Pharmacotherapeutic group: Drugs used in diabetes, combinations of oral blood glucose lowering drugs.
ATC code: A10BD11.
Pharmacology: Pharmacodynamics: Trajenta Duo combines two antihyperglycaemic medicinal products with complementary mechanisms of action to improve glycaemic control in patients with type 2 diabetes: linagliptin, a dipeptidyl peptidase 4 (DPP-4) inhibitor, and metformin hydrochloride, a member of the biguanide class.
Mechanism of action: Linagliptin: Linagliptin is an inhibitor of the enzyme DPP-4 (Dipeptidyl peptidase 4) an enzyme which is involved in the inactivation of the incretin hormones GLP-1 and GIP (glucagon-like peptide-1, glucose-dependent insulinotropic polypeptide). These hormones are rapidly degraded by the enzyme DPP-4. Both incretin hormones are involved in the physiological regulation of glucose homeostasis. Incretins are secreted at a low basal level throughout the day and levels rise immediately after meal intake. GLP-1 and GIP increase insulin biosynthesis and secretion from pancreatic beta cells in the presence of normal and elevated blood glucose levels. Furthermore GLP-1 also reduces glucagon secretion from pancreatic alpha cells, resulting in a reduction in hepatic glucose output. Linagliptin binds very effectively to DPP-4 in a reversible manner and thus leads to a sustained increase and a prolongation of active incretin levels. Linagliptin glucose-dependently increases insulin secretion and lowers glucagon secretion thus resulting in an overall improvement in the glucose homeostasis. Linagliptin binds selectively to DPP-4 and exhibits a > 10,000-fold selectivity
versus DPP-8 or DPP-9 activity
in vitro.
Metformin: Metformin hydrochloride is a biguanide with antihyperglycaemic effects, lowering both basal and postprandial plasma glucose. It does not stimulate insulin secretion and therefore does not produce hypoglycaemia.
Metformin hydrochloride may act via 3 mechanisms: (1) reduction of hepatic glucose production by inhibiting gluconeogenesis and glycogenolysis; (2) in muscle, by increasing insulin sensitivity, improving peripheral glucose uptake and utilisation; (3) and delay of intestinal glucose absorption.
Metformin hydrochloride stimulates intracellular glycogen synthesis by acting on glycogen synthase.
Metformin hydrochloride increases the transport capacity of all types of membrane glucose transporters (GLUTs) known to date.
In humans, independently of its action on glycaemia, metformin hydrochloride has favourable effects on lipid metabolism. This has been shown at therapeutic doses in controlled, medium-term or long-term clinical studies: metformin hydrochloride reduces total cholesterol, LDL cholesterol and triglyceride levels.
Clinical efficacy and safety: Linagliptin as add-on to metformin therapy: The efficacy and safety of linagliptin in combination with metformin in patients with insufficient glycaemic control on metformin monotherapy was evaluated in a double-blind placebo-controlled study of 24 weeks duration. Linagliptin added to metformin provided significant improvements in HbA
1c, (-0.64% change compared to placebo), from a mean baseline HbA
1c of 8%. Linagliptin also showed significant improvements in fasting plasma glucose (FPG) by -21.1 mg/dl and 2-hour post-prandial glucose (PPG) by -67.1 mg/dl compared to placebo, as well as a greater portion of patients achieving a target HbA
1c of < 7.0% (28.3% on linagliptin
versus 11.4% on placebo). The observed incidence of hypoglycaemia in patients treated with linagliptin was similar to placebo. Body weight did not differ significantly between the groups.
