Nicardipine hydrochloride.
Nicardipine hydrochloride 10 mg for 10 ml of solution for injection / infusion.
Excipient with known effect: sorbitol and sodium.
Each ml of solution for injection / infusion contains 0.039 mg equivalent to 0.0017 mmol of sodium. Each 10ml ampoule contains 0.39 mg equivalent to 0.017 mmol of sodium.
Each ml of solution for injection / infusion contains 50 mg of sorbitol. Each 10 ml ampoule contains 500 mg of sorbitol.
Excipients/Inactive Ingredients: Sorbitol, citric acid monohydrate, sodium citrate, hydrochloric acid, sodium hydroxide, water for injections.
Pharmacotherapeutic group: Selective calcium inhibitors with vascular effects. ATC code: C08CA04 (cardiovascular system).
Pharmacology: Pharmacodynamics: Mechanism of action: Nicardipine is a second generation slow calcium channel inhibitor, and belongs to the phenyl-dihydropyridine group. Nicardipine has a greater selectivity for L-type calcium channels in vascular smooth muscle than cardiac myocytes. At very low concentrations, it inhibits the influx of calcium into the cell. Its action is produced mainly on arterial smooth muscle. This is reflected in relatively large and rapid changes in blood pressure, with minimal inotropic changes in cardiac function (baroreflex effect).
Pharmacodynamic effects: Administered by systemic route, nicardipine is a potent vasodilator which diminishes total peripheral resistance and lowers blood pressure. Heart rate is temporarily increased; as a result of a decrease in after-load, cardiac output is markedly and durably increased.
In humans, the vasodilator action also occurs in both acute dose administration and chronic administration in the large and small arteries, increasing blood flow and improving arterial compliance. Renal vascular resistance is decreased.
Pharmacokinetics: Distribution: Nicardipine is highly bound to plasma proteins over a wide concentration range.
Biotransformation: Nicardipine is metabolised by cytochrome P450 3A4. Studies involving either a single dose, or administration 3 times daily for 3 days, have shown that less than 0.03% of unchanged nicardipine is recovered in the urine in humans after oral or intravenous administration. The most abundant metabolite in human urine is the glucuronide of the hydroxy form, which is formed by the oxidative cleaving of the N-methylbenzyl moiety and the oxidation of the pyridine ring.
Elimination: After co-administration of a radioactive intravenous dose of nicardipine with an oral 30 mg dose given every 8 hours, 49% of the radioactivity was recovered in the urine and 43% in the faeces within 96 hours. None of the dose was recovered as unchanged nicardipine in the urine. The elimination profile of the medicinal product following an intravenous dose consists of three phases, with corresponding half-life: alpha 6.4 min, beta 1.5 hours, gamma 7.9 hours.
Renal failure: The pharmacokinetics of intravenously administered nicardipine was studied in subjects with severe renal failure requiring haemodialysis (creatinine clearance <10 ml/min), mild/moderate renal failure (creatinine clearance 10-50 ml/min) and normal renal function (creatinine clearance >50 ml/min). At steady state, Cmax and AUC were significantly higher and clearance significantly lower in subjects with mild/moderate renal failure compared to subjects with normal renal function. There were no significant differences in the principal pharmacokinetic parameters between severe renal dysfunction and normal renal function.
Toxicology: Preclinical safety data: Nicardipine has been shown to pass into the milk of lactating animals. It has been reported in animal studies that the medicinal product is excreted into breast milk. In animal studies where this medicinal product was administered at a high dose during the terminal stage of pregnancy, an increase in foetal deaths, delivery disturbances, decrease in the body weight of offspring, and suppression of post-natal body weight gain were reported. However, toxicity to reproduction has not been reported.
Intravenous nicardipine is indicated for the treatment of acute life-threatening hypertension, particularly in the event of: Malignant arterial hypertension/Hypertensive encephalopathy; Aortic dissection, when short acting beta-blocker therapy is not suitable, or in combination with a beta-blocker when beta-blocking alone is not effective; Severe pre-eclampsia, when other intravenous antihypertensive agents are not recommended or are contra-indicated.
