Pharmacotherapeutic group: Drugs for dementia.
ATC Code: N06DA02.
Pharmacology: Pharmacodynamics: Donepezil hydrochloride is a specific and reversible inhibitor of acetylcholinesterase, the predominant cholinesterase in the brain. Donepezil hydrochloride is over 1000 times more potent inhibitor of this enzyme than of butyrylcholinesterase, an enzyme which is present mainly outside the central nervous system.
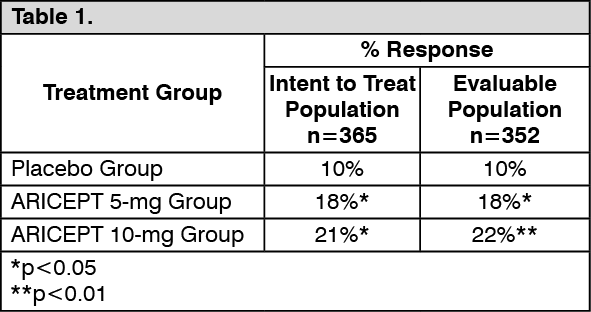
Mild to moderately severe Alzheimer's disease: In patients with Alzheimer's dementia participating in clinical trials, administration of single daily doses of 5 mg or 10 mg of Donepezil hydrochloride produced steady-state inhibition of acetylcholinesterase activity (measured in erythrocyte membranes) of 63.6% and 77.3%, respectively when measured post-dose. The inhibition of acetylcholinesterase (AChE) in red blood cells by donepezil hydrochloride has been shown to correlate to changes in ADAS-Cog, a sensitive scale which examines selected aspects of cognition. The potential for donepezil hydrochloride to alter the course of the underlying neuropathology has not been studied. In the clinical trials of patients with mild to moderately severe Alzheimer's Disease, an analysis was done at the conclusion of 6 months of donepezil hydrochloride treatment using a combination of three efficacy criteria: the ADAS-Cog, the Clinician Interview Based Impression of Change with Caregiver Input (CIBIC-Plus - a measure of global function) and the Combined Activities of Daily Living Domains of the Clinical Dementia Rating Scale) CDR - a measure of capabilities in community affairs, home and hobbies and personal care).
Patients who fulfilled the criteria listed as follows were considered treatment responders.
Response: Improvement of ADAS-Cog of at least 4 points; No deterioration of CIBIC - Plus scores; No deterioration of Combined Activities of Daily Livinq Domains of the Clinical Dementia Rating Scale (CDR). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Donepezil hydrochloride (ARICEPT EVESS) produced a dose-dependent statistically significant increase in the percentage of patients who were judged treatment responders (Figure 1). The percentages of randomized patients who completed the study were: Placebo 80%, 5 mg/day 85% and 10 mg/day 68%. (See Figure 1.)
Click on icon to see table/diagram/image
The curves demonstrate that both patients assigned to placebo and donepezil hydrochloride have a wide range of responses, but that the active treatment groups are more likely to show greater improvements. A curve for an effective treatment would be shifted to the left of the curve for placebo, while an ineffective or deleterious treatment would be superimposed upon or shifted to the right of the curve for placebo, respectively.
Figure 2 is a histogram of the frequency distribution of CIBIC-Plus scores attained by patients assigned to each of the three treatment groups who completed 24 weeks of treatment. The mean drug-placebo differences for these groups of patients were 0.35 units and 0.39 units for 5 mg/day and 10 mg/day of donepezil hydrochloride, respectively. The differences were statistically significant. There was no statistically significant difference between the two active treatments. (See Figure 2.)
Click on icon to see table/diagram/image
Severe Alzheimer's disease: Swedish 6 month Study: The effectiveness of donepezil hydrochloride as a treatment for severe Alzheimer's disease is demonstrated by the results of a randomized, double-blind, placebo-controlled clinical study conducted in Sweden (6 month Study) in patients with probable or possible Alzheimer's disease diagnosed by NINCDS-ADRDA and DSM-IV criteria, MMSE: range of 1-10. Two hundred and forty-eight (248) patients with severe Alzheimer's disease were randomized to donepezil hydrochloride or placebo. For patients randomized to donepezil hydrochloride, treatment was initiated at 5 mg once daily for 28 days and then increased to 10 mg once daily. At the end of 6 month treatment period, 90.5% of the donepezil hydrochloride-treated patients were receiving the 10 mg dose. The mean age of patients was 84.9 years with a range of 59 to 99. Approximately 77% of patients were women and 23% were men. Almost all patients were Caucasian. Probable AD was diagnosed in the majority of the patients (83.6% of donepezil hydrochloride-treated patients and 84.2% of placebo-treated patients).
Study Outcome Measures: The effectiveness of treatment with donepezil hydrochloride was determined using a dual outcome assessment strategy that evaluated cognitive function using an instrument designed for more impaired patients and overall function through caregiver-rated assessment. This study showed that patients on donepezil hydrochloride experienced significant improvement on both measures compared to placebo.