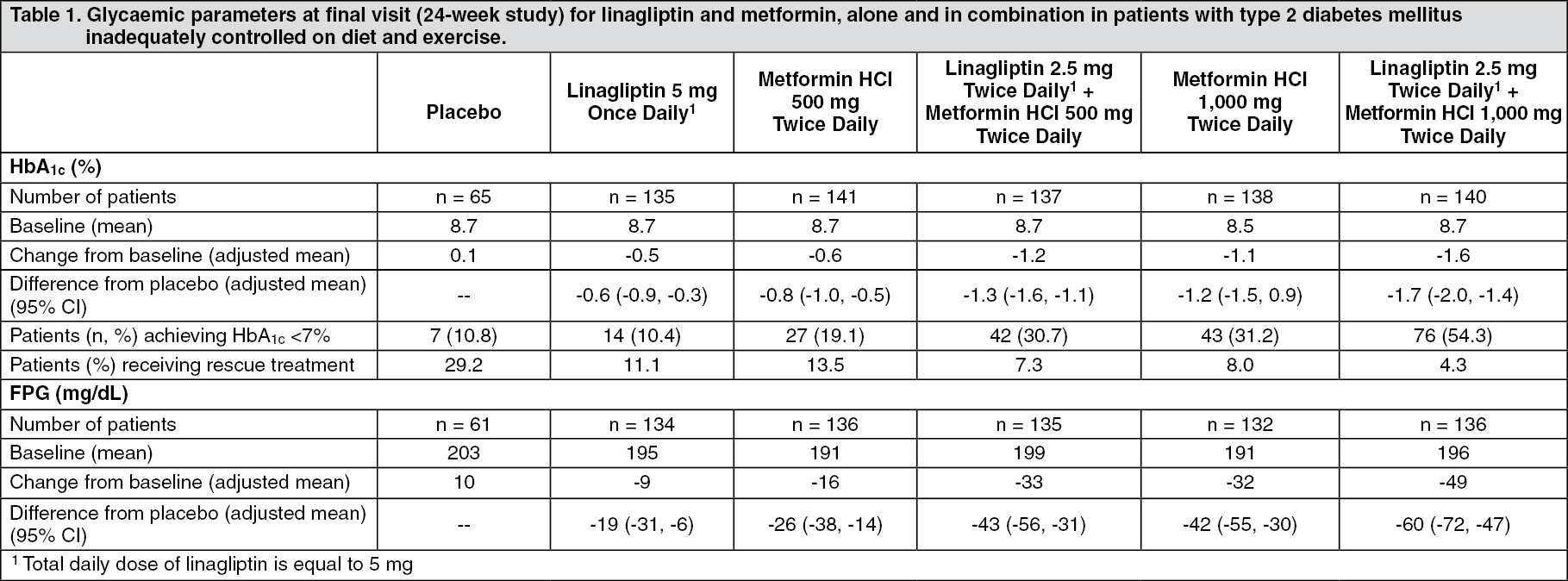
In a 24-week placebo-controlled factorial study of initial therapy, linagliptin 2.5 mg twice daily in combination with metformin (500 mg or 1,000 mg twice daily) provided significant improvements in glycaemic parameters compared with either monotherapy as summarised in Table 1 (mean baseline HbA
1c 8.65%). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Mean reductions from baseline in HbA
1c were generally greater for patients with higher baseline HbA
1c values. Effects on plasma lipids were generally neutral. The decrease in body weight with the combination of linagliptin and metformin was similar to that observed for metformin alone or placebo; there was no change in weight from baseline for patients on linagliptin alone. The incidence of hypoglycaemia was similar across treatment groups (placebo 1.4%, linagliptin 5 mg 0%, metformin 2.1%, and linagliptin 2.5 mg plus metformin twice daily 1.4%).
The efficacy and safety of linagliptin 2.5 mg twice daily versus 5 mg once daily in combination with metformin in patients with insufficient glycaemic control on metformin monotherapy was evaluated in a double-blind placebo-controlled study of 12 weeks duration. Linagliptin 5 mg once daily and 2.5 mg twice daily provided comparable (CI: -0.07; 0.19) significant HbA
1c reductions of -0.80% (from baseline 7.98%), and -0.74% (from baseline 7.96%) compared to placebo. The observed incidence of hypoglycaemia in patients treated with linagliptin was similar to placebo. Body weight did not differ significantly between the groups.
Linagliptin as add-on to a combination of metformin and sulphonylurea therapy: A placebo-controlled study of 24 weeks in duration was conducted to evaluate the efficacy and safety of linagliptin 5 mg to placebo, in patients not sufficiently treated with a combination with metformin and a sulphonylurea. Linagliptin provided significant improvements in HbA
1c (-0.62% change compared to placebo), from a mean baseline HbA
1c of 8.14%. Linagliptin also showed significant improvements in patients achieving a target HbA
1c of < 7.0% (31.2% on linagliptin versus 9.2% on placebo), and also for fasting plasma glucose (FPG) with -12.7 mg/dl reduction compared to placebo. Body weight did not differ significantly between the groups.
