis of cortisol or aldosterone, measured before or after ACTH challenge, thus demonstrating its selectivity with regard to the other enzymes involved in the steroidogenic pathway.
Glucocorticoid or mineralocorticoid replacements are therefore not needed. A non dose-dependent slight increase in serum LH and FSH levels has been observed even at low doses: this effect is, however, expected for the pharmacological class and is probably the result of feedback at the pituitary level due to the reduction in oestrogen levels that stimulate the pituitary secretion of gonadotropins also in postmenopausal women.
Pharmacokinetics: Absorption: After oral administration of Exemestane tablets, Exemestane is absorbed rapidly. The fraction of the dose absorbed from the gastrointestinal tract is high. The absolute bioavailability in humans is unknown, although it is anticipated to be limited by an extensive first pass effect. A similar effect resulted in an absolute bioavailability in rats and dogs of 5%. After a single dose of 25 mg, maximum plasma levels of 18 ng/ml are reached after 2 hours. Concomitant intake with food increases the bioavailability by 40%.
Distribution: The volume of distribution of Exemestane, not corrected for the oral bioavailability, is ca 20000 l. The kinetics is linear and the terminal elimination half-life is 24 h. binding to plasma proteins is 90% and is concentration independent. Exemestane and its metabolites do not bind to red blood cells.
Exemestane does not accumulate in an unexpected way after repeated dosing.
Metabolism and excretion: Exemestane is metabolised by oxidation of the methylene moiety on the 6 position by CYP 3A4 isoenzyme and/or reduction of the 17-keto group by aldoketoreductase followed by conjugation. The clearance of exemestane is ca 500 l/h, not corrected for the oral bioavailability.
The metabolites are inactive or the inhibition of aromatase is less than the parent compound.
The amount excreted unchanged in urine is 1% of the dose. In urine and faeces equal amounts (40%) of 14C-labeled exemestane were eliminated within a week.
Special populations: Age: No significant correlation between the systemic exposure of Exemestane and the age of subjects has been observed.
Renal insufficiency: In patients with severe renal impairment (CLcr < 30 ml/min) the systemic exposure to Exemestane was 2 times higher compared with healthy volunteers.
Given the safety profile of exemestane, no dose adjustment is considered to be necessary.
Hepatic insufficiency: In patients with moderate or severe hepatic impairment the exposure of Exemestane is 2-3 fold higher compared with healthy volunteers. Given the safety profile of Exemestane, no dose adjustment is considered to be necessary.
Toxicology: Preclinical safety data: Toxicological studies: Findings in the repeat dose toxicology studies in rat and dog were generally attributable to the pharmacological activity of Exemestane, such as effects on reproductive and accessory organs. Other toxicological effects (on liver, kidney or central nervous system) were observed only at exposures considered sufficiently in excess of the maximum human exposure indicating little relevance to clinical use.
Mutagenicity: Exemestane was not genotoxic in bacteria (Ames test), in V79 Chinese hamster cells, in rat hepatocytes or in the mouse micronucleus assay. Although Exemestane was clastogenic in lymphocytes in vitro, it was not clastogenic in two in vivo studies.
Reproductive toxicology: Exemestane was embryotoxic in rats and rabbits at systemic exposure levels similar to those obtained in humans at 25 mg/day. There was no evidence of teratogenicity.
Carcinogenicity: In a two-year carcinogenicity study in female rats, no treatment-related tumors were observed. In male rats the study was terminated on week 92, because of early death by chronic nephropathy. In a two-year carcinogenicity study in mice, an increase in the incidence of hepatic neoplasms in both genders was observed at the intermediate and high doses (150 and 450 mg/kg/day). This finding is considered to be related to the induction of hepatic microsomal enzymes, an effect observed in mice but not in clinical studies. An increase in the incidence of renal tubular adenomas was also noted in male mice at the high dose (450 mg/kg/day). This change is considered to be species and gender-specific and occurred at a dose which represents 63-fold greater exposure than occurs at the human therapeutic dose. None of these observed effects is considered to be clinically relevant to the treatment of patients with Exemestane.
Exemestane is indicated for the adjuvant treatment of postmenopausal women with oestrogen receptor positive invasive early breast cancer, following 2 - 3 years of initial adjuvant Tamoxifen therapy.