The ability of donepezil hydrochloride to improve cognitive performance was assessed with the Severe Impairment Battery (SIB). The SIB, a multi-item instrument, has been validated for the evaluation of cognitive function in patients with moderately severe to severe dementia. The SIB evaluates selective aspects of cognitive performance, including elements of memory, language, orientation, attention, praxis, visuospatial ability, construction, and social interaction. The SIB scoring range is from 0 to 100, with lower scores indicating greater cognitive impairment. Daily function was assessed using the Modified Alzheimer's disease Cooperative Study Activities of Daily Living Inventory for Severe Alzheimer's disease (ADCS-ADL-severe). The ADCS-ADL-severe is derived from the Alzheimer's disease Cooperative Study Activities of Daily Living Inventory, which is a comprehensive battery of ADL questions used to measure the functional capabilities of patients. Each ADL item is rated from the highest level of independent performance to complete loss. The ADCS-ADL-severe is a subset of 19 items, including ratings of the patient's ability to eat, dress, bathe, use the telephone, get around (or travel), and perform other activities of daily living; it has been validated for the assessment of patients with moderately severe to severe dementia. The ADCS-ADL-severe has a scoring range of 0 to 54 with the lower scores indicating greater functional impairment. The investigator performs the inventory by interviewing a caregiver, in this study a nurse staff member, familiar with the functioning of the patient.
Effects on the SIB: Figure 3 shows the time course for the change from baseline in SIB score tor the two treatment groups over the 6 months of the study. At 6 months of treatment, the mean difference in the SIB change scores for donepezil hydrochloride-treated patients compared to patients on placebo was 5.9 units. Donepezil hydrochloride treatment was statistically significantly superior to placebo. (See Figure 3.)
Click on icon to see table/diagram/image
Figure 4 illustrates the cumulative percentages of patients from each of the two treatment groups who attained the measure of improvement in SIB score shown on the X-axis. While patients assigned both to donepezil hydrochloride and to placebo have a wide range of responses, the curves show that the donepezil hydrochloride group is more likely to show a greater improvement in cognitive performance. (See Figure 4.)
Click on icon to see table/diagram/image
Effects on the ADCS-ADL-severe: Figure 5 illustrates the time course for the change from baseline in ADCS-ADL-severe scores for patients in the two treatment groups over the 6 months of the study. After 6 months of treatment, the mean difference in the ADCS-ADL-severe change scores for donepezil hydrochloride treated patients compared to patients on placebo was 1.8 units. ARICEPT treatment was statistically significantly superior to placebo. (See Figure 5.)
Click on icon to see table/diagram/image
Figure 6 shows the cumulative percentages of patients from each treatment group with specified changes from baseline ADCS-ADL-severe scores. While both patients assigned to donepezil hydrochloride and placebo have a wide range of responses, the curves demonstrate that the donepezil hydrochloride group is more likely to show a smaller decline or an improvement. (See Figure 6.)
Click on icon to see table/diagram/image
Japanese 24-Week Study: In a study of 24 weeks duration, conducted in Japan, 325 patients with severe Alzheimer's disease were randomized to doses of 5 mg/day or 10 mg/day of donepezil hydrochloride, administered once daily, or placebo. Patients randomized to treatment with donepezil hydrochloride were to achieve their assigned doses by titration, beginning at 3 mg/day, and extending over a maximum of 6 weeks. 248 patients completed the study with similar proportions of patients completing the study in each treatment group. The primary efficacy measures for this study were the SIB and CIBIC plus.
At 24 weeks of treatment, statistically significant treatment differences were observed between the 10 mg/day dose of donepezil hydrochloride and placebo on both the SIB and CIBIC plus. The 5 mg/day dose of donepezil hydrochloride showed a statistically significant superiority to placebo on the SIB, but not on the CIBIC plus.
Multinational Study in Patients with Severe AD: A multinational, multicenter, randomized, double-blind, placebo-controlled, parallel-group, 24 week study in patients with severe Alzheimer's disease was also conducted. A total of 343 subjects were randomized, 176 to donepezil hydrochloride and 167 to placebo. Subjects received 5 mg daily of donepezil hydrochloride (immediate release) for the first 6 weeks, followed by 10 mg daily of donepezil hydrochloride for the remainder of the double-blind phase of the study.
Donepezil hydrochloride was statistically significantly superior to placebo on the SIB score at endpoint for both the ITT LOCF population (LS mean difference of 5.32 points; p=0.0001). On the CIBIC-plus patients, the difference favored donepezil hydrochloride treatment but did not reach statistical significance (p=0.0905). However, after collapsing the 7-point scale to a 3-point scale (improved, no change or worsened), statistically significant differences favoring the donepezil hydrochloride group were found compared to the placebo group for both the ITT LOCF population (p=0.0156).
Vascular dementia: The efficacy of treatment of vascular dementia with Donepezil hydrochloride (ARICEPT EVESS) has been investigated in three placebo-controlled trials of 6-month duration in which the diagnostic criteria for vascular dementia proposed by the NINDS-AIREN consensus group (National Institute of Neurological Disorders and Stroke Association Internationale pour la Recherche et l'Enseignementen Neuroscience) were used to define the population of patients studied.
