Olmesartan medoxomil, amlodipine besilate.
Each film coated tablet contains: Olmesartan medoxomil, USP 20 mg; Amlodipine (as besilate), BP 5 mg.
Olmesartan medoxomil, USP 20 mg; Amlodipine (as besilate), BP 10 mg.
Olmesartan medoxomil, USP 40 mg; Amlodipine (as besilate), BP 5 mg.
Olmesartan medoxomil, USP 40 mg; Amlodipine (as besilate), BP 10 mg.
Angiotensin II Receptor Blocker/Calcium Channel Blocker.
Pharmacology: Pharmacodynamics: Mechanism of Action: Olmesartan medoxomil plus Amlodipine combination is a combination of an angiotensin II receptor antagonist, Olmesartan medoxomil, and a calcium channel blocker, amlodipine besilate. The combination of these active ingredients has an additive antihypertensive effect, reducing blood pressure to a greater degree than either component alone.
Pharmacokinetics: Olmesartan medoxomil plus Amlodipine combination: Following oral intake of Olmesartan medoxomil plus Amlodipine combination, peak plasma concentrations of olmesartan and amlodipine are reached at 1.5 - 2 h and 6 - 8 hours, respectively. The rate and extent of absorption of the two active substances from Olmesartan medoxomil plus Amlodipine combination are equivalent to the rate and extent of absorption following intake of the two components as separate tablets. Food does not affect the bioavailability of olmesartan and amlodipine from Olmesartan medoxomil plus Amlodipine combination.
Olmesartan medoxomil (active ingredient of Olmesartan medoxomil plus Amlodipine combination): Absorption and distribution: Olmesartan medoxomil is a prodrug. It is rapidly converted to the pharmacologically active metabolite, olmesartan, by esterases in the gut mucosa and in portal blood during absorption from the gastrointestinal tract. No intact Olmesartan medoxomil or intact side chain medoxomil moiety have been detected in plasma or excreta. The mean absolute bioavailability of olmesartan from a tablet formulation was 25.6%.
The mean peak plasma concentration (Cmax) of olmesartan is reached within about 2 hours after oral dosing with Olmesartan medoxomil, and olmesartan plasma concentrations increase approximately linearly with increasing single oral doses up to about 80 mg.
Food had minimal effect on the bioavailability of olmesartan and therefore Olmesartan medoxomil may be administered with or without food.
No clinically relevant gender-related differences in the pharmacokinetics of olmesartan have been observed.
Olmesartan is highly bound to plasma protein (99.7%), but the potential for clinically significant protein binding displacement interactions between olmesartan and other highly bound co-administered active substances is low (as confirmed by the lack of a clinically significant interaction between Olmesartan medoxomil and warfarin). The binding of olmesartan to blood cells is negligible. The mean volume of distribution after intravenous dosing is low (16 - 29 L).
Biotransformation and elimination: Total plasma clearance of olmesartan was typically 1.3 L/h (CV, 19%) and was relatively slow compared to hepatic blood flow (ca 90 L/h). Following a single oral dose of 14C-labelled Olmesartan medoxomil, 10% - 16% of the administered radioactivity was excreted in the urine (the vast majority within 24 hours of dose administration) and the remainder of the recovered radioactivity was excreted in the faeces. Based on the systemic availability of 25.6%, it can be calculated that absorbed olmesartan is cleared by both renal excretion (ca 40%) and hepato-biliary excretion (ca 60%). All recovered radioactivity was identified as olmesartan. No other significant metabolite was detected. Enterohepatic recycling of olmesartan is minimal. Since a large proportion of olmesartan is excreted via the biliary route, use in patients with biliary obstruction is contraindicated.
The terminal elimination half-life of olmesartan is between 10 and 15 hours after multiple oral dosing. Steady state is reached after the first few doses and no further accumulation is evident after 14 days of repeated dosing. Renal clearance is approximately 0.5 - 0.7 L/h and is independent of dose.
Amlodipine (active ingredient of Olmesartan medoxomil plus Amlodipine combination): Absorption and distribution: After oral administration of therapeutic doses, amlodipine is well absorbed with peak blood levels between 6-12 hours post dose. Absolute bioavailability has been estimated to be between 64 and 80%. The volume of distribution is approximately 21 l/kg. In vitro studies have shown that approximately 97.5% of circulating amlodipine is bound to plasma proteins.
The absorption of amlodipine is unaffected by the concomitant intake of food.
Biotransformation and elimination: The terminal plasma elimination half-life is about 35-50 hours and is consistent with once daily dosing. Amlodipine is extensively metabolized by the liver to inactive metabolites with 10% of the parent compound and 60% of metabolites excreted in the urine.
Olmesartan medoxomil plus Amlodipine combination is indicated for the treatment of hypertension, alone or with other antihypertensive agents. This fixed combination drug is indicated as initial therapy in patients likely to need multiple anti-hypertensive agents to achieve their blood pressure goals. Initial therapy is not recommended in patients ≥75 years of age or in hepatically impaired patients.
Adults: The recommended dosage of Olmesartan medoxomil plus Amlodipine combination is 1 tablet per day.
The usual starting dose is 20/5mg once daily. The dosage can be increased after 1 to 2 weeks of therapy to maximum dose of 40/10mg tablet once daily as needed to control blood pressure.
For convenience, patients receiving Olmesartan medoxomil and amlodipine from separate tablets may be switched to Olmesartan medoxomil plus Amlodipine combination tablets containing the same component doses.
Olmesartan medoxomil plus Amlodipine combination can be taken with or without food.
Elderly (age 65 years or over): No adjustment of the recommended dose is generally required for elderly people but increase of the dosage should take place with care.
If up-titration to the maximum dose of 40 mg olmesartan medoxomil daily is required, blood pressure should be closely monitored.
Renal impairment: The maximum dose of Olmesartan medoxomil in patients with mild to moderate renal impairment (creatinine clearance of 20 - 60 mL/min) is 20 mg Olmesartan medoxomil once daily, owing to limited experience of higher dosages in this patient group. The use of Olmesartan medoxomil plus Amlodipine combination in patients with severe renal impairment (creatinine clearance < 20 mL/min) is not recommended.
Monitoring of potassium levels and creatinine is advised in patients with moderate renal impairment.
Hepatic impairment: Olmesartan medoxomil plus Amlodipine combination should be used with caution in patients with mild to moderate hepatic impairment.
In patients with moderate hepatic impairment, an initial dose of 10 mg Olmesartan medoxomil once daily is recommended and the maximum dose should not exceed 20 mg once daily. Close monitoring of blood pressure and renal function is advised in hepatically-impaired patients who are already receiving diuretics and/or other antihypertensive agents. There is no experience of Olmesartan medoxomil in patients with severe hepatic impairment.
As with all calcium antagonists, amlodipine's half-life is prolonged in patients with impaired liver function and dosage recommendations have not been established. Olmesartan medoxomil plus Amlodipine combination should therefore be administered with caution in these patients. The pharmacokinetics of amlodipine have not been studied in severe hepatic impairment.
Amlodipine should be initiated at the lowest dose and titrated slowly in patients with impaired liver function. Use of Olmesartan medoxomil plus Amlodipine combination in patients with severe hepatic impairment is contraindicated.
Paediatric population: The safety and efficacy of Olmesartan medoxomil plus Amlodipine combination in children and adolescents below 18 years has not been established. No data are available.
Method of administration: The tablet should be swallowed with a sufficient amount of fluid (e.g. one glass of water). The tablet should not be chewed and should be taken at the same time each day.
Symptoms: There is no experience of overdose with Olmesartan medoxomil plus Amlodipine combination. The most likely effects of Olmesartan Medoxomil overdosage are hypotension and tachycardia; bradycardia could be encountered if parasympathetic (vagal) stimulation occurred. Amlodipine overdosage can be expected to lead to excessive peripheral vasodilatation with marked hypotension and possibly a reflex tachycardia. Marked and potentially prolonged systemic hypotension up to and including shock with fatal outcome has been reported.
Treatment: If intake is recent, gastric lavage may be considered. In healthy subjects, the administration of activated charcoal immediately or up to 2 hours after ingestion of amlodipine has been shown to reduce substantially the absorption of amlodipine.