Linagliptin as add-on to a combination of metformin and empagliflozin therapy: In patients inadequately controlled with metformin and empagliflozin (10 mg (n=247) or 25 mg (n=217)), 24-weeks treatment with add-on therapy of linagliptin 5 mg provided adjusted mean HbA
1c reductions from baseline by -0.53% (significant difference to add-on placebo -0.32% (95% CI -0.52, -0.13) and -0.58% (significant difference to add-on placebo -0.47% (95% CI -0.66; -0.28), respectively. A statistically significant greater proportion of patients with a baseline HbA
1c ≥7.0% and treated with linagliptin 5 mg achieved a target HbA
1c of <7% compared to placebo.
Linagliptin in combination with metformin and insulin: A 24-week placebo-controlled study was conducted to evaluate the efficacy and safety of linagliptin (5 mg once daily) added to insulin with or without metformin. 83% of patients were taking metformin in combination with insulin in this trial. Linagliptin in combination with metformin plus insulin provided significant improvements in HbA
1c in this subgroup with -0.68% (CI: -0.78; -0.57) adjusted mean change from baseline (mean baseline HbA
1c 8.28%) compared to placebo in combination with metformin plus insulin. There was no meaningful change from baseline in body weight in either group.
Linagliptin 24-month data, as add-on to metformin in comparison with glimepiride: In a study comparing the efficacy and safety of the addition of linagliptin 5 mg or glimepiride (mean dose 3 mg) in patients with inadequate glycaemic control on metformin monotherapy, mean reductions in HbA
1c were -0.16% with linagliptin (mean baseline HbA
1c 7.69%) and -0.36% with glimepiride (mean baseline HbA
1c 7.69%) with a mean treatment difference of 0.20% (97.5% CI: 0.09, 0.299). The incidence of hypoglycaemia in the linagliptin group (7.5%) was significantly lower than that in the glimepiride group (36.1%). Patients treated with linagliptin exhibited a significant mean decrease from baseline in body weight compared to a significant weight gain in patients administered glimepiride (-1.39 versus +1.29 kg).
Linagliptin as add-on therapy in elderly (age ≥ 70 years) with type 2 diabetes: The efficacy and safety of linagliptin in elderly (age ≥ 70 years) with type 2 diabetes was evaluated in a double-blind study of 24 weeks duration. Patients received metformin and/or sulphonylurea and/or insulin as background therapy. Doses of background anti-diabetic therapy were kept stable during the first 12 weeks, after which adjustments were permitted. Linagliptin provided significant improvements in HbA
1c (-0.64% change compared to placebo after 24 weeks), from a mean baseline HbA
1c of 7.8%. Linagliptin also showed significant improvements in fasting plasma glucose (FPG) compared to placebo. Body weight did not differ significantly between the groups.
In a pooled analysis of elderly (age ≥ 70 years) patients with type 2 diabetes (n=183) who were taking both metformin and basal insulin as background therapy, linagliptin in combination with metformin plus insulin provided significant improvements in HbA
1c parameters with -0.81% (CI: -1.01; -0.61) adjusted mean change from baseline (mean baseline HbA
1c 8.13%) compared to placebo in combination with metformin plus insulin.
Linagliptin cardiovascular and renal safety study (CARMELINA): CARMELINA was a randomized study in 6979 patients with type 2 diabetes with increased CV risk evidenced by a history of established macrovascular or renal disease who were treated with linagliptin 5 mg (3494) or placebo (3485) added to standard of care targeting regional standards for HbA
1c, CV risk factors and renal disease. The study population included 1211 (17.4%) patients ≥ 75 years of age and 4348 (62.3%) patients with renal impairment. Approximately 19% of the population had eGFR ≥45 to <60 mL/min/1.73 m
2, 28% of the population had eGFR ≥30 to <45 mL/min/1.73 m
2) and 15% had eGFR < 30 mL/min/1.73 m
2. The mean HbA
1c at baseline was 8.0%.