In the first two studies, an analysis was done at the conclusion of donepezil hydrochloride treatment using a combination of three efficacy criteria. Patients from the first two studies who fulfilled the criteria listed as follows were considered treatment responders. Response was defined as (1) improvement of ADAS-Cog of at least 4 points; and (2) improvement or no deterioration of CIBIC-Plus; and (3) improvement or no deterioration of Clinical Dementia Rating functionality subscale (Table 2). Donepezil hydrochloride produced a statistically significant increase in the percentage of patients who were Judged treatment responders. (See Table 2.)
Click on icon to see table/diagram/image
In the third study, the primary efficacy measures were the Vascular-Alzheimer's disease Assessment Scale-Cognitive Subscale (V-ADAS-Cog) and the Clinician's Interview-Based Impression of Change-Plus (CIBIC-Plus). The endpoint analyses of the primary efficacy measures were done using the intent to treat (ITT) population with the last observation carried forward (LOCF). There was a statistically significant treatment difference favoring donepezil hydrochloride in the change from Baseline to Endpoint in the V-ADAS-Cog (p=0.0067). However, for the CIBIC-Plus at Endpoint, statistical significance was not demonstrated for the treatment difference by a Cochran-Mantel-Haenszel (CMH) analysis of the frequency distribution of responses (p=0.2287). A sensitivity analysis of CIBIC-Plus using ANCOVA analysis of the overall change treated as a numerical value also did not show statistical significance (P=0.3431).
Dementia with Lewy Bodies: The effectiveness of donepezil hydrochloride as a treatment for Dementia with Lewy Bodies (DLB) was investigated in two multicenter, randomized, double-blind, parallel-group, placebo-controlled, 12-week studies in Japanese patients diagnosed with probable DLB according to the consensus diagnostic criteria of the 1st Consortium on DLB International Workshop, MMSE: range 10-26.
Japanese Exploratory 12-Week Study: A total of 140 subjects were randomized, 35 to donepezil hydrochloride 3 mg/day, 33 to donepezil hydrochloride 5 mg/day, 37 to donepezil hydrochloride 10 mg/day and 35 to placebo. In the 5 mg group, the initial dose was 3 mg. After 2 weeks, the dose was increased to 5 mg. In the 10 mg group, the initial dose 3 mg. After 2 weeks, the dose was increased to 5 mg. The dose was further increased to 10 mg after dosing at 5 mg for 4 weeks.
Study Outcome Measures: Since this study was an exploratory study, no specific primary endpoint was set and multiplicity test was not taken into consideration.
The ability of donepezil hydrochloride to produce an overall clinical effect was assessed using a Clinician's Interview-Based Impression of Change that incorporated the use of caregiver information, the CIBIC-plus.
The ability of donepezil hydrochloride to improve cognitive function was assessed using a Mini-Mental State Examination (MMSE). The MMSE is a widely used, brief and reliable test for evaluating the cognitive function of patients with neurocognitive disorder.
Behavioral and neuropsychiatric symptoms were assessed using a Neuropsychiatric Inventory (NPI; modified NPl-12). This consisted of 12 items: the original 10 items (delusions, hallucinations, dysphoria, anxiety, agitation/aggression, euphoria, disinhibition, irritability/lability, apathy, and aberrant motor activity; NPl-10), sleep, and cognitive fluctuation, which was reported as Cognitive Fluctuation Inventory. An NPl-2 is a 2-item subscore calculated as the sum of scores for hallucinations and cognitive fluctuation, which correspond to two of the core features of DLB.
Effects on the CIBIC-Plus: The improvement in CIBIC plus at the final evaluation (LOCF) was distributed to the improving direction (Table 3), showing a significant difference from placebo group in all donepezil groups (p<0.001 in the 3 mg group, p=0.001 in the 5 mg group, p=0.001 in the 1 0 mg group; 2-sample Wilcoxon test). (See Table 3.)
Click on icon to see table/diagram/image
Effects on the MMSE: The mean differences of MMSE score between donepezil groups and placebo group for the change from Baseline to Week 12 (LOCF) were: 3 mg 1.8 units, 5 mg 4.1 units and 10 mg 2.8 units (Table 4), indicating statistically significant treatment benefits in favor of all donepezil groups over the placebo group (p=0.046 in the 3 mg group, p<0.001 in the 5 mg group, p<0.001 in the 10 mg group; 2-sample
t test). (See Table 4.)
Click on icon to see table/diagram/image
Effects on the NPI-2: The mean differences of NPI-2 score between the donepezil groups and placebo group for the change from Baseline to Week 12 (LOCF) were: 3 mg -2.4 units, 5 mg -3.6 units and 10 mg -5.2 units (Table 5), indicating statistically significant treatment benefits in favor of 5 mg and 10 mg groups over placebo group (p=0.001 in the 5 mg group, p<0.001 in the 10 mg group; 2-sample
t test). (See Table 5.)
