Pharmacotherapeutic group: Alclav Neo: Combinations of penicillins, including beta-lactamase inhibitors.
Pharmacology: Pharmacodynamics: Mechanism of Action: Alclav Neo 625 mg/Alclav Kids/Alclav Hospi: Amoxicillin is a semisynthetic penicillin (beta-lactam antibiotic) that inhibits one or more enzymes (often referred to as penicillin-binding proteins, PBPs) in the biosynthetic pathway of bacterial peptidoglycan, which is an integral structural component of the bacterial cell wall. Inhibition of peptidoglycan synthesis leads to weakening of the cell wall, which is usually followed by cell lysis and death.
Amoxicillin is susceptible to degradation by beta-lactamases produced by resistant bacteria and therefore the spectrum of activity of amoxicillin alone does not include organisms which produce these enzymes.
Clavulanic acid is a beta-lactam structurally related to penicillins. It inactivates some beta-lactamase enzymes thereby preventing inactivation of amoxicillin. Clavulanic acid alone does not exert a clinically useful antibacterial effect.
Alclav Neo 1 g: Co-amoxiclav is a novel concept in antibiotic therapy. Resistance to many antibiotics is caused by bacterial enzymes which destroy the antibiotic before it can act on the pathogen. The clavulanate anticipates this defense mechanism by blocking the β-lactamase enzymes, thus rendering the organisms sensitive to amoxicillin's rapid bactericidal effect at concentrations readily attainable in the body. Clavulanate by itself has little antibacterial activity; however, in association with amoxicillin, it produces a novel antibiotic agent of broad spectrum with wide application in hospital and general practice.
Pharmacokinetics: Alclav Neo: Absorption: Amoxicillin and clavulanic acid, are fully dissociated in aqueous solution at physiological pH. Both components are rapidly and well absorbed by the oral route of administration. Following oral administration, amoxicillin and clavulanic acid are approximately 70% bioavailable. The plasma profiles of both components are similar and the time to peak plasma concentration (Tmax) in each case is approximately one hour.
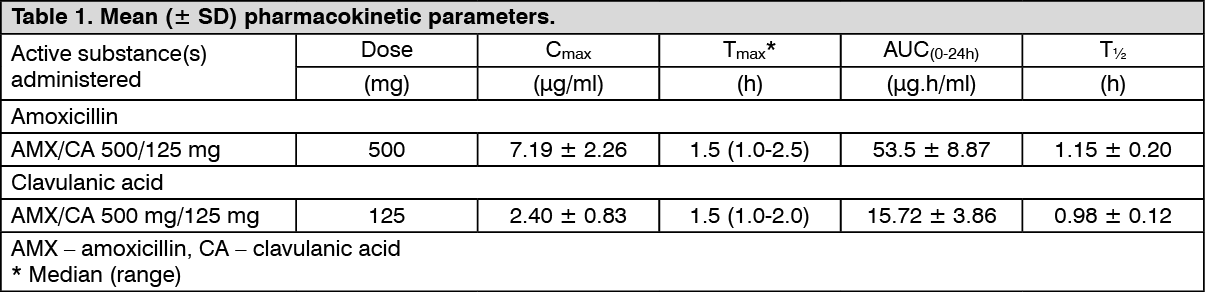
The pharmacokinetic results for a study, in which amoxicillin/clavulanic acid (500 mg/125 mg tablets three times daily) was administered in the fasting state to groups of healthy volunteers are presented as follows.
625 mg: See Table 1.
 Click on icon to see table/diagram/image
1 g:
Click on icon to see table/diagram/image
1 g: See Table 2.
Click on icon to see table/diagram/image
Amoxicillin and clavulanic acid serum concentrations achieved with amoxicillin/clavulanic acid are similar to those produced by the oral administration of equivalent doses of amoxicillin or clavulanic acid alone.
Distribution: About 25% of total plasma clavulanic acid and 18% of total plasma amoxicillin is bound to protein. The apparent volume of distribution is around 0.3-0.4 l/kg for amoxicillin and around 0.2 l/kg for clavulanic acid.
Following intravenous administration, both amoxicillin and clavulanic acid have been found in gall bladder, abdominal tissue, skin, fat, muscle tissues, synovial and peritoneal fluids, bile and pus. Amoxicillin does not adequately distribute into the cerebrospinal fluid.
From animal studies there is no evidence for significant tissue retention of drug-derived material for either component. Amoxicillin, like most penicillins, can be detected in breast milk. Trace quantities of clavulanic acid can also be detected in breast milk.