The study was designed to demonstrate non-inferiority for the primary cardiovascular endpoint which was a composite of the first occurrence of cardiovascular death or a non-fatal myocardial infarction (MI) or a non-fatal stroke (3P-MACE). The renal composite endpoint was defined as renal death or sustained end stage renal disease or sustained decrease of 40% or more in eGFR.
After a median follow up of 2.2 years, linagliptin, when added to standard of care, did not increase the risk of major adverse cardiovascular events or renal outcome events. There was no increased risk in hospitalization for heart failure which was an additional adjudicated endpoint observed compared to standard of care without linagliptin in patients with type 2 diabetes (Table 2). (See Table 2.)
Click on icon to see table/diagram/image
In analyses for albuminuria progression (change from normoalbuminuria to micro- or macroalbuminuria, or from microalbuminuria to macroalbuminuria) the estimated hazard ratio was 0.86 (95% CI 0.78, 0.95) for linagliptin versus placebo.
Linagliptin cardiovascular safety study (CAROLINA): CAROLINA was a randomized study in 6033 patients with early type 2 diabetes and increased CV risk or established complications who were treated with linagliptin 5 mg (3023) or glimepiride 1-4 mg (3010) added to standard of care (including background therapy with metformin in 83% of patients) targeting regional standards for HbA
1c and CV risk factors. The mean age for study population was 64 years and included 2030 (34%) patients ≥ 70 years of age. The study population included 2089 (35%) patients with cardiovascular disease and 1130 (19%) patients with renal impairment with an eGFR < 60ml/min/1.73m
2 at baseline. The mean HbA
1c at baseline was 7.15%.
The study was designed to demonstrate non-inferiority for the primary cardiovascular endpoint which was a composite of the first occurrence of cardiovascular death or a non-fatal myocardial infarction (MI) or a non-fatal stroke (3P-MACE).
After a median follow up of 6.25 years, linagliptin, when added to standard of care, did not increase the risk of major adverse cardiovascular events (Table 3) as compared to glimepiride. Results were consistent for patients treated with or without metformin. (See Table 3.)
Click on icon to see table/diagram/image
For the entire treatment period (median time on treatment 5.9 years) the rate of patients with moderate or severe hypoglycaemia was 6.5% on linagliptin versus 30.9% on glimepiride, severe hypoglycaemia occurred in 0.3% of patients on linagliptin versus 2.2% on glimepiride.
Metformin: The prospective randomised (UKPDS) study has established the long-term benefit of intensive blood glucose control in type 2 diabetes. Analysis of the results for overweight patients treated with metformin after failure of diet alone showed: A significant reduction of the absolute risk of any diabetes-related complication in the metformin group (29.8 events/1,000 patient-years)
versus diet alone (43.3 events/1,000 patient-years), p=0.0023, and
versus the combined sulphonylurea and insulin monotherapy groups (40.1 events/1,000 patient-years), p=0.0034.
A significant reduction of the absolute risk of any diabetes-related mortality: metformin 7.5 events/1,000 patient-years, diet alone 12.7 events/1,000 patient-years, p=0.017.
A significant reduction of the absolute risk of overall mortality: metformin 13.5 events/1,000 patient-years
versus diet alone 20.6 events/1,000 patient-years, (p=0.011), and
versus the combined sulphonylurea and insulin monotherapy groups 18.9 events/1,000 patient-years (p=0.021).
A significant reduction in the absolute risk of myocardial infarction: metformin 11 events/1,000 patient-years, diet alone 18 events/1,000 patient-years, (p=0.01).
Paediatric population: The European Medicines Agency has waived the obligation to submit the results of the studies with Trajenta Duo in all subsets of the paediatric population in type 2 diabetes (see Dosage & Administration for information on paediatric use).
Pharmacokinetics: Bioequivalence studies in healthy subjects demonstrated that the Trajenta Duo (linagliptin/metformin hydrochloride) combination tablets are bioequivalent to co-administration of linagliptin and metformin hydrochloride as individual tablets.