Click on icon to see table/diagram/image
Japanese Confirmatory 12-Week Study: A total of 142 subjects were randomized, 47 to donepezil hydrochloride 5 mg/day, 49 to donepezil hydrochloride 10 mg/day and 46 to placebo. In the 5 mg group, the initial dose was 3 mg. After 2 weeks, the dose was increased to 5 mg. In the 10 mg group, the initial dose 3 mg. After 2 weeks, the dose was increased to 5 mg. The dose was further increased 10 mg after dosing at 5 mg for 4 weeks.
Study Outcome Measures: The effectiveness of treatment with donepezil hydrochloride was determined using a dual outcome assessment strategy that evaluated cognitive function measured by the MMSE and psychiatric symptom and behavioral disorders measured by the NPI-2. The co-primary efficacy variables, using the LOCF imputation for missing data, were used to determine whether each treatment with donepezil 5 mg and donepezil 10 mg has superior efficacy compared to placebo.
The statistical significance both in MMSE and NPI-2 between the placebo group and each donepezil group could determine a superiority of the donepezil over placebo. However, no superiority was demonstrated in either the 5 mg or 10 mg group in the primary analysis.
Effects on the MMSE: The mean differences of MMSE score between each donepezil group and the placebo group for the change from Baseline to Week 12 were: 5 mg 0.8 units and 10 mg 1.6 units (Table 6), indicating a statistically significant treatment benefit in favor of the donepezil 10 mg group over the placebo group (p=0.016; ANCOVA). (See Table 6.)
Click on icon to see table/diagram/image
Effects on the NPI-2: For the mean differences of NPl-2 score at Week 12 (Table 7), there was no significant difference between each treatment of donepezil and placebo. (See Table 7.)
Click on icon to see table/diagram/image
Post Marketing Surveillance etc.: Post-marketing clinical study in Japan in patients with dementia with Lewy bodies: A post-marketing clinical study was conducted in patients with dementia with Lewy bodies (MMSE score ≥10 and ≤26). During the treatment period (double-blind, placebo-controlled), the patients received this drug at 10 mg (at 3 mg/day for 2 weeks, and then at 5 mg/day for 4 weeks, followed by 10 mg/day or 5 mg/day when the dose was reduced for 6 weeks) or placebo for 12 weeks. Patients who completed the treatment period received 10 mg of this drug in the extension treatment period of 48 weeks (open-label, uncontrolled) (10 mg/day or 5 mg/day during dose reduction in the treatment period drug group, and 3 mg/day for 2 weeks, 5 mg/day for 4 weeks, and 10 mg/day or 5 mg/day during dose reduction in the treatment period placebo group).
In the treatment period, 160 patients received either this drug or placebo, with no significant difference between the placebo and this drug groups in the distribution of clinical global impressions (CIBIC-plus overall assessment) at the final evaluation during the treatment period, the primary endpoint (p=0.408, two-sample Wilcoxon test; the significance level at the final analysis [two-sided] was 0.046). (See Table 8.)
Click on icon to see table/diagram/image
The distribution of clinical global impressions (CIBIC-plus overall assessment) at the final evaluation during the treatment period by the presence or absence of visual hallucinations before the treatment initiation was as follows. (See Table 9.)
Click on icon to see table/diagram/image
Rating Scale: 1: Markedly improved, 2: Improved, 3: Slightly improved, 4: No change, 5: Slightly aggravated, 6: Aggravated, 7: Markedly aggravated.
The treatment period was completed by 143 patients of whom 139 entered the extension treatment period and 105 completed the extension treatment period. The change from baseline MMSE at each evaluation time point (treatment and extension treatment periods), the secondary endpoints, is shown in the figure as follows. (See Figure 7.)
Click on icon to see table/diagram/image
The placebo group started receiving 3 mg/day of this drug at Week 12, 5 mg/day at Week 14, and 10 mg/day at Week 18 (the dose could be reduced to 5 mg/day). Mixed Model for Repeated Measures with the treatment group, time point, and interaction between treatment group and time point as factors, and change in MMSE baseline values and screening period as covariates. The covariance structure was assumed to be unstructured.
Changes in MMSE from baseline at each evaluation time point (treatment and extension treatment periods): The study did not test the hypothesis stating that the efficacy of the drug on clinical global impressions is superior to that of a placebo.
Pharmacokinetics: Absorption: Maximum plasma levels are reached approximately 3 to 4 hours after oral administration. Plasma concentrations and area under the curve rise in proportion to the dose. The terminal disposition half-life is approximately 70 hours, thus, administration of multiple single-daily doses results in gradual approach to steady-state. Approximate steady-state is achieved within 3 weeks after initiation of therapy. Once at steady-state, plasma donepezil hydrochloride concentrations and the related pharmacodynamic activity show little variability over the course of the day.
Food does not affect the absorption of donepezil hydrochloride.
