Active ingredient: Metformin hydrochloride 500 mg.
Excipients/Inactive Ingredients: Povidone K25, hypromellose, magnesium stearate, opadry white.
Treatment of type 2 diabetes mellitus, particularly in overweight patients, when dietary management and exercise alone does not result in adequate glycaemic control.
In adults, Metformin STELLA 500 mg may be used as monotherapy or in combination with other oral antidiabetic agents or with insulin.
In children from 10 years of age and adolescents, Metformin STELLA 500 mg may be used as monotherapy or in combination with insulin.
A reduction of diabetic complications has been shown in overweight type 2 diabetic adult patients treated with metformin as first-line therapy after diet failure.
Adults with normal renal function (GFR ≥ 90 ml/min): Monotherapy and combination with other oral antidiabetic agents: The usual starting dose is 500 mg or 850 mg metformin hydrochloride 2 or 3 times daily given during or after meals.
After 10 to 15 days the dose should be adjusted on the basis of blood glucose measurements. A slow increase of dose may improve gastrointestinal tolerability.
The maximum recommended dose of metformin hydrochloride is 3 g daily, taken as 3 divided doses.
If transfer from another oral antidiabetic agent is intended: Discontinue the other agent and initiate metformin at the dose indicated previously.
Combination with insulin: Metformin and insulin may be used in combination therapy to achieve better blood glucose control. Metformin hydrochloride is given at the usual starting dose of 500 mg or 850 mg 2 or 3 times daily, while insulin dosage is adjusted on the basis of blood glucose measurements.
Elderly: Due to the potential for decreased renal function in elderly subjects, the metformin dosage should be adjusted based on renal function. Regular assessment of renal function is necessary.
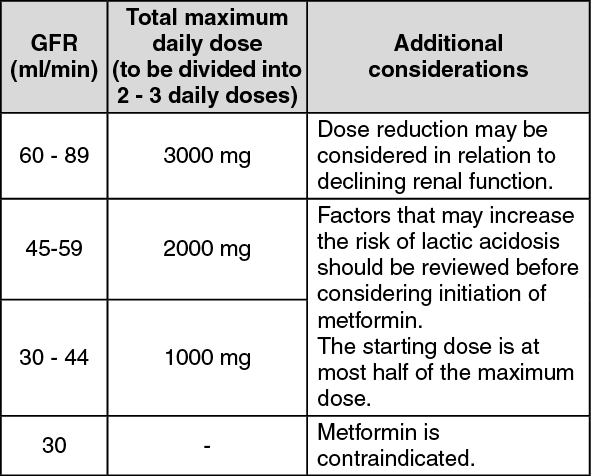
Renal impairment: A GFR should be assessed before initiation of treatment with metformin containing products and at least annually thereafter. In patients at an increased risk of further progression of renal impairment and in the elderly, renal function should be assessed more frequently, e.g. every 3 - 6 months. (See table.)
 Click on icon to see table/diagram/image
Paediatric population: Monotherapy and combination with insulin:
Click on icon to see table/diagram/image
Paediatric population: Monotherapy and combination with insulin: Metformin STELLA 500 mg can be used in children from 10 years of age and adolescents.
The usual starting dose is 500 mg or 850 mg metformin hydrochloride once daily, given during or after meals.
After 10 to 15 days the dose should be adjusted on the basis of blood glucose measurements. A slow increase of dose may improve gastrointestinal tolerability. The maximum recommended dose of metformin hydrochloride is 2 g daily, taken as 2 or 3 divided doses.
Hypoglycaemia has not been seen with metformin hydrochloride doses of up to 85 g, although lactic acidosis has occurred in such circumstances. High overdose of metformin or concomitant risks may lead to lactic acidosis. Lactic acidosis is a medical emergency and must be treated in hospital. The most effective method to remove lactate and metformin is haemodialysis.
Hypersensitivity to metformin or to any of the excipients listed in the product.
Any type of acute metabolic acidosis (such as lactic acidosis, diabetic ketoacidosis).
Diabetic pre-coma.
Severe renal failure (GFR < 30 ml/min).
Acute conditions with the potential to alter renal function such as: Dehydration, severe infection, shock.
Disease which may cause tissue hypoxia (especially acute disease, or worsening of chronic disease) such as: Decompensated heart failure, respiratory failure, recent myocardial infarction, shock.