Administration of Trajenta Duo 2.5/1,000 mg with food resulted in no change in overall exposure of linagliptin. With metformin there was no change in AUC, however mean peak serum concentration of metformin was decreased by 18% when administered with food. A delayed time to peak serum concentrations by 2 hours was observed for metformin under fed conditions. These changes are not likely to be clinically meaningful.
The following statements reflect the pharmacokinetic properties of the individual active substances of Trajenta Duo.
Linagliptin: The pharmacokinetics of linagliptin has been extensively characterised in healthy subjects and patients with type 2 diabetes. After oral administration of a 5 mg dose to healthy volunteers or patients, linagliptin was rapidly absorbed, with peak plasma concentrations (median T
max) occurring 1.5 hours post-dose.
Plasma concentrations of linagliptin decline in a triphasic manner with a long terminal half-life (terminal half-life for linagliptin more than 100 hours), that is mostly related to the saturable, tight binding of linagliptin to DPP-4 and does not contribute to the accumulation of the active substance. The effective half-life for accumulation of linagliptin, as determined from oral administration of multiple doses of 5 mg linagliptin, is approximately 12 hours. After once daily dosing of 5 mg linagliptin, steady-state plasma concentrations are reached by the third dose. Plasma AUC of linagliptin increased approximately 33% following 5 mg doses at steady-state compared to the first dose. The intra-subject and inter-subject coefficients of variation for linagliptin AUC were small (12.6% and 28.5%, respectively). Due to the concentration dependent binding of linagliptin to DPP-IV, the pharmacokinetics of linagliptin based on total exposure is not linear; indeed total plasma AUC of linagliptin increased in a less than dose-proportional manner, while unbound AUC increases in a roughly dose proportional manner. The pharmacokinetics of linagliptin was generally similar in healthy subjects and in patients with type 2 diabetes.
Absorption: The absolute bioavailability of linagliptin is approximately 30%. Co-administration of a high-fat meal with linagliptin prolonged the time to reach C
max by 2 hours and lowered C
max by 15%, but no influence on AUC
0-72h was observed. No clinically relevant effect of C
max and T
max changes is expected; therefore linagliptin may be administered with or without food.
Distribution: As a result of tissue binding, the mean apparent volume of distribution at steady-state following a single 5 mg intravenous dose of linagliptin to healthy subjects is approximately 1110 litres, indicating that linagliptin extensively distributes to the tissues. Plasma protein binding of linagliptin is concentration-dependent, decreasing from about 99% at 1 nmol/l to 75-89% at ≥ 30 nmol/l, reflecting saturation of binding to DPP-4 with increasing concentration of linagliptin. At high concentrations, where DPP-4 is fully saturated, 70-80% of linagliptin was bound to other plasma proteins than DPP-4, hence 20-30% were unbound in plasma.
Biotransformation: Following a [
14C] linagliptin oral 10 mg dose, approximately 5% of the radioactivity was excreted in urine. Metabolism plays a subordinate role in the elimination of linagliptin. One main metabolite with a relative exposure of 13.3% of linagliptin at steady-state was detected which was found to be pharmacologically inactive, and thus does not contribute to the plasma DPP-4 inhibitory activity of linagliptin.
Elimination: Following administration of an oral [
14C] linagliptin dose to healthy subjects, approximately 85% of the administered radioactivity was eliminated in faeces (80%) or urine (5%) within 4 days of dosing. Renal clearance at steady-state was approximately 70 ml/min.
Renal impairment: Under steady-state conditions, linagliptin exposure in patients with mild renal impairment was comparable to healthy subjects. In moderate renal impairment, a moderate increase in exposure of about 1.7-fold was observed compared with control. Exposure in T2DM patients with severe RI was increased by about 1.4-fold compared to T2DM patients with normal renal function. Steady-state predictions for AUC of linagliptin in patients with ESRD indicated comparable exposure to that of patients with moderate or severe renal impairment. In addition, linagliptin is not expected to be eliminated to a therapeutically significant degree by hemodialysis or peritoneal dialysis. No dose adjustment of linagliptin is recommended in patients with renal impairment; therefore, linagliptin may be continued as a single entity tablet at the same total daily dose of 5 mg if Trajenta Duo is discontinued due to evidence of renal impairment.