Both amoxicillin and clavulanic acid have been shown to cross the placental barrier.
Biotransformation: Amoxicillin is partly excreted in the urine as the inactive penicilloic acid in quantities equivalent to up to 10 to 25% of the initial dose. Clavulanic acid is extensively metabolized in man and eliminated in urine and faeces, and as carbon dioxide in expired air.
Elimination: The major route of elimination for amoxicillin is via the kidney, whereas for clavulanic acid it is by both renal and non-renal mechanisms.
Amoxicillin/clavulanic acid has a mean elimination half-life of approximately one hour and a mean total clearance of approximately 25 l/h in healthy subjects. Approximately 60 to 70% of the amoxicillin and approximately 40 to 65% of the clavulanic acid are excreted unchanged in urine during the first 6 h after administration of single co-amoxiclav 250 mg/125 mg or 500 mg/125 mg tablets. Various studies have found the urinary excretion to be 50-85% for amoxicillin and between 27-60% for clavulanic acid over a 24 hour period. In the case of clavulanic acid, the largest amount of drug is excreted during the first 2 hours after administration.
Concomitant use of probenecid delays amoxicillin excretion but does not delay renal excretion of clavulanic acid.
1 g: Age: The elimination half-life of amoxicillin is similar for children aged around 3 months to 2 years and older children and adults. For very young children (including preterm newborns) in the first week of life, the interval of administration should not exceed twice daily administration due to immaturity of the renal pathway of elimination. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
Gender: Following oral administration of amoxicillin/clavulanic acid to healthy males and female subjects, gender has no significant impact on the pharmacokinetics of either amoxicillin or clavulanic acid.
Renal impairment: The total serum clearance of amoxicillin/clavulanic acid decreases proportionately with decreasing renal function. The reduction in drug clearance is more pronounced for amoxicillin than for clavulanic acid, as a higher proportion of amoxicillin is excreted via the renal route. Doses in renal impairment must therefore prevent undue accumulation of amoxicillin while maintaining adequate levels of clavulanic acid.
Hepatic impairment: Hepatically impaired patients should be dosed with caution and hepatic function monitored at regular intervals.
Alclav Kids: Absorption: Amoxicillin and clavulanic acid, are fully dissociated in aqueous solution at physiological pH. Both components are rapidly and well absorbed by the oral route of administration. Following oral administration, amoxicillin and clavulanic acid are approximately 70% bioavailable. The plasma profiles of both components are similar and the time to peak plasma concentration (Tmax) in each case is approximately one hour.
The pharmacokinetic results for a study, in which amoxicillin/clavulanic acid (875 mg/125 mg tablets given twice daily) was administered in the fasting state to groups of healthy volunteers are presented as follows. (See Table 3.)
Click on icon to see table/diagram/image
Amoxicillin and clavulanic acid serum concentrations achieved with amoxicillin/clavulanic acid are similar to those produced by the oral administration of equivalent doses of amoxicillin or clavulanic acid alone.
Distribution: About 25% of total plasma clavulanic acid and 18% of total plasma amoxicillin is bound to protein. The apparent volume of distribution is around 0.3-0.4 l/kg for amoxicillin and around 0.2 l/kg for clavulanic acid.
Following intravenous administration, both amoxicillin and clavulanic acid have been found in gall bladder, abdominal tissue, skin, fat, muscle tissues, synovial and peritoneal fluids, bile and pus. Amoxicillin does not adequately distribute into the cerebrospinal fluid.
From animal studies there is no evidence for significant tissue retention of drug-derived material for either component. Amoxicillin, like most penicillins, can be detected in breast milk. Trace quantities of clavulanic acid can also be detected in breast milk.
Both amoxicillin and clavulanic acid have been shown to cross the placental barrier.
Biotransformation: Amoxicillin is partly excreted in the urine as the inactive penicilloic acid in quantities equivalent to up to 10 to 25% of the initial dose. Clavulanic acid is extensively metabolized in man and eliminated in urine and faeces, and as carbon dioxide in expired air.
Elimination: The major route of elimination for amoxicillin is via the kidney, whereas for clavulanic acid it is by both renal and non-renal mechanisms.
Amoxicillin/clavulanic acid has a mean elimination half-life of approximately one hour and a mean total clearance of approximately 25 l/h in healthy subjects. Approximately 60 to 70% of the amoxicillin and approximately 40 to 65% of the clavulanic acid are excreted unchanged in urine during the first 6 h after administration of single Co-amoxiclav 400/57 mg/5 ml Powder for Oral Suspension 250 mg/125 mg or 500 mg/125 mg tablets. Various studies have found the urinary excretion to be 50-85% for amoxicillin and between 27-60% for clavulanic acid over a 24 hour period. In the case of clavulanic acid, the largest amount of drug is excreted during the first 2 hours after administration.
Concomitant use of probenecid delays amoxicillin excretion but does not delay renal excretion of clavulanic acid.
Age: The elimination half-life of amoxicillin is similar for children aged around 3 months to 2 years and older children and adults. For very young children (including preterm newborns) in the first week of life the interval of administration should not exceed twice daily administration due to immaturity of the renal pathway of elimination. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
Gender: Following oral administration of amoxicillin/clavulanic acid to healthy males and female subjects, gender has no significant impact on the pharmacokinetics of either amoxicillin or clavulanic acid.
Renal impairment: The total serum clearance of amoxicillin/clavulanic acid decreases proportionately with decreasing renal function.
The reduction in drug clearance is more pronounced for amoxicillin than for clavulanic acid, as a higher proportion of amoxicillin is excreted via the renal route. Doses in renal impairment must therefore prevent undue accumulation of amoxicillin while maintaining adequate levels of clavulanic acid.
Hepatic impairment: Hepatically impaired patients should be dosed with caution and hepatic function monitored at regular intervals.
Alclav Hospi: Absorption: The pharmacokinetic results for studies in which amoxicillin/clavulanic acid was administered to groups of healthy volunteers as either 500 mg/100 mg or 1000 mg/200 mg given as a bolus intravenous injection are presented as follows. (See Table 4.)
Click on icon to see table/diagram/image
Distribution: About 25% of total plasma clavulanic acid and 18% of total plasma amoxicillin is bound to protein. The apparent volume of distribution is around 0.3-0.4 L/Kg for amoxicillin and around 0.2 L/Kg for clavulanic acid.
Following intravenous administration, both amoxicillin and clavulanic acid have been found in gall bladder, abdominal tissue, skin, fat, muscle tissues, synovial and peritoneal fluids, bile and pus. Amoxicillin does not adequately distribute into the cerebrospinal fluid.
From animal studies, there is no evidence for significant tissue retention of drug-derived material for either component. Amoxicillin, like most penicillins, can be detected in breast milk. Trace quantities of clavulanic acid can also be detected in breast milk.
Biotransformation: Amoxicillin is partly excreted in the urine as the inactive penicilloic acid in quantities equivalent to up
to 10 to 25% of the initial dose. Clavulanic acid is extensively metabolized in man and eliminated in urine and faeces, and as carbon dioxide in expired air.
Elimination: The major route of elimination for amoxicillin is via the kidney, whereas for clavulanic acid it is by both renal and non-renal mechanisms.
Amoxicillin/clavulanic acid has a mean elimination half-life of approximately one hour and a mean total clearance of approximately 25 l/h in healthy subjects. Approximately 60 to 70% of the amoxicillin and approximately 40 to 65% of the clavulanic acid are excreted unchanged in urine during the first 6 h after administration of a single 500/100 mg or a single 1000/200 mg bolus intravenous injection. Various studies have found the urinary excretion to be 50-85% for amoxicillin and between 27-60% for clavulanic acid over a 24 hour period. In the case of clavulanic acid, the largest amount of drug is excreted during the first 2 hours after administration. Concomitant use of probenecid delays amoxicillin excretion but does not delay renal excretion of clavulanic acid.
Age: The elimination half-life of amoxicillin is similar for children aged around 3 months to 2 years and older children and adults. For very young children (including preterm newborns) in the first week of life the interval of administration should not exceed twice daily administration due to immaturity of the renal pathway of elimination. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
Renal impairment: The total serum clearance of amoxicillin/clavulanic acid decreases proportionately with decreasing renal function. The reduction in drug clearance is more pronounced for amoxicillin than for clavulanic acid, as a higher proportion of amoxicillin is excreted via the renal route. Doses in renal impairment must therefore prevent undue accumulation of amoxicillin while maintaining adequate levels of clavulanic acid.
Hepatic impairment: Hepatically impaired patients should be dosed with caution and hepatic function monitored at regular intervals.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image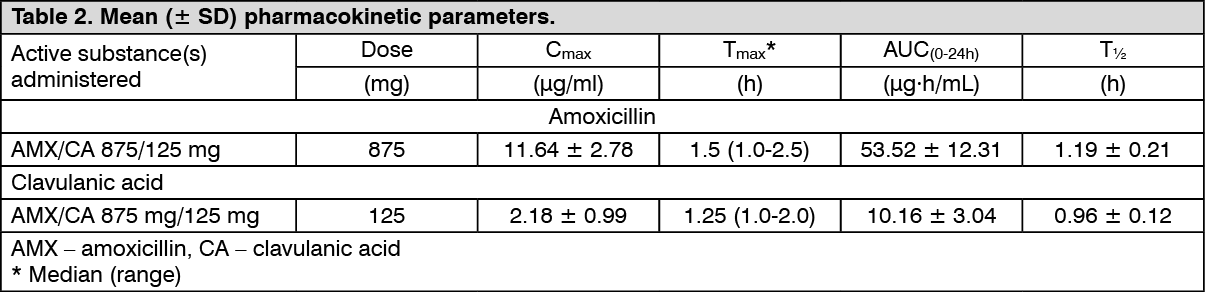 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image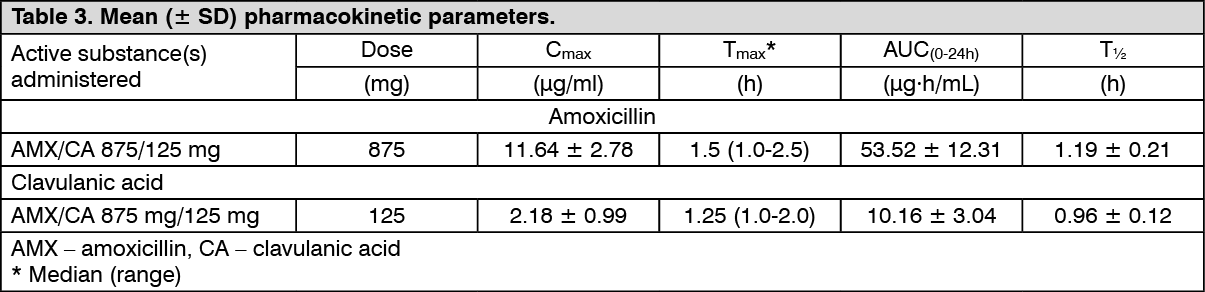 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image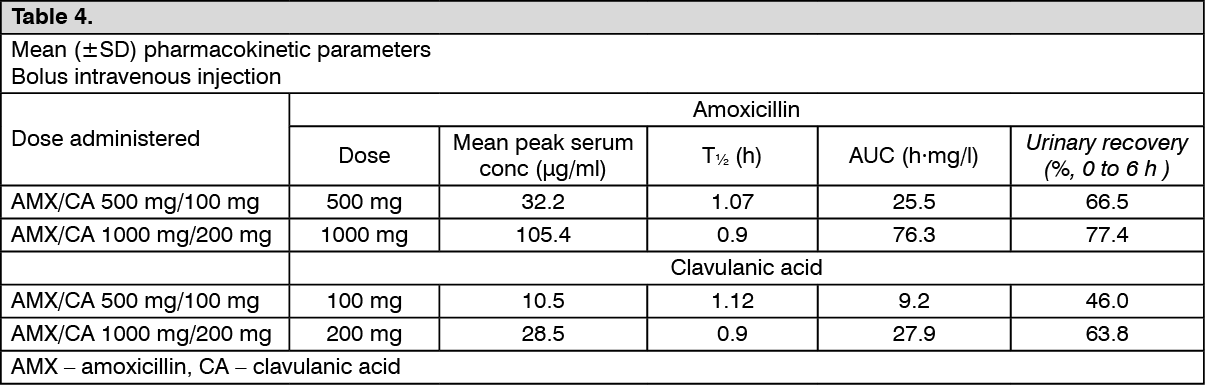 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image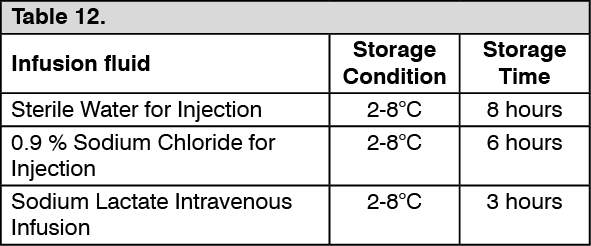 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out