Distribution: Donepezil hydrochloride is approximately 95% bound to human plasma proteins. The plasma protein binding of the active metabolite 6-O-desmethyldonepezil is not known. The distribution of donepezil hydrochloride in various body tissues has not been definitively studied. However, in a mass balance study conducted in healthy male volunteers, 240 hours after the administration of a single 5 mg dose of
14C-labeled donepezil hydrochloride, approximately 28% of the label remained unrecovered. This suggests that donepezil hydrochloride and/or its metabolites may persist in the body for more than 10 days.
Metabolism/Excretion: Donepezil is hepatically metabolized and the predominant route for the elimination of both parent drug and its metabolites is renal, as 79% of the recovered dose was found in the urine with the remaining 21% found in the feces. Moreover, the parent compound, donepezil, is the predominant elimination product in urine. The major metabolites of donepezil include M1 and M2 (via
O-dealkylation and hydroxylation), M11 and M12 (via glucuronidation of M1 and M2, respectively), M4 (via hydrolysis) and M6 (via
N-oxidation).
Plasma donepezil concentrations decline with a half-life of approximately 70 hours.
Sex, race and smoking history have no clinically significant influence on plasma concentrations of donepezil hydrochloride. The pharmacokinetics of donepezil has not been formally studied in healthy elderly subjects, or in Alzheimer's or vascular dementia patients. However, mean plasma levels in patients closely agreed with those of young healthy volunteers.
There was a relationship noted between body weight and clearance. Over the range of body weight from 50 kg to 110 kg, clearance increased from 7.77 L/h to 14.04 L/h, with a value of 10 L/h for 70 kg individuals.
Toxicology: Pre-clinical Safety Data: General: Extensive testing in experimental animals has demonstrated that this compound causes few effects other than the intended pharmacological effects consistent with its action as a cholinesterase inhibitor.
Mutagenicity: Donepezil hydrochloride is not genotoxic in bacterial reverse mutation and mouse lymphoma