Exemestane is indicated for the treatment of advanced breast cancer in women with natural or induced postmenopausal status whose disease has progressed following anti-oestrogen therapy. Efficacy has not been demonstrated in patients with oestrogen receptor negative status.
Adult and elderly patients: The recommended dose is one film-coated tablet (25mg) to be taken orally once a day, after a meal.
In patients with early breast cancer, treatment with Exemestane should continue until completion of five years of combined sequential adjuvant hormonal therapy (Tamoxifen followed by Exemestane), or earlier if tumour relapse occurs.
In patients with advanced breast cancer, treatment with Exemestane should continue until tumour progression is evident.
No dose adjustments are required for patients with hepatic or renal insufficiency (see Pharmacology: Pharmacokinetics under Actions).
Children and adolescents: Not recommended for use in children and adolescents.
Exemestane given up to 800 mg in a single dose to healthy female volunteers and up to 600 mg daily to postmenopausal women with advanced breast cancer; were well tolerated. The single dose of Exemestane that could result in life-threatening symptoms is not known. In rats and dogs, lethality was observed after single oral doses equivalent respectively to 2000 and 4000 times the recommended human dose on a mg/m2 basis. There is no specific antidote to overdosing and treatment must be symptomatic. General supportive care, including frequent monitoring of vital signs and close observation of the patient, is indicated.
Exemestane is contraindicated in: pre-menopausal women; pregnant or lactating women; patients with hypersensitivity to the active substance or to any of the excipients.
Exemestane should not be administered to women with pre-menopausal endocrine status. Therefore, whenever clinically appropriate, the post-menopausal status should be ascertained by assessment of LH, FSH and oestradiol levels.
Exemestane should be used with caution in patients with hepatic or renal impairment.
Exemestane is a potent oestrogen lowering agent, and a reduction in bone mineral density and an increased fracture rate has been observed following administration (see Pharmacology: Pharmacodynamics under Actions). During adjuvant treatment with Exemestane, women with osteoporosis or at risk of osteoporosis should have their bone mineral density formally assessed by bone densitometry at the commencement of treatment. Although adequate data to show the effects of therapy in the treatment of the bone mineral density loss caused by Exemestane are not available, treatment for osteoporosis should be initiated in at risk patients. Patients treated with Exemestane should be carefully monitored.
Effects on ability to drive and use machines: Drowsiness, somnolence, asthenia and dizziness have been reported with the use of the drug. Patients should be advised that, if these events occur, their physical and/or mental abilities required for operating machinery or driving a car may be impaired.
Pregnancy: No clinical data on exposed pregnancies are available with Exemestane.
The potential risk for humans is unknown. Exemestane is therefore contraindicated in pregnant women.
Lactation: It is not known whether Exemestane is excreted into human milk, therefore, should not be administered to lactating woman.
Women of perimenopausal status or child-bearing potential: The physician needs to discuss the necessity of adequate contraception with women who have the potential to become pregnant including women who are perimenopausal or who have recently become postmenopausal, until their postmenopausal status is fully established (see Contraindications and Precautions).
Exemestane was generally well tolerated at a standard dose of 25 mg/day, and undesirable effects were usually mild to moderate.
The withdrawal rate due to adverse events was 7.4% in patients with early breast cancer receiving adjuvant treatment with Exemestane following initial adjuvant Tamoxifen therapy. The most commonly reported adverse reactions were hot flushes (22%), arthralgia (18%) and fatigue (16%).
The withdrawal rate due to adverse events was 2.8% in the overall patient population with advanced breast cancer. The most commonly reported adverse reactions were hot flushes (14%) and nausea (12%).
Most adverse reactions can be attributed to the normal pharmacological consequences of oestrogen deprivation (e.g. hot flushes).