Nicardipine is also indicated for the treatment of post-operative hypertension.
Posology: The antihypertensive effect depends on the administered dose. The dosage to achieve the desired blood pressure can vary depending on the targeted blood pressure, the response of the patient, and the age or general condition of the patient.
Unless given via a central venous line, dilute the product to a concentration of 0.1-0.2 mg/ml before use (see Incompatibilities under Cautions for Usage for details on incompatible solutions).
Adults: Initial dose: Treatment should start with the continuous administration of nicardipine at a rate of 3-5 mg/h for 15 minutes. Rates can be increased by increments of 0.5 or 1 mg every 15 minutes. The infusion rate should not exceed 15 mg/h.
Maintenance dose: When the target pressure is reached, the dose should be reduced progressively, usually to between 2 and 4 mg/h, to maintain therapeutic efficacy.
Transition to an oral antihypertensive agent: Discontinue nicardipine or titrate downward while appropriate oral therapy is established. When an oral antihypertensive agent is being instituted, consider the lag time before onset of the oral agent's effect. Continue blood pressure monitoring until the desired effect is achieved.
A switch can also be made to oral nicardipine 20 mg tablets at a dosage of 60 mg/day in 3 daily doses, or to nicardipine 50 mg extended-release capsules, at a dosage of 100 mg/day, in 2 daily doses.
It should be noted that nicardipine 20 mg tablets and 50 mg extended-release capsules oral preparations are not available in Hong Kong market.
Elderly patients: Clinical studies on nicardipine did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects.
Elderly patients may be more sensitive to the effects of nicardipine because of impaired renal and/or hepatic function. It is recommended to provide a continuous infusion of nicardipine starting at a dose of 1 to 5 mg/h, depending on the blood pressure and clinical situation. After 30 minutes, depending on the effect observed, the rate can be increased or decreased by increments of 0.5 mg/h. The rate should not exceed 15 mg/h.
Pregnancy: It is recommended to provide a continuous infusion of nicardipine starting at 1 to 5 mg/h, depending on the blood pressure and clinical situation. After 30 minutes, depending on the effect observed, the rate can be increased or decreased by increments of 0.5 mg/h.
Doses higher than 4 mg/h are generally not exceeded in the treatment of pre-eclampsia. However, the rate should not exceed 15 mg/h (see Precautions, Use in Pregnancy & Lactation, and Adverse Reactions).
Hepatic failure: Nicardipine should be used with particular caution in these patients. Since nicardipine is metabolised in the liver, it is recommended to use the same dose regimens as for elderly patients in patients with hepatic failure or reduced hepatic blood flow.
Renal failure: Nicardipine should be used with particular caution in these patients. In some patients with moderate renal failure, a significantly lower systemic clearance and higher area under the curve (AUC) have been observed. Therefore, it is recommended to use the same dose regimens as for elderly patients in patients with renal failure.
Paediatric population: The safety and efficacy of nicardipine in low birth weight infants, newborns, nursing infants, infants, and children have not been established.
Nicardipine should only be used for life-threatening hypertension in paediatric intensive care settings or post-operative contexts.
Initial dose: In case of emergency, a starting dose of 0.5 to 5 mcg/kg/min is recommended.
Maintenance dose: The maintenance dose of 1 to 4 mcg/kg/min is recommended.
Nicardipine should be used with caution in children with renal failure. In this case, only the lowest dosage should be used.
Method of administration: Nicardipine must only be administered by continuous intravenous infusion.
Nicardipine must only be administered by specialists in a well-controlled medical environment, such as hospitals and intensive care units, with continuous monitoring of blood pressure. The rate of administration should be precisely controlled using an electronic syringe driver or a volumetric pump. The blood pressure and heart rate should be monitored at a minimum of every 5 minutes during infusion, then until stabilisation of vital signs and at least 12 hours after the end of nicardipine administration.
