Administration: Fluconazole is administered orally.
The physician should prescribe the most appropriate pharmaceutical form and strength according to age, weight and dose. The capsule formulation is not adapted for use in infants and small children.
The capsules should be swallowed whole and independent of food intake.
Dosage: The dose should be based on the nature and severity of the fungal infection. Treatment of infections requiring multiple dosing should be continued until clinical parameters or laboratory tests indicate that active fungal infection has subsided. An inadequate period of treatment may lead to recurrence of active infection.
Adults: Treatment: Coccidioidomycosis: Use 200 mg to 400 mg once daily. Duration of treatment is 11 months up to 24 months or longer depending on the patient. 800 mg daily may be considered for some infections and especially for meningeal disease.
Mucosal candidiasis including: Oropharyngeal candidiasis: Loading dose is 200 mg to 400 mg on Day 1. Subsequent dose is 100 mg to 200 mg once daily. Duration of treatment is 7 to 21 days (until oropharyngeal candidiasis is in remission). Longer periods may be used in patients with severely compromised immune function.
Oesophageal candidiasis: Loading dose is 200 mg to 400 mg on Day 1. Subsequent dose is 100 mg to 200 mg once daily. Duration of treatment is 14 to 30 days (until oesophageal candidiasis is in remission). Longer periods may be used in patients with severely compromised immune function.
Candiduria: Use 200 mg to 400 mg once daily. Duration of treatment is 7 to 21 days. Longer periods may be used in patients with severely compromised immune function.
Vaginal candidiasis: Acute vaginal candidiasis: Use 150 mg as a single dose.
Recurrent vaginal candidiasis (4 or more episodes a year): Use 150 mg every third day for a total of 3 doses (day 1, 4, and 7) followed by 150 mg once weekly maintenance dose (Maintenance dose: 6 months).
Candidal balanitis: Use 150 mg as a single dose.
Dermatomycosis including: Tinea pedis, tinea corporis, tinea cruris and dermal candida infections: Use 150 mg once weekly. Duration of treatment is 2 to 4 weeks; tinea pedis may require treatment for up to 6 weeks.
Tinea versicolor: Use 300 mg to 400 mg once weekly. Duration of treatment is 1 to 3 weeks.
Tinea unguinium (onychomycosis): Use 150 mg once weekly. Treatment should be continued until infected nail is replaced (uninfected nail grows in). Regrowth of fingernails and toenails normally requires 3 to 6 months and 6 to 12 months, respectively. However, growth rates may vary widely in individuals and by age. After successful treatment of long-term chronic infections, nails occasionally remain disfigured.
Prophylaxis: Relapse of oropharyngeal or oesophageal candidiasis in the patients infected with HIV: Use 100 mg to 200 mg once daily. Duration of treatment is an indefinite period for patients with chronic immune suppression.
To reduce the incidence of recurrent vaginal candidiasis (4 or more episodes a year): Use 150 mg every third day for a total of 3 doses (day 1, 4, and 7) followed by 150 mg once weekly maintenance dose (Maintenance dose: 6 months).
Prophylaxis of candidal infections in the patients with prolonged neutropenia: Use 200 mg to 400 mg once daily. Treatment should start several days before the anticipated onset of neutropenia and continue for 7 days after recovery from neutropenia after the neutrophil count rises above 1000 cells per mm
3.
Special populations: Elderly: Dosage should be adjusted based on the renal function.
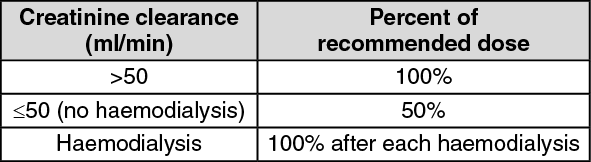
Renal impairment: The drug is predominantly excreted in the urine as unchanged active substance. No adjustments in single dose therapy are necessary. In patients with impaired renal function who will receive multiple doses of fluconazole, an initial dose of 50 mg to 400 mg should be given, based on the recommended daily dose for the indication. After this initial loading dose, the daily dose (according to indication) should be based on the following table: See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patients on haemodialysis should receive 100% of the recommended dose after each haemodialysis; on non-dialysis days, patients should receive a reduced dose according to their creatinine clearance.
Hepatic impairment: Limited data are available in patients with hepatic impairment, therefore fluconazole should be administered with caution to patients with liver dysfunction.
(For dosages other than 150 mg or multiple of 150 mg (e.g. 300 mg), physicians should consider other registered products in the market.)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out