Hepatic insufficiency, acute alcohol intoxication, alcoholism.
Lactic acidosis: Lactic acidosis, a very rare, but serious metabolic complication, most often occurs at acute worsening of renal function or cardiorespiratory illness or sepsis. Metformin accumulation occurs at acute worsening of renal function and increases the risk of lactic acidosis.
In case of dehydration (severe diarrhoea or vomiting, fever or reduced fluid intake), metformin should be temporarily discontinued and contact with a health care professional is recommended.
Medicinal products that can acutely impair renal function (such as antihypertensives, diuretics and NSAIDs) should be initiated with caution in metformin-treated patients. Other risk factors for lactic acidosis are excessive alcohol intake, hepatic insufficiency, inadequately controlled diabetes, ketosis, prolonged fasting and any conditions associated with hypoxia, as well as concomitant use of medicinal products that may cause lactic acidosis.
Patients and/or care-givers should be informed of the risk of lactic acidosis. Lactic acidosis is characterised by acidotic dyspnoea, abdominal pain, muscle cramps, asthenia and hypothermia followed by coma. In case of suspected symptoms, the patient should stop taking metformin and seek immediate medical attention. Diagnostic laboratory findings are decreased blood pH (< 7.35), increased plasma lactate levels (> 5 mmol/L) and an increased anion gap and lactate/pyruvate ratio.
Renal function: GFR should be assessed before treatment initiation and regularly thereafter. Metformin is contraindicated in patients with GFR < 30 ml/min and should be temporarily discontinued in the presence of conditions that alter renal function.
Cardiac function: Patients with heart failure are more at risk of hypoxia and renal insufficiency. In patients with stable chronic heart failure, metformin may be used with a regular monitoring of cardiac and renal function.
For patients with acute and unstable heart failure, metformin is contraindicated.
Administration of iodinated contrast agents: Intravascular administration of iodinated contrast agents may lead to contrast induced nephropathy, resulting in metformin accumulation and an increased risk of lactic acidosis. Metformin should be discontinued prior to or at the time of the imaging procedure and not restarted until at least 48 hours after, provided that renal function has been re-evaluated and found to be stable.
Surgery: Metformin must be discontinued at the time of surgery under general, spinal or epidural anaesthesia. Therapy may be restarted no earlier than 48 hours following surgery or resumption of oral nutrition and provided that renal function has been re-evaluated and found to be stable.
Other precautions: All patients should continue their diet with a regular distribution of carbohydrate intake during the day. Overweight patients should continue their energy-restricted diet.
The usual laboratory tests for diabetes monitoring should be performed regularly.
Metformin alone does not cause hypoglycaemia, but caution is advised when it is used in combination with insulin or other oral antidiabetics (e.g. sulfonylureas or meglitinides).
Effects on ability to drive and use machines: Metformin monotherapy does not cause hypoglycaemia and therefore has no effect on the ability to drive or to use machines.
However, patients should be alerted to the risk of hypoglycaemia when metformin is used in combination with other antidiabetic agents (e.g. sulfonylureas, insulin or meglitinides).
Use in Children: The diagnosis of type 2 diabetes mellitus should be confirmed before treatment with metformin is initiated.
No effect of metformin on growth and puberty has been detected during controlled clinical studies of one-year duration but no long-term data on these specific points are available. Therefore, a careful follow-up of the effect of metformin on these parameters in metformin-treated children, especially prepubescent children, is recommended.
Children aged between 10 and 12 years: Only 15 subjects aged between 10 and 12 years were included in the controlled clinical studies conducted in children and adolescents. Although efficacy and safety of metformin in these children did not differ from efficacy and safety in older children and adolescents, particular caution is recommended when prescribing to children aged between 10 and 12 years.
Pregnancy: Uncontrolled diabetes during pregnancy (gestational or permanent) is associated with increased risk of congenital abnormalities and perinatal mortality.
A limited amount of data from the use of metformin in pregnant women does not indicate an increased risk of congenital abnormalities. Animal studies do not indicate harmful effects with respect to pregnancy, embryonic or foetal development, parturition or postnatal development.
When the patient plans to become pregnant and during pregnancy, it is recommended that diabetes is not treated with metformin but insulin be used to maintain blood glucose levels as close to normal as possible, to reduce the risk of malformations of the foetus.