Symptoms: Overdose with nicardipine hydrochloride can potentially result in the following symptoms: marked hypotension, bradycardia, palpitations, flushing, drowsiness, collapse, peripheral oedema, confusion, slurred speech and hyperglycaemia. In animals, overdose also resulted in reversible hepatic function abnormalities, sporadic focal hepatic necrosis and progressive atrio-ventricular conduction block.
Management: In case of an overdose, it is recommended to use routine measures, including monitoring of cardiac and respiratory function. In addition to general supportive measures, intravenous calcium preparations and vasopressors are clinically indicated for patients exhibiting the effects of calcium entry blockade. Major hypotension can be treated by intravenous infusion of any plasma volume expander and supine position with the legs elevated.
Nicardipine is not dialyzable.
Hypersensitivity to the active substance or to any of the excipients listed in Description; Severe aortic stenosis; Compensatory hypertension, in case of an arteriovenous shunt or aortic coarctation; Unstable angina; Within 8 days after myocardial infarction.
It is recommended to administer nicardipine with caution to avoid an excessive fall in blood pressure. In fact, rapid pharmacologic reductions in blood pressure may produce systemic hypotension and reflex tachycardia. If either occurs with nicardipine, consider decreasing the dose by half or stop the infusion.
Bolus administration or intravenous administration not controlled by the use of an electronic syringe driver or a volumetric pump is not recommended and can increase the risk of serious hypotension, particularly in the elderly, in children, in patients with renal or hepatic failure and during pregnancy.
Cardiac failure: Nicardipine should be used with caution in patients with congestive cardiac failure or pulmonary oedema, particularly when these patients are receiving concomitant beta-blockers, as worsening of cardiac failure may occur.
Ischaemic cardiovascular disease: Nicardipine is contra-indicated in unstable angina and immediately following myocardial infarction (see Contraindications).
Nicardipine should be used with caution in patients with suspected coronary ischaemia. Occasionally, patients have developed an increased frequency, duration, or severity of angina upon starting or increasing nicardipine dosage, or during the course of treatment.
Patients with history of hepatic dysfunction or hepatic failure: Rare cases of abnormal hepatic function possibly associated with the administration of nicardipine have been reported. Potential risk groups are patients with a history of hepatic dysfunction or those with hepatic failure at the initiation of treatment with nicardipine. Nicardipine should be used with particular caution in patients with hepatic failure.
Renal failure: Nicardipine should be used with caution in patients with renal failure (see Pharmacology: Pharmacokinetics under Actions).
Patients with portal hypertension: Intravenous nicardipine at high doses has been reported to worsen portal vein hypertension and portal-systemic collateral blood flow index in cirrhotic patients.
Patients with pre-existing intracranial hypertension: Nicardipine should be used with caution in patients with a risk of increased intracranial pressure. Intracranial pressure should be monitored, to allow calculation of the cerebral perfusion pressure.
Patients with stroke: Nicardipine should be used with caution in patients with acute cerebral infarction. A hypertensive episode which often accompanies a stroke is not an indication for emergency antihypertensive therapy. The use of antihypertensive medicinal products is not recommended in ischaemic stroke patients unless acute hypertension precludes the administration of an adequate treatment (e.g. thrombolysis) or there is other end-organ damage which is life-threatening in the short term.
Use in Pregnancy: Due to the risk of severe maternal hypotension and potentially fatal foetal hypoxia, the decrease in blood pressure should be progressive and always closely monitored. Due to the possible risk of pulmonary oedema or excessive decrease in blood pressure, caution should be taken if magnesium sulphate is used concomitantly.
As cases of acute pulmonary oedema have been reported during pregnancy, nicardipine should be administered with caution in pregnant women, who should be closely monitored to detect possible onset of acute pulmonary oedema. If an acute pulmonary oedema occurs, nicardipine treatment should be immediately stopped and an appropriate treatment should be initiated.