Clinically significant hypotension due to an overdose of Olmesartan medoxomil plus Amlodipine combination requires active support of the cardiovascular system, including close monitoring of heart and lung function, elevation of the extremities, and attention to circulating fluid volume and urine output. A vasoconstrictor may be helpful in restoring vascular tone and blood pressure, provided that there is no contraindication to its use. Intravenous calcium gluconate may be beneficial in reversing the effects of calcium channel blockade.
Since amlodipine is highly protein-bound, dialysis is not likely to be of benefit. The dialysability of olmesartan is unknown.
Hypersensitivity to the active substances, to dihydropyridine derivatives or to any of the excipients.
Second and third trimesters of pregnancy.
Severe hepatic insufficiency and biliary obstruction.
The concomitant use of Olmesartan medoxomil plus Amlodipine combination with aliskiren-containing products is contraindicated in patients with diabetes mellitus or renal impairment (GFR < 60 mL/min/1.73 m2).
Due to the component amlodipine, Olmesartan medoxomil plus Amlodipine combination is also contraindicated in patients with: severe hypotension; shock (including cardiogenic shock); obstruction of the outflow tract of the left ventricle (e.g. high grade aortic stenosis); haemodynamically unstable heart failure after acute myocardial infarction.
Patients with hypovolaemia or sodium depletion: Symptomatic hypotension may occur in patients who are volume and/or sodium depleted by vigorous diuretic therapy, dietary salt restriction, diarrhoea or vomiting, especially after the first dose. Correction of this condition prior to administration of Olmesartan medoxomil plus Amlodipine combination or close medical supervision at the start of the treatment is recommended.
Other conditions with stimulation of the renin-angiotensin-aldosterone system: In patients whose vascular tone and renal function depend predominantly on the activity of the renin-angiotensin-aldosterone system (e.g. patients with severe congestive heart failure or underlying renal disease, including renal artery stenosis), treatment with other medicinal products that affect this system, such as angiotensin II receptor antagonists, has been associated with acute hypotension, azotaemia, oliguria or, rarely, acute renal failure.
Renovascular hypertension: There is an increased risk of severe hypotension and renal insufficiency when patients with bilateral renal artery stenosis or stenosis of the artery to a single functioning kidney are treated with medicinal products that affect the renin-angiotensin-aldosterone system.
Renal impairment and kidney transplantation: When Olmesartan medoxomil plus Amlodipine combination is used in patients with impaired renal function, periodic monitoring of serum potassium and creatinine levels is recommended. Use of Olmesartan medoxomil plus Amlodipine combination is not recommended in patients with severe renal impairment (creatinine clearance < 20 mL/min). There is no experience of the administration of Olmesartan medoxomil plus Amlodipine combination in patients with a recent kidney transplant or in patients with end-stage renal impairment (i.e. creatinine clearance < 12 mL/min).
Dual blockade of the renin-angiotensin-aldosterone system (RAAS): There is evidence that the concomitant use of ACE-inhibitors, angiotensin II receptor blockers or aliskiren increases the risk of hypotension, hyperkalaemia and decreased renal function (including acute renal failure). Dual blockade of RAAS through the combined use of ACE-inhibitors, angiotensin II receptor blockers or aliskiren is therefore not recommended.
If dual blockade therapy is considered absolutely necessary, this should only occur under specialist supervision and subject to frequent close monitoring of renal function, electrolytes and blood pressure.
ACE-inhibitors and angiotensin II receptor blockers should not be used concomitantly in patients with diabetic nephropathy.
Hepatic impairment: Exposure to amlodipine and Olmesartan medoxomil is increased in patients with hepatic impairment. Care should be taken when Olmesartan medoxomil plus Amlodipine combination is administered in patients with mild to moderate hepatic impairment. In moderately impaired patients, the dose of Olmesartan medoxomil should not exceed 20 mg. In patients with impaired hepatic function, amlodipine should be initiated at the lower end of the dosing range and caution should be used, both on initial treatment and when increasing the dose. Use of Olmesartan medoxomil plus Amlodipine combination in patients with severe hepatic impairment is contraindicated.
Hyperkalaemia: As with other angiotensin II antagonists and ACE inhibitors, hyperkalaemia may occur during treatment, especially in the presence of renal impairment and/or heart failure. Close monitoring of serum potassium levels in at-risk patients is recommended.
Concomitant use with potassium supplements, potassium-sparing diuretics, salt substitutes containing potassium, or other medicinal products that may increase potassium levels (heparin, etc.) should be undertaken with caution and with frequent monitoring of potassium levels.
Lithium: As with other angiotensin II receptor antagonists, the concomitant use of Olmesartan medoxomil plus Amlodipine combination and lithium is not recommended.
Aortic or mitral valve stenosis; obstructive hypertrophic cardiomyopathy: Due to the amlodipine component of Olmesartan medoxomil plus Amlodipine combination, as with all other vasodilators, special caution is indicated in patients suffering from aortic or mitral valve stenosis, or obstructive hypertrophic cardiomyopathy.
Primary aldosteronism: Patients with primary aldosteronism generally will not respond to antihypertensive medicinal products acting through inhibition of the renin-angiotensin system. Therefore, the use of Olmesartan medoxomil plus Amlodipine combination is not recommended in such patients.
Heart failure: As a consequence of the inhibition of the renin-angiotensin-aldosterone system, changes in renal function may be anticipated in susceptible individuals. In patients with severe heart failure whose renal function may depend on the activity of the renin-angiotensin-aldosterone system, treatment with angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor antagonists has been associated with oliguria and/or progressive azotaemia and (rarely) with acute renal failure and/or death.
Patients with heart failure should be treated with caution. In a long-term, placebo controlled study of amlodipine in patients with severe heart failure (NYHA III and IV), the reported incidence of pulmonary oedema was higher in the amlodipine group than in the placebo group. Calcium channel blockers, including amlodipine, should be used with caution in patients with congestive heart failure, as they may increase the risk of future cardiovascular events and mortality.
Sprue-like enteropathy: In very rare cases severe, chronic diarrhoea with substantial weight loss has been reported in patients taking olmesartan few months to years after drug initiation, possibly caused by a localized delayed hypersensitivity reaction. Intestinal biopsies of patients often demonstrated villous atrophy. If a patient develops these symptoms during treatment with olmesartan, and in the absence of other apparent etiologies, olmesartan treatment should be immediately discontinued and should not be restarted. If diarrhoea does not improve during the week after the discontinuation, further specialist (e.g. a gastro-enterologist) advice should be considered.
Ethnic differences: As with all other angiotensin II antagonists, the blood pressure lowering effect of Olmesartan medoxomil plus Amlodipine combination can be somewhat less in black patients than in non-black patients, possibly because of a higher prevalence of low-renin status in the black hypertensive population.
Other: As with any antihypertensive agent, excessive blood pressure decrease in patients with ischaemic heart disease or ischaemic cerebrovascular disease could result in a myocardial infarction or stroke.
Effects on the Ability to Drive or Operate Machinery: Olmesartan medoxomil plus Amlodipine combination can have minor or moderate influence on the ability to drive and use machines.
Dizziness, headache, nausea or fatigue may occasionally occur in patients taking antihypertensive therapy, which may impair the ability to react. Caution is recommended especially at the start of treatment.
Use in Pregnancy: Angiotensin II antagonists should not be initiated during pregnancy. Unless continued angiotensin II antagonist therapy is considered essential, patients planning pregnancy should be changed to alternative antihypertensive treatments which have an established safety profile for use in pregnancy. When pregnancy is diagnosed, treatment with angiotensin II antagonists should be stopped immediately, and, if appropriate, alternative therapy should be started.
Use in the Elderly: In the elderly, increase of the dosage should take place with care.
Pregnancy: There are no data about the use of Olmesartan medoxomil plus Amlodipine combination in pregnant patients. Animal reproductive toxicity studies with Olmesartan medoxomil plus Amlodipine combination have not been performed.
Olmesartan medoxomil (active ingredient of Olmesartan medoxomil plus Amlodipine combination): The use of angiotensin II antagonists is not recommended during the first trimester of pregnancy. The use of angiotensin II antagonists is contraindicated during the 2nd and 3rd trimesters of pregnancy.
Epidemiological evidence regarding the risk of teratogenicity following exposure to ACE inhibitors during the first trimester of pregnancy has not been conclusive; however a small increase in risk cannot be excluded. Whilst there is no controlled epidemiological data on the risk with angiotensin II antagonists, similar risks may exist for this class of drugs. Unless continued angiotensin II antagonists therapy is considered essential, patients planning pregnancy should be changed to alternative anti-hypertensive treatments which have an established safety profile for use in pregnancy. When pregnancy is diagnosed, treatment with angiotensin II antagonists should be stopped immediately, and, if appropriate, alternative therapy should be started.
Exposure to angiotensin II antagonists therapy during the second and third trimesters is known to induce human fetotoxicity (decreased renal function, oligohydramnios, skull ossification retardation) and neonatal toxicity (renal failure, hypotension and hyperkalemia).
Should exposure to angiotensin II antagonists have occurred from the second trimester on, ultrasound check of renal function and skull is recommended. Infants whose mothers have taken angiotensin II antagonists should be closely observed for hypotension.
Amlodipine (active ingredient of Olmesartan medoxomil plus Amlodipine combination): Data on a limited number of exposed pregnancies do not indicate that amlodipine or other calcium receptor antagonists have a harmful effect on the health of the fetus. However, there may be a risk of prolonged delivery.
As a consequence, Olmesartan medoxomil plus Amlodipine combination is not recommended during the first trimester of pregnancy and is contraindicated during the second and third trimesters of pregnancy.
Breastfeeding: Olmesartan is excreted into the milk of lactating rats. However, it is not known whether olmesartan passes into human milk. It is not known whether amlodipine is excreted in breast milk. Similar calcium channel blockers of the dihydropyridine type are excreted in breast milk.
Because no information is available regarding the use of olmesartan and amlodipine during breast-feeding, Olmesartan medoxomil plus Amlodipine combination is not recommended and alternative treatments with better established safety profiles during breast-feeding are preferable, especially while nursing a newborn or preterm infant.
Olmesartan medoxomil plus Amlodipine combination: The most commonly reported adverse reactions during treatment with Olmesartan medoxomil plus Amlodipine combination are peripheral oedema (11.3%), headache (5.3%) and dizziness (4.5%).
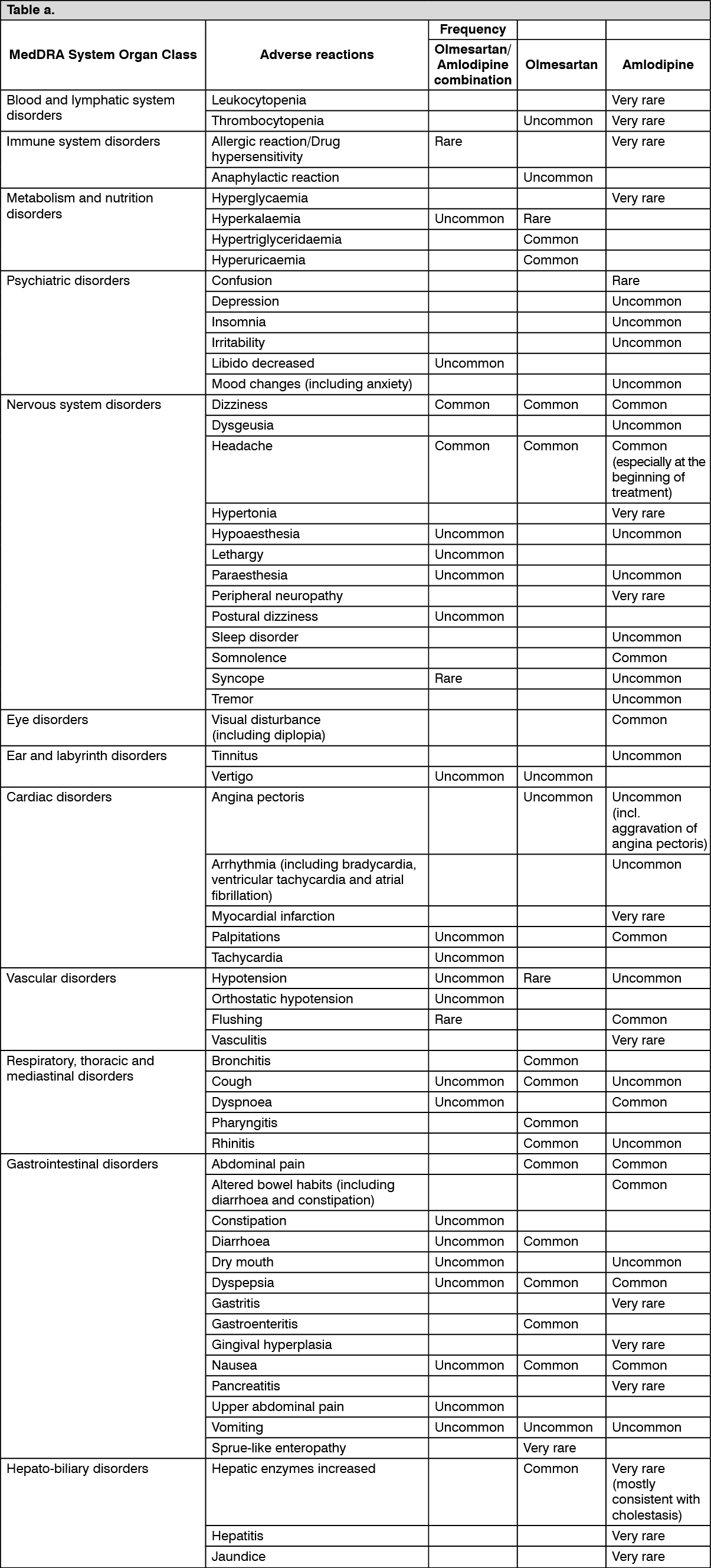
Adverse reactions from Olmesartan medoxomil plus Amlodipine combination in clinical trials, post-authorization safety studies and spontaneous reporting are summarized in the tables as follows as well as adverse reactions from the individual components olmesartan medoxomil and amlodipine based on the known safety profile of these substances.
The following terminologies have been used in order to classify the occurrence of adverse reactions: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1/1,000), Very rare (<1/10,000), not known (cannot be estimated from the available data). (See Tables a and b.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Single cases of rhabdomyolysis have been reported in temporal association with the intake of angiotensin II receptor blockers. Single cases of extrapyramidal syndrome have been reported in patients treated with amlodipine.
Potential interactions related to the Olmesartan medoxomil plus Amlodipine combination: To be taken into account with concomitant use.
Other antihypertensive agents: The blood pressure lowering effect of Olmesartan medoxomil plus Amlodipine combination can be increased by concomitant use of other antihypertensive medicinal products (e.g. alpha blockers, diuretics).
Potential interactions related to the Olmesartan medoxomil component of Olmesartan medoxomil plus Amlodipine combination: Concomitant use not recommended.
ACE-inhibitors, angiotensin II receptor blockers or aliskiren: Clinical trial data has shown that dual blockade of the renin-angiotensin-aldosterone-system (RAAS) through the combined use of ACE-inhibitors, angiotensin II receptor blockers or aliskiren is associated with a higher frequency of adverse events such as hypotension, hyperkalaemia and decreased renal function (including acute renal failure) compared to the use of a single RAAS-acting agent.
Medicinal products affecting potassium levels: Concomitant use of potassium-sparing diuretics, potassium supplements, salt substitutes containing potassium or other medicinal products that may increase serum potassium levels (e.g. heparin, ACE inhibitors) may lead to increases in serum potassium. If medicinal products which affect potassium levels are to be prescribed in combination with Olmesartan medoxomil plus Amlodipine combination, monitoring of serum potassium levels is recommended.
Lithium: Reversible increases in serum lithium concentrations and toxicity have been reported during concomitant administration of lithium with angiotensin converting enzyme inhibitors and, rarely, with angiotensin II antagonists. Therefore concomitant use of Olmesartan medoxomil plus Amlodipine combination and lithium is not recommended. If concomitant use of Olmesartan medoxomil plus Amlodipine combination and lithium proves necessary, careful monitoring of serum lithium levels is recommended.
Concomitant use requiring caution: Non-steroidal anti-inflammatory medicinal products (NSAIDs) including selective COX-2 inhibitors, acetylsalicylic acid (> 3 g/day) and non-selective NSAIDs: When angiotensin II antagonists are administered simultaneously with NSAIDs, attenuation of the antihypertensive effect may occur. Furthermore, concomitant use of angiotensin II antagonists and NSAIDs may increase the risk of worsening of renal function and may lead to an increase in serum potassium. Therefore monitoring of renal function at the beginning of such concomitant therapy is recommended, as well as adequate hydration of the patient.
Bile acid sequestering agent colesevelam: Concurrent administration of the bile acid sequestering agent colesevelam hydrochloride reduces the systemic exposure and peak plasma concentration of olmesartan and reduces t½. Administration of olmesartan medoxomil at least 4 hours prior to colesevelam hydrochloride decreased the drug interaction effect. Administering olmesartan medoxomil at least 4 hours before the colesevelam hydrochloride dose should be considered.
Additional information: After treatment with antacid (aluminium magnesium hydroxide), a modest reduction in bioavailability of olmesartan was observed.
Olmesartan medoxomil had no significant effect on the pharmacokinetics or pharmacodynamics of warfarin or the pharmacokinetics of digoxin. Co-administration of Olmesartan medoxomil with pravastatin had no clinically relevant effects on the pharmacokinetics of either component in healthy subjects.
Olmesartan had no clinically relevant inhibitory effects on human cytochrome P450 enzymes 1A1/2, 2A6, 2C8/9, 2C19, 2D6, 2E1 and 3A4 in vitro, and had no or minimal inducing effects on rat cytochrome P450 activities. No clinically relevant interactions between olmesartan and medicinal products metabolized by the previously mentioned cytochrome P450 enzymes are expected.
Potential interactions related to the amlodipine component of Olmesartan medoxomil plus Amlodipine combination: Effects of other medicinal products on amlodipine: CYP3A4 inhibitors: Concomitant use of amlodipine with strong or moderate CYP3A4 inhibitors (protease inhibitors, azole antifungals, macrolides like erythromycin or clarithromycin, verapamil or diltiazem) may give rise to significant increase in amlodipine exposure. The clinical translation of these PK variations may be more pronounced in the elderly. Clinical monitoring and dose adjustment may thus be required.
CYP3A4 inducers: There is no data available regarding the effect of CYP3A4 inducers on amlodipine. The concomitant use of CYP3A4 inducers (i.e. rifampicin, Hypericum perforatum) may give a lower plasma concentration of amlodipine. Amlodipine should be used with caution together with CYP3A4 inducers.
Administration of amlodipine with grapefruit or grapefruit juice is not recommended as bioavailability may be increased in some patients resulting in increased blood pressure lowering effects.
Dantrolene (infusion): In animals, lethal ventricular fibrillation and cardiovascular collapse are observed in association with hyperkalaemia after administration of verapamil and intravenous dantrolene. Due to risk of hyperkalaemia, it is recommended that the co-administration of calcium channel blockers such as amlodipine be avoided in patients susceptible to malignant hyperthermia and in the management of malignant hyperthermia.
Effects of amlodipine on other medicinal products: The blood pressure lowering effects of amlodipine adds to the blood pressure-lowering effects of other antihypertensive agents.
In clinical interaction studies, amlodipine did not affect the pharmacokinetics of atorvastatin, digoxin or warfarin.
Simvastatin: Co-administration of multiple doses of 10 mg of amlodipine with 80 mg simvastatin resulted in a 77% increase in exposure to simvastatin compared to simvastatin alone. Limit the dose of simvastatin in patients on amlodipine to 20 mg daily.
Tacrolimus: There is a risk of increased tacrolimus blood levels when co-administered with amlodipine but the pharmacokinetic mechanism of this interaction is not fully understood. In order to avoid toxicity of tacrolimus, administration of amlodipine in a patient treated with tacrolimus requires monitoring of tacrolimus blood levels and dose adjustment of tacrolimus when appropriate.
Cyclosporine: In a prospective study in renal transplant patients, an average 40% increase in trough cyclosporine levels was observed when used concomitantly with amlodipine. The co-administration of Olmesartan medoxomil plus Amlodipine combination with cyclosporine may increase exposure to cyclosporine. Monitor trough cyclosporine levels during concomitant use and cyclosporine dose reductions should be made as necessary.
Store at temperatures not exceeding 30°C.
C09DB02 - olmesartan medoxomil and amlodipine ; Belongs to the class of angiotensin II receptor blockers (ARBs) and calcium channel blockers. Used in the treatment of cardiovascular disease.
Alzor CCB 20 mg/10 mg FC tab
30's
Alzor CCB 20 mg/5 mg FC tab
30's
Alzor CCB 40 mg/10 mg FC tab
30's
Alzor CCB 40 mg/5 mg FC tab
30's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image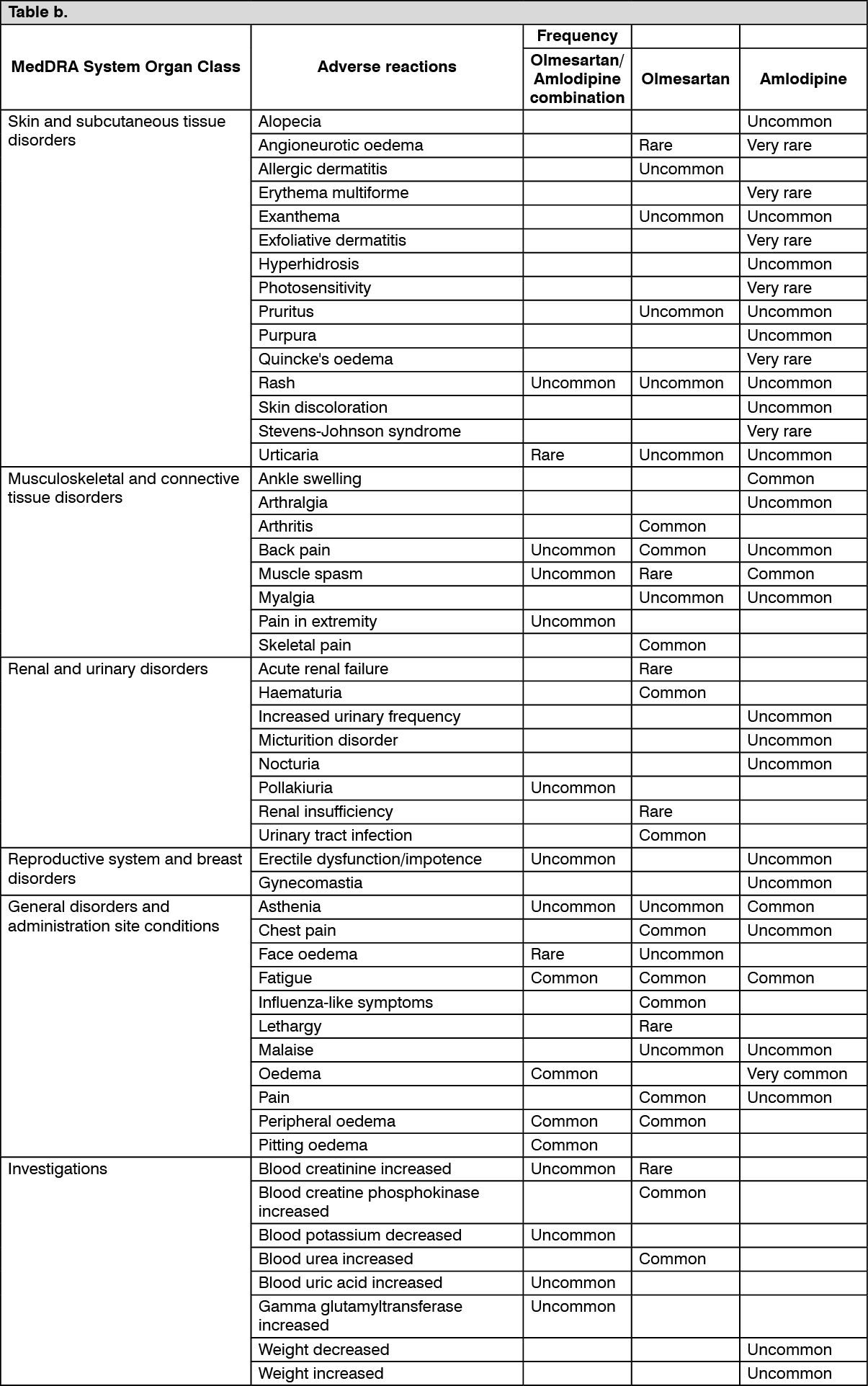 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out