Hepatic impairment: In patients with mild moderate and severe hepatic impairment (according to the Child-Pugh classification), mean AUC and C
max of linagliptin were similar to healthy matched controls following administration of multiple 5 mg doses of linagliptin.
Body Mass Index (BMI): Body mass index had no clinically relevant effect on the pharmacokinetics of linagliptin based on a population pharmacokinetic analysis of Phase I and Phase II data. The clinical trials before marketing authorization have been performed up to a BMI equal to 40 kg/m
2.
Gender: Gender had no clinically relevant effect on the pharmacokinetics of linagliptin based on a population pharmacokinetic analysis of Phase I and Phase II data.
Elderly: Age did not have a clinically relevant impact on the pharmacokinetics of linagliptin based on a population pharmacokinetic analysis of Phase I and Phase II data. Older subjects (65 to 80 years, oldest patient was 78 years) had comparable plasma concentrations of linagliptin compared to younger subjects. Linagliptin trough concentrations were also measured in elderly (age ≥ 70 years) with type 2 diabetes in a phase III study of 24 weeks duration. Linagliptin concentrations in this study were within the range of values previously observed in younger type 2 diabetes patients.
Paediatric population: A paediatric Phase 2 study examined the pharmacokinetics and pharmacodynamics of 1 mg and 5 mg linagliptin in children and adolescents ≥10 to <18 years of age with type 2 diabetes mellitus. The observed pharmacokinetic and pharmacodynamic responses were consistent with those found in adult subjects. Linagliptin 5 mg showed superiority over 1 mg with regard to trough DPP-4 inhibition (72% vs 32%, p=0.0050) and a numerically larger reduction with regard to adjusted mean change from baseline in HbA
1c (-0.63% vs -0.48%, n.s.). Due to the limited nature of the data set the results should be interpreted cautiously.
Race: Race had no obvious effect on the plasma concentrations of linagliptin based on a composite analysis of available pharmacokinetic data, including patients of Caucasian, Hispanic, African, and Asian origin. In addition the pharmacokinetic characteristics of linagliptin were found to be similar in dedicated phase I studies in Japanese, Chinese and Caucasian healthy subjects and African American type 2 diabetes patients.
Metformin: Absorption: After an oral dose of metformin, T
max is reached in 2.5 hours. Absolute bioavailability of a 500 mg or 850 mg metformin hydrochloride tablet is approximately 50-60% in healthy subjects. After an oral dose, the non-absorbed fraction recovered in faeces was 20-30%.
After oral administration, metformin hydrochloride absorption is saturable and incomplete. It is assumed that the pharmacokinetics of metformin hydrochloride absorption are non-linear.
At the recommended metformin hydrochloride doses and dosing schedules, steady-state plasma concentrations are reached within 24 to 48 hours and are generally less than 1 microgram/ml. In controlled clinical trials, maximum metformin hydrochloride plasma levels (C
max) did not exceed 5 microgram/ml, even at maximum doses.
Food decreases the extent and slightly delays the absorption of metformin hydrochloride. Following administration of a dose of 850 mg, a 40% lower plasma peak concentration, a 25% decrease in AUC (area under the curve) and a 35-minute prolongation of the time to peak plasma concentration were observed. The clinical relevance of these decreases is unknown.
Distribution: Plasma protein binding is negligible. Metformin hydrochloride partitions into erythrocytes. The blood peak is lower than the plasma peak and appears at approximately the same time. The red blood cells most likely represent a secondary compartment of distribution. The mean volume of distribution (Vd) ranged between 63-276 l.
Biotransformation: Metformin hydrochloride is excreted unchanged in the urine. No metabolites have been identified in humans.
Elimination: Renal clearance of metformin hydrochloride is > 400 ml/min, indicating that metformin hydrochloride is eliminated by glomerular filtration and tubular secretion. Following an oral dose, the apparent terminal elimination half-life is approximately 6.5 hours.
When renal function is impaired, renal clearance is decreased in proportion to that of creatinine and thus the elimination half-life is prolonged, leading to increased levels of metformin hydrochloride in plasma.
Paediatric population: Single dose study: After single doses of metformin hydrochloride 500 mg, paediatric patients have shown a similar pharmacokinetic profile to that observed in healthy adults.