Lactation: Metformin is excreted into human breast milk. No adverse effects were observed in breastfed newborns/infants. However, as only limited data are available, breast-feeding is not recommended during metformin treatment. A decision on whether to discontinue breast-feeding should be made, taking into account the benefit of breast-feeding and the potential risk to adverse effects on the child.
During treatment initiation, the most common adverse reactions are nausea, vomiting, diarrhoea, abdominal pain and loss of appetite which resolve spontaneously in most cases. To prevent them, it is recommended to take metformin in 2 or 3 daily doses and to increase slowly the doses.
The following adverse reactions may occur under treatment with metformin. Frequencies are defined as follows: very common: ≥1/10; common >1/100, <1/10; uncommon >1/1,000, <1/100; rare >1/10,000, <1/1,000; very rare <1/10,000.
Within each frequency grouping, adverse reactions are presented in order of decreasing seriousness.
Metabolism and nutrition disorders: Very rare: Lactic acidosis.
Decrease of vitamin B12 absorption with decrease of serum levels during long-term use of metformin. Consideration of such aetiology is recommended if a patient presents with megaloblastic anaemia.
Nervous system disorders: Common: Taste disturbance.
Gastrointestinal disorders: Very common: Gastrointestinal disorders such as nausea, vomiting, diarrhoea, abdominal pain and loss of appetite. These undesirable effects occur most frequently during initiation of therapy and resolve spontaneously in most cases. To prevent them, it is recommended that metformin be taken in 2 or 3 daily doses during or after meals. A slow increase of the dose may also improve gastrointestinal tolerability.
Hepatobiliary disorders: Very rare: Isolated reports of liver function tests abnormalities or hepatitis resolving upon metformin discontinuation.
Skin and subcutaneous tissue disorders: Very rare: Skin reactions such as erythema, pruritus, urticaria.
Paediatric population: In published and post marketing data and in controlled clinical studies in a limited paediatric population aged 10-16 years treated during 1 year, adverse event reporting was similar in nature and severity to that reported in adults.
Concomitant use not recommended: Alcohol: Alcohol intoxication is associated with an increased risk of lactic acidosis, particularly in case of fasting, malnutrition or hepatic impairment.
Iodinated contrast agents: Metformin must be discontinued prior to or at the time of the imaging procedure and not restarted until at least 48 hours after, provided that renal function has been re-evaluated and found to be stable.
Combinations requiring precautions for use: Some medicinal products can adversely affect renal function which may increase the risk of lactic acidosis, e.g. NSAIDs, including selective cyclo-oxygenase (COX) II inhibitors, ACE inhibitors, angiotensin II receptor antagonists and diuretics, especially loop diuretics. When starting or using such products in combination with metformin, close monitoring of renal function is necessary.
Medicinal products with intrinsic hyperglycaemic activity (e.g. glucocorticoids (systemic and local routes) and sympathomimetics): More frequent blood glucose monitoring may be required, especially at the beginning of treatment. If necessary, adjust the metformin dosage during therapy with the respective medicinal product and upon its discontinuation.
Organic cation transporters (OCT): Metformin is a substrate of both transporters OCT1 and OCT2.
Co-administration of metformin with: Inhibitors of OCT1 (such as verapamil) may reduce efficacy of metformin.
Inducers of OCT1 (such as rifampicin) may increase gastrointestinal absorption and efficacy of metformin.
Inhibitors of OCT2 (such as cimetidine, dolutegravir, ranolazine, trimethoprim, vandetanib, isavuconazole) may decrease the renal elimination of metformin and thus lead to an increase in metformin plasma concentration.
Inhibitors of both OCT1 and OCT2 (such as crizotinib, olaparib) may alter efficacy and renal elimination of metformin.
Caution is therefore advised, especially in patients with renal impairment, when these drugs are co-administered with metformin, as metformin plasma concentration may increase. If needed, dose adjustment of metformin may be considered as OCT inhibitors/inducers may alter the efficacy of metformin.
Store in a well-closed container, in a dry place. Do not store above 30°C.
A10BA02 - metformin ; Belongs to the class of biguanides. Used in the treatment of diabetes.
Metformin Stella FC tab 500 mg
30's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out