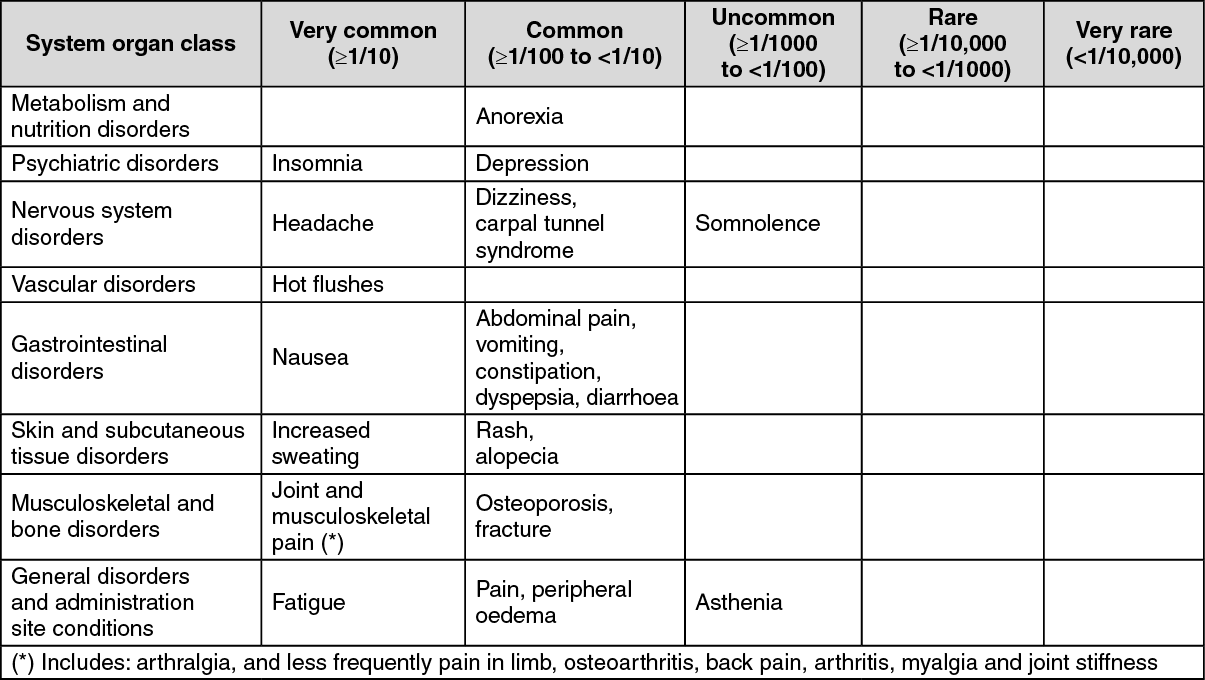
The reported adverse reactions are listed as follows by system organ class and by frequency. Frequencies are defined as: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1000 to ≤ 1/100), rare (≥1/10,000 to <1/1000). (See Table.)
 Click on icon to see table/diagram/image
Blood and lymphatic system disorders:
Click on icon to see table/diagram/image
Blood and lymphatic system disorders: In patients with advanced breast cancer thrombocytopenia and leucopenia have been rarely reported. An occasional decrease in lymphocytes has been observed in approximately 20% of patients receiving Exemestane, particularly in patients with pre-existing lymphopenia; however, mean lymphocyte values in these patients did not change significantly over time and no corresponding increase in viral infections was observed. These effects have not been observed in patients treated in early breast cancer studies.
Hepatobiliary disorders: Elevation of liver function test parameters including enzymes, bilirubin and alkaline phosphatase have been observed.
Adverse reactions from post-marketing experience: Hepatobiliary disorders: Hepatitis, cholestatic hepatitis.
Because reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
In vitro evidence showed that the drug is metabolised through cytochrome P450 (CYP) 3A4 and aldoketoreductases (see Pharmacology: Pharmacokinetics under Actions) and does not inhibit any of the major CYP isoenzymes.
Exemestane should be used cautiously with drugs that are metabolised via CYP3A4 and have a narrow therapeutic window. There is no clinical experience of the concomitant use with other anticancer drugs.
Exemestane should not be co administered with oestrogen-containing medicines as these would negate its pharmacological action.
Special precautions for disposal and other handling: Any unused product or waste should be disposed of in accordance with local requirements.
Keep at temperatures not exceeding 25°C.
Shelf life: 3 years.
L02BG06 - exemestane ; Belongs to the class of enzyme inhibitors. Used in treatment of neoplastic diseases.
Exemestane Stada FC tab 25 mg
100's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out