Multiple-dose study: Data are restricted to one study. After repeated doses of 500 mg twice daily for 7 days in paediatric patients the peak plasma concentration (C
max) and systemic exposure (AUC
0-t) were reduced by approximately 33% and 40%, respectively compared to diabetic adults who received repeated doses of 500 mg twice daily for 14 days. As the dose is individually titrated based on glycaemic control, this is of limited clinical relevance.
Toxicology: Preclinical safety data: Linagliptin plus metformin: General toxicity studies in rats for up to 13 weeks were performed with the co-administration of linagliptin and metformin. The only observed interaction between linagliptin and metformin was a reduction of body weight gain. No other additive toxicity caused by the combination of linagliptin and metformin was observed at AUC exposure levels up to 2 and 23 times human exposure, respectively.
An embryofetal development study in pregnant rats did not indicate a teratogenic effect attributed to the co-administration of linagliptin and metformin at AUC exposure levels up to 4 and 30 times human exposure, respectively.
Linagliptin: Liver, kidneys and gastrointestinal tract are the principal target organs of toxicity in mice and rats at repeat doses of linagliptin of more than 300 times the human exposure.
In rats, effects on reproductive organs, thyroid and the lymphoid organs were seen at more than 1500 times human exposure. Strong pseudo-allergic reactions were observed in dogs at medium doses, secondarily causing cardiovascular changes, which were considered dog-specific. Liver, kidneys, stomach, reproductive organs, thymus, spleen, and lymph nodes were target organs of toxicity in Cynomolgus monkeys at more than 450 times human exposure. At more than 100 times human exposure, irritation of the stomach was the major finding in these monkeys.