Combination with beta-blockers: Caution should be exercised when using nicardipine in combination with a beta-blocker in patients with decreased cardiac function. In such case, the dosage of the beta-blocker should be individualized to the clinical situation of each patient (see Interactions).
Injection site reactions: Infusion site reactions can occur, particularly with a prolonged duration of administration and in peripheral veins. It is advised to change the infusion site in case of any suspicion of injection site irritation. The use of a central venous line or of a greater dilution of the solution could reduce the risk of occurrence of injection site reaction.
Excipient: This medicine contains sorbitol. Its use is not recommended in patients with hereditary fructose intolerance (rare hereditary disease).
Effects on ability to drive and use machines: Reactions to the medicinal product, which vary from one individual to another, may affect the ability to drive and use machines. More particularly at the beginning or in case of any change to treatment and in combination with alcohol. Precautions should be taken since the hypotensive effects of this medicinal product may cause dizziness.
Use in Children: The safety and efficacy of nicardipine IV has not been tested in controlled clinical trials in infants or children, thus special care is required in this population (see Dosage & Administration).
Pregnancy: Animal studies have shown no teratogenic effects. In the absence of teratogenic effects in animals, no malformative effect is expected in humans. In fact, until now, substances responsible for malformations in humans have always been demonstrated to be teratogenic in animals during studies carried out well in two species. Nicardipine should only be used if the benefit outweighs the risk because a reduction of birth weight in newborns has been reported when used in combination with calcium channel blockers.
Limited pharmacokinetic data have shown that nicardipine IV does not accumulate and has a low placental transfer.
In clinical practice, the use of nicardipine during the first two trimesters in a limited number of pregnancies has not revealed any malformative or particular foetotoxic effect to date.
The use of nicardipine for severe pre-eclampsia during the third trimester of pregnancy could potentially produce an undesirable tocolytic effect which could potentially interfere with the spontaneous induction of labour.
Acute pulmonary oedema has been observed when nicardipine has been used as tocolytic during pregnancy (see Precautions and Adverse Reactions), especially in cases of multiple pregnancy (twins or more), with the intravenous route and/or concomitant use of beta-2-agonists. Nicardipine should not be used in multiple pregnancies or in pregnant women with compromised cardio-vascular condition, except if there is no other acceptable alternative.
Breast-feeding: Nicardipine should not be used during breast-feeding (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Fertility: Not applicable.
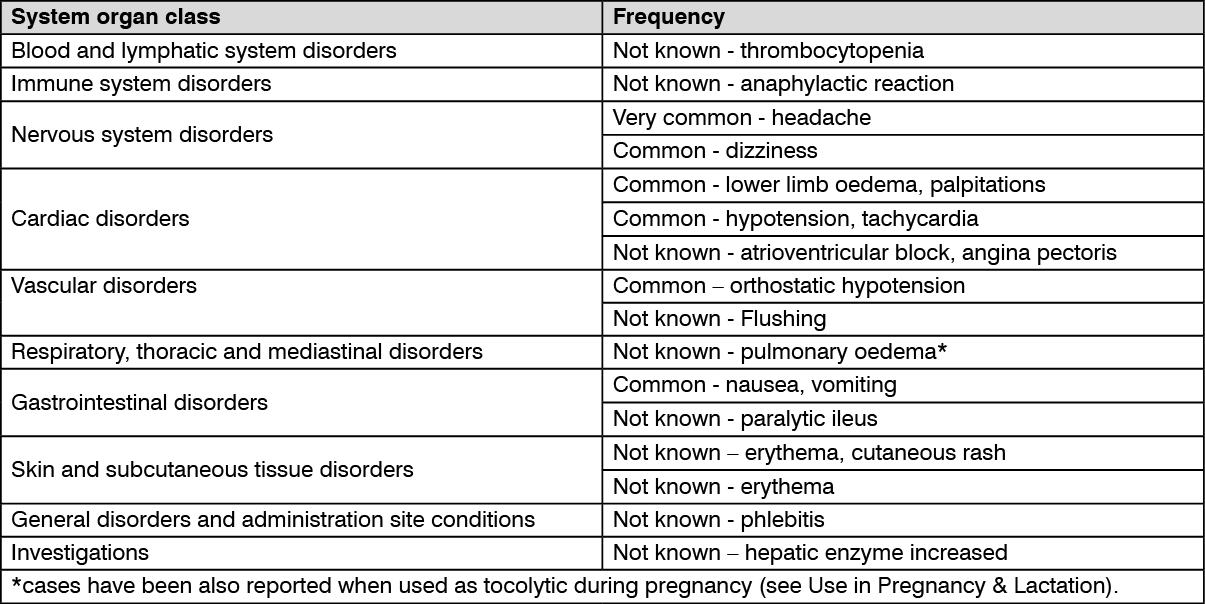
Summary of safety profile: The majority of undesirable effects are the consequence of the vasodilator effects of nicardipine. The most common effects are headache, dizziness, peripheral oedema, palpitations and flushing.