tk assays. In chromosomal aberration assays
in vitro, some clastogenic effects were observed
in vitro at concentrations overtly toxic to the cells and more than 3000 times the steady-state plasma concentrations produces by 10 mg/day. However, no clastogenic potential was observed in the
in vivo mouse micronucleus model and DNA damage was not observed
in vivo/
in vitro UDS assay. In summary, donepezil was negative in a battery of genotoxicity assays (
in vitro bacterial reverse mutation,
in vitro mouse lymphoma
tk,
in vitro chromosomal aberration, and
in vivo mouse micronucleus).
Carcinogenicity: No evidence of a carcinogenic potential was obtained in an 88 week carcinogenicity study of donepezil hydrochloride conduced in CD-1 mice at doses of up to 180 mg/kg/day (approximately 39 times the maximum recommended human dose (23 mg/day) on a mg/m
2 basis), or in a 104 week carcinogenicity study in Sprague-Dawley rats at doses of up to 30 mg/kg/day (approximately 13 times the maximum recommended human dose on a mg/m
2 basis.
Fertility: Donepezil hydrochloride had no effect on fertility at dosages up to 10 mg/kg/day (approximately 4 times the maximum recommended human dose [23 mg/day] on a mg/m
2 basis) when administered to males and females prior to and during mating and continuing in females through implantation. Donepezil hydrochloride was not teratogenic in rats or rabbits. Donepezil hydrochloride had a slight effect on stillbirths and early pup survival when administered to pregnant rats at doses up to 10 mg/kg/day (see Use in Pregnancy & Lactation).


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image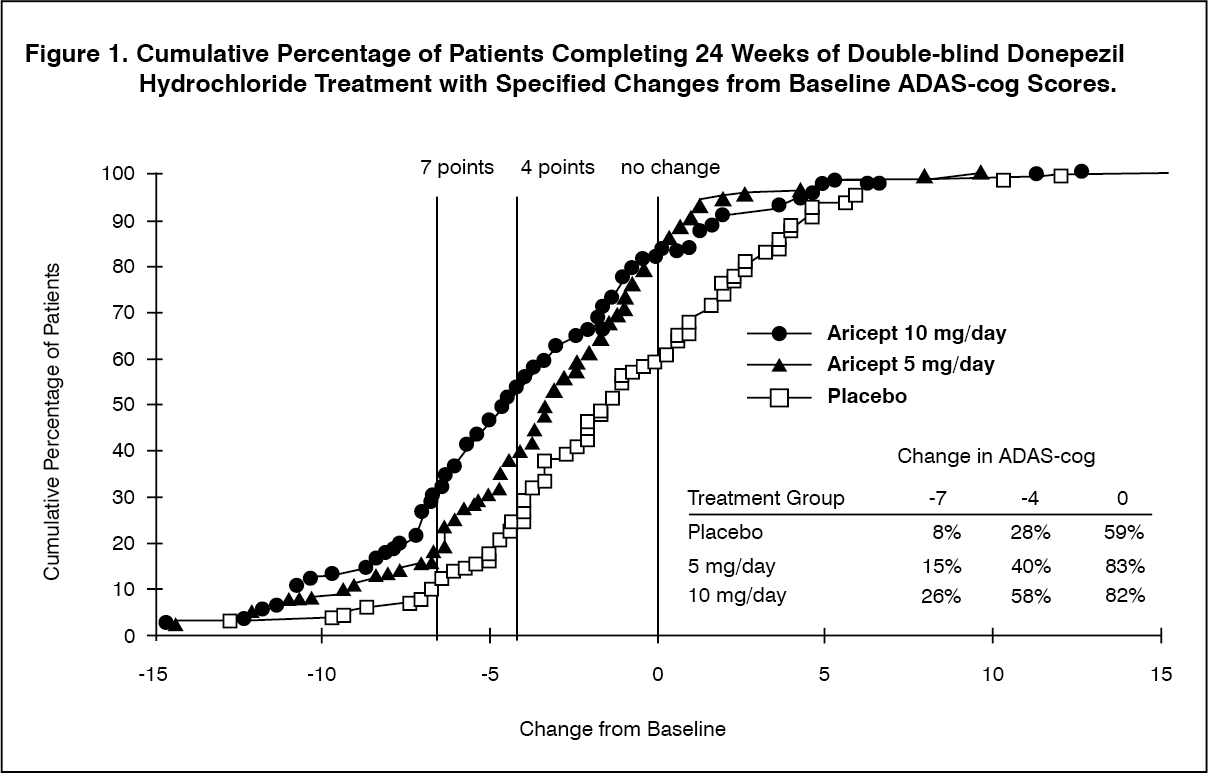 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image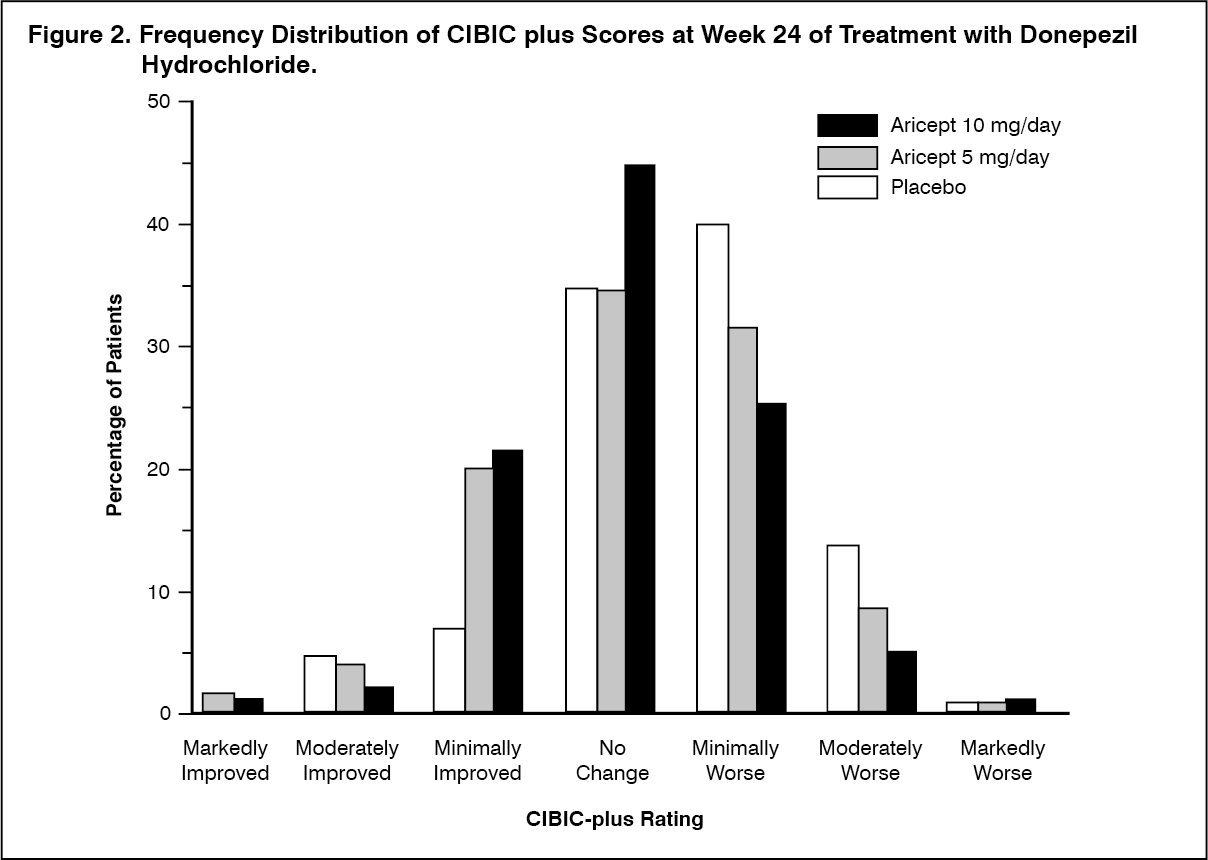 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image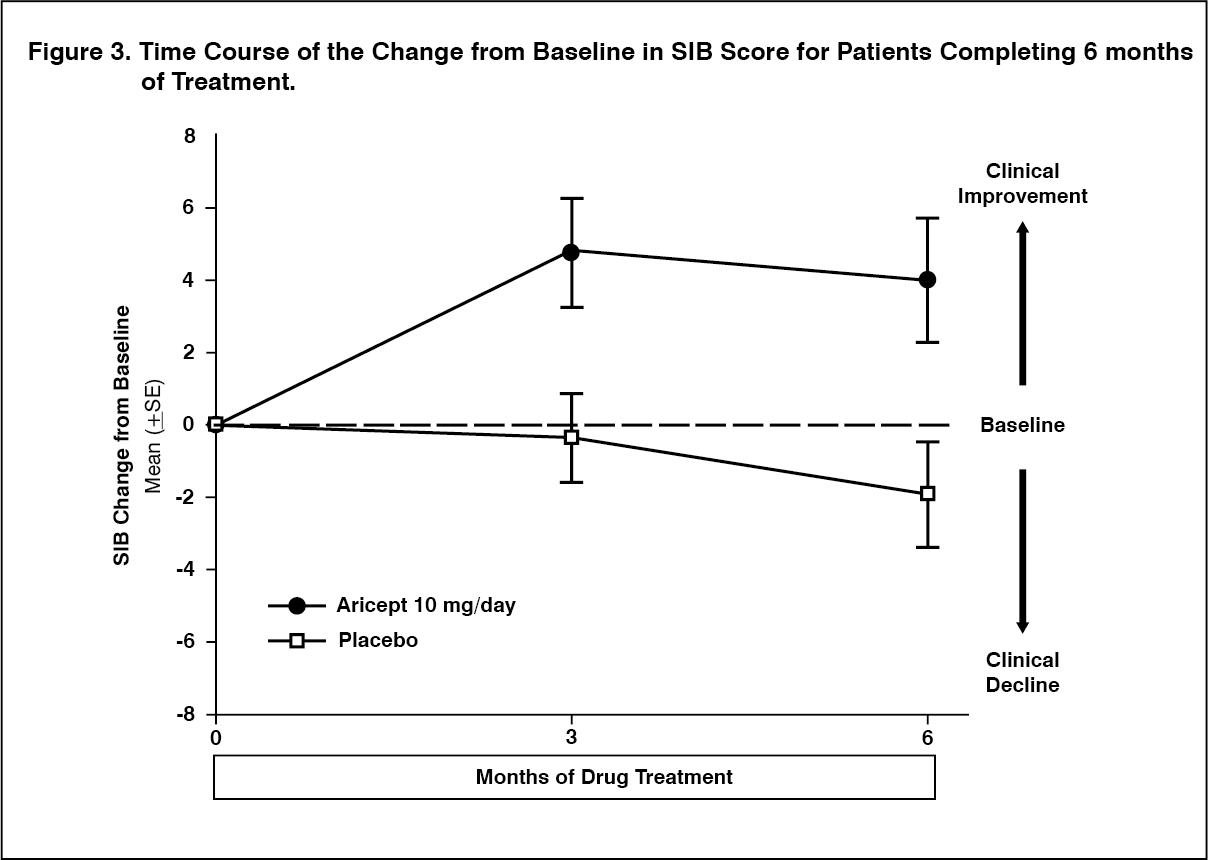 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image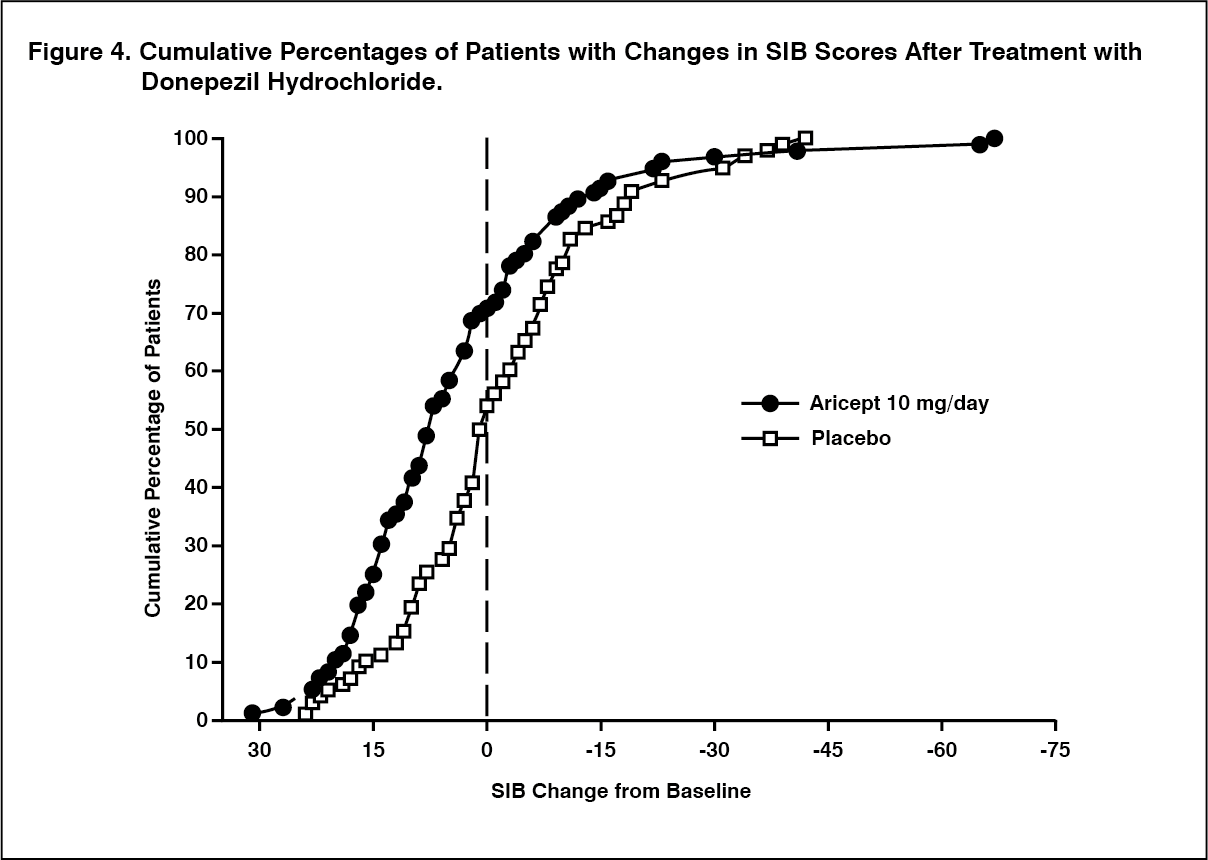 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image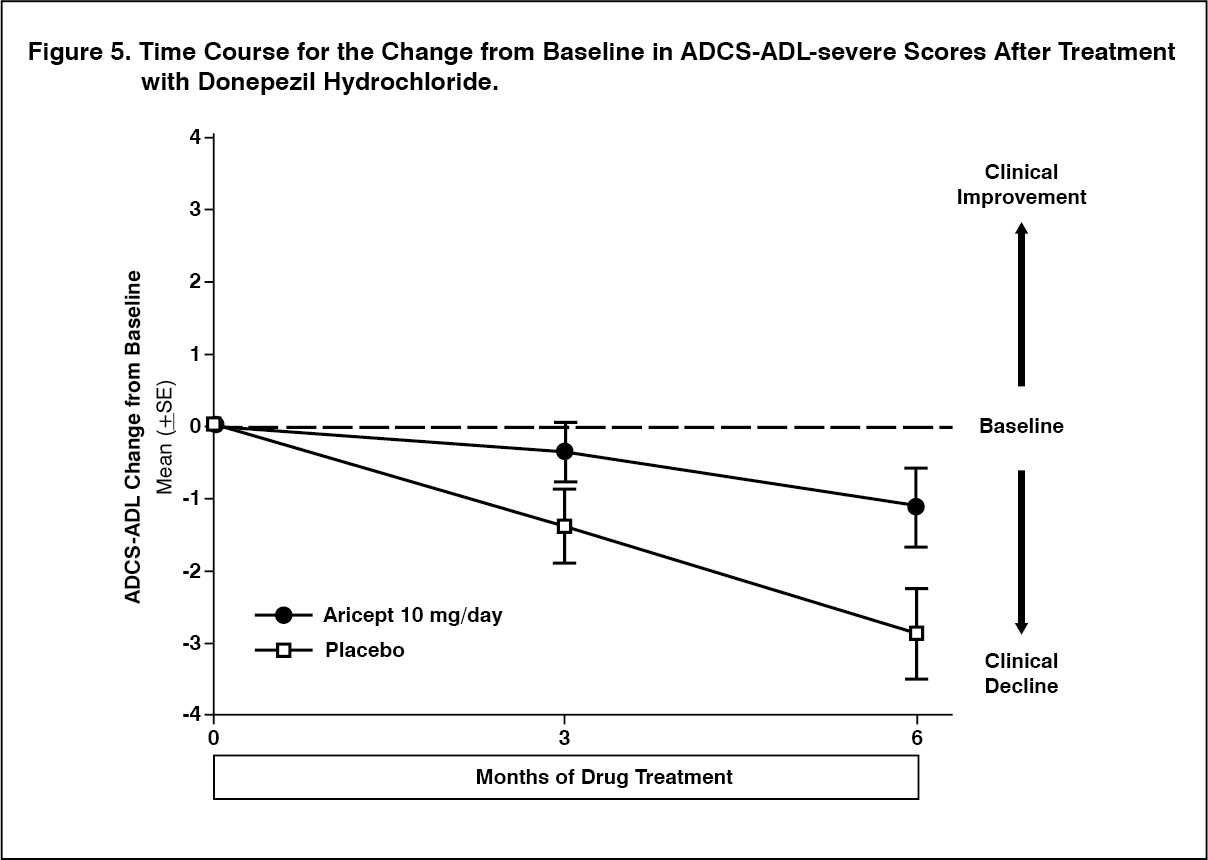 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image