Linagliptin and its main metabolite did not show a genotoxic potential.
Oral 2-year carcinogenicity studies in rats and mice revealed no evidence of carcinogenicity in rats or male mice. A significantly higher incidence of malignant lymphomas only in female mice at the highest dose (> 200 times human exposure) is not considered relevant for humans (explanation: non-treatment related but due to highly variable background incidence). Based on these studies there is no concern for carcinogenicity in humans.
The NOAEL for fertility, early embryonic development and teratogenicity in rats was set at > 900 times the human exposure. The NOAEL for maternal-, embryo-fetal-, and offspring toxicity in rats was 49 times human exposure. No teratogenic effects were observed in rabbits at > 1,000 times human exposure. A NOAEL of 78 times human exposure was derived for embryo-fetal toxicity in rabbits, and for maternal toxicity the NOAEL was 2.1 times human exposure. Therefore, it is considered unlikely that linagliptin affects reproduction at therapeutic exposures in humans.
Metformin: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction and development.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image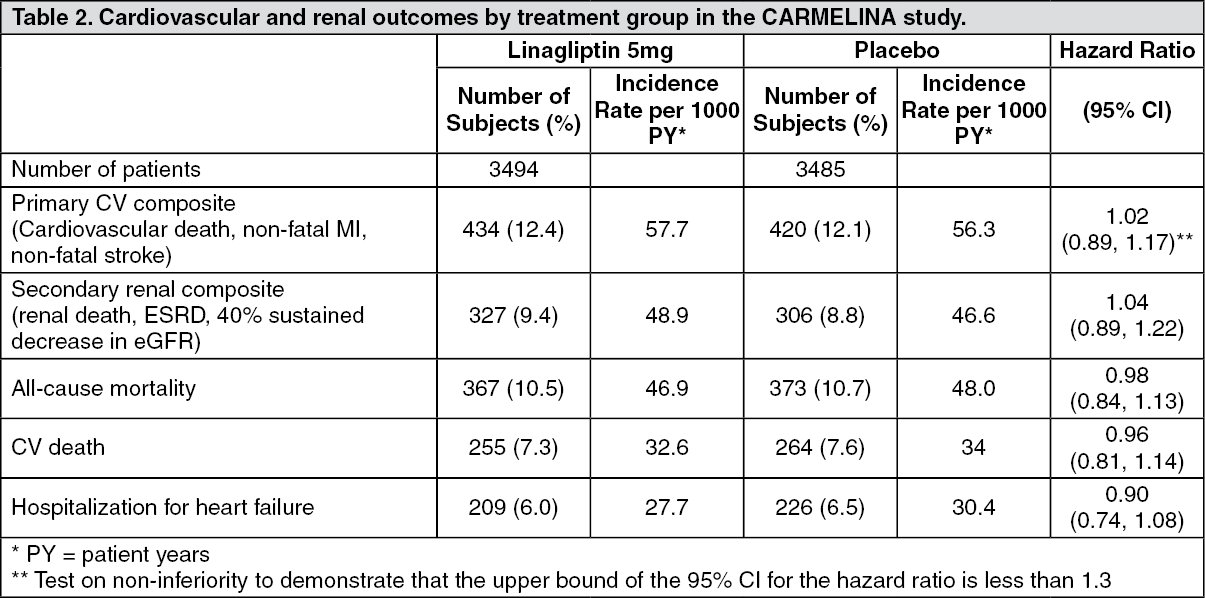 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image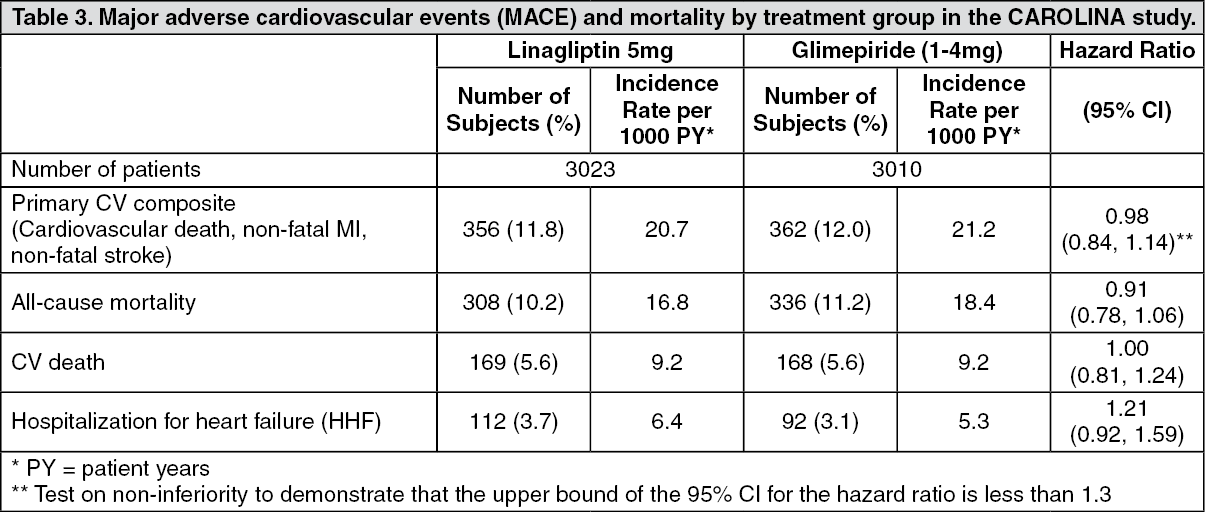 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image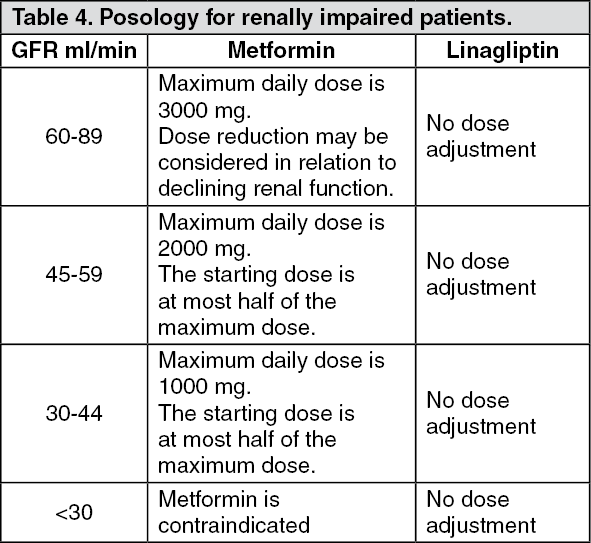 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out