Tabulated list of adverse reactions: Adverse reactions listed as follows have been observed during clinical studies and/or after marketed use and are based on clinical trial data and classified according to MedDRA System Organ Class. Frequency categories are defined according to the following convention: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000) and not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Inadvisable combinations: Dantrolene: Dantrolene administered by infusion: In animal studies, fatal ventricular fibrillation cases are consistently observed when verapamil and dantrolene are administered intravenously. The combination of a calcium channel inhibitor and dantrolene is therefore potentially dangerous.
However, a few patients received the combination of nifedipine and dantrolene without any inconvenience.
Combinations requiring precautions for use: Idelalisib: Increased adverse effects of nicardipine, such as orthostatic hypotension, especially in elderly patients.
Clinical monitoring and dosage adjustment of nicardipine should be performed during treatment with idelalisib and after its discontinuation.
Immunosuppressants (Ciclosporine, everolimus, sirolimus, tacrolimus and temsirolimus): Increase in blood levels of the immunosuppressant, by inhibiting its metabolism. Determination of blood levels of the immunosuppressant, monitoring of renal function and adjustment of its dosage during treatment and after discontinuation.
CYP3A4 inducers and inhibitors: Nicardipine is metabolised by cytochrome P450 3A4. Co-administration of CYP 3A4 enzyme-inducing agents (e.g. carbamazepine, phenobarbital, phenytoin, fosphenytoin, primidone and rifampicin) may cause a decrease in the plasma concentrations of nicardipine due to its increased hepatic metabolism.
Clinical monitoring and possible dosage adjustment if nicardipine should be performed during treatment with the anticonvulsant and after its discontinuation.
Co-administration of potent CYP3A4 enzyme-inhibiting agents (e.g. cimetidine, clarithromycin, cobicistat, erythromycin, itraconazole, grapefruit juice, ketoconazole, nelfinavir, posaconazole, ritonavir, telaprevir, telithromycin, voriconazole) may cause an increase in the plasma concentration of nicardipine.
Increased adverse effects of nicardipine, more commonly orthostatic hypotension, especially in elderly patients. Co-administration of calcium channel blockers with itraconazole has shown an increased risk of adverse effects, in particular oedema due to a decreased metabolism of the calcium channel blocker in the liver.
Clinical monitoring and dosage adjustment of nicardipine should be performed during treatment with a potent CYP3A4 enzyme inhibitor and after its discontinuation.
Combinations to be taken into account: Potential additive hypertensive effect: Medicinal products which could potentiate the antihypertensive effect of nicardipine during concomitant administration, with an increased risk of orthostatic hypotension, include baclofen, urologic alpha-blockers (alfuzosin, doxazosin, prazosin, silodosin, tamsulosin, terazosin), alpha-blocking antihypertensive agents (doxazosin, prazosin, urapidil), tricyclic antidepressants, imipramine antidepressants, neuroleptics, opioids and amifostine.
Nitrate derivatives and related agents: Increased risk of hypotension, particularly orthostatic hypotension.
Medicinal products that cause orthostatic hypotension: Increased risk of hypotension, particularly orthostatic hypotension.
Inhalational anaesthetics: The co-administration of nicardipine with inhalational anaesthetics could induce a potential additive or synergistic hypotensive effect, as well as an inhibition by anaesthetics of the baroreflex heart rate increase associated with peripheral vasodilators. Limited clinical data suggests that the effects of inhaled anaesthetics (e.g. isoflurane, sevoflurane and enflurane) on nicardipine appear to be moderate.
Enhancement of negative inotropic effect: Nicardipine may enhance the negative inotropic effect of beta-blockers in cardiac failure (bisoprolol, carvedilol, metoprolol, nebivolol) and may cause hypotension, cardiac failure in patients with latent or uncontrolled cardiac failure (see Warnings and Precautions). Moreover, the presence of a beta-blocker treatment can minimise the reflex sympathetic reaction set into action in case of excessive haemodynamic repercussion.
Nicardipine may enhance the negative inotropic effect of beta-blockers (except for esmolol) and may cause hypotension, cardiac failure in patients with latent or uncontrolled cardiac failure (see Warnings and Precautions) (addition of negative inotropic effects). Moreover, the beta-blocker can minimise the reflex sympathetic reaction set into action in case of excessive haemodynamic repercussion.
Magnesium: Due to the possible risk of pulmonary oedema or excessive decrease in blood pressure, caution should be taken if magnesium sulphate is used concomitantly (see Warnings).
Digoxin: Nicardipine has been reported to increase the plasma levels of digoxin in pharmacokinetic studies. Digoxin levels should be monitored when concomitant therapy with nicardipine is initiated.
Decrease of antihypertensive effect: Nicardipine in combination with intravenous corticosteroids (glucocorticoids and mineralocorticoids) and tetracosactide (except for hydrocortisone used as replacement therapy in Addison's disease) may cause a decrease in the antihypertensive effect.
Competitive neuromuscular blockers: Limited data suggest that nicardipine, as other calcium channel blockers, enhances neuromuscular block possibly by acting on the post-synaptic region. Vecuronium infusion dose requirements could be reduced by the concurrent use of nicardipine. Reversal of neuromuscular block by neostigmine appears not to be affected by nicardipine infusion. No additional monitoring is required.
Special precautions for disposal and other handling: Instructions for opening the ampoules: 1. Hold the ampoule with the coloured spot right up. If there is any liquid in the upper part of the ampoule, tap it to allow the liquid to run into the body of the ampoule.
2. Then grasp the top of the ampoule (above the tip) and apply a pressure to break the ampoule.
Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Incompatibilities: There is a risk of precipitation with products in solution of pH greater than 6 (e.g. bicarbonate solution, Ringer's solution, diazepam, furosemide, methohexital sodium, thiopental).
In the presence of saline solutions, there is a risk of nicardipine absorption on the plastic materials of infusion devices.
Do not store above +25°C.
Store the ampoule in the outer packaging, away from light.
Shelf life: Before opening: 2 years.
After opening: The physicochemical stability of the undiluted solution or diluted in a solution of 5% glucose in a polypropylene syringe has been demonstrated for 24 hours at a temperature of +25°C, away from light.
Nevertheless, from a microbiological standpoint, the product should be used immediately.
C08CA04 - nicardipine ; Belongs to the class of dihydropyridine derivative selective calcium-channel blockers with mainly vascular effects. Used in the treatment of cardiovascular diseases.
Nicardipine Aguettant soln for inj/infusion 10 mg/10 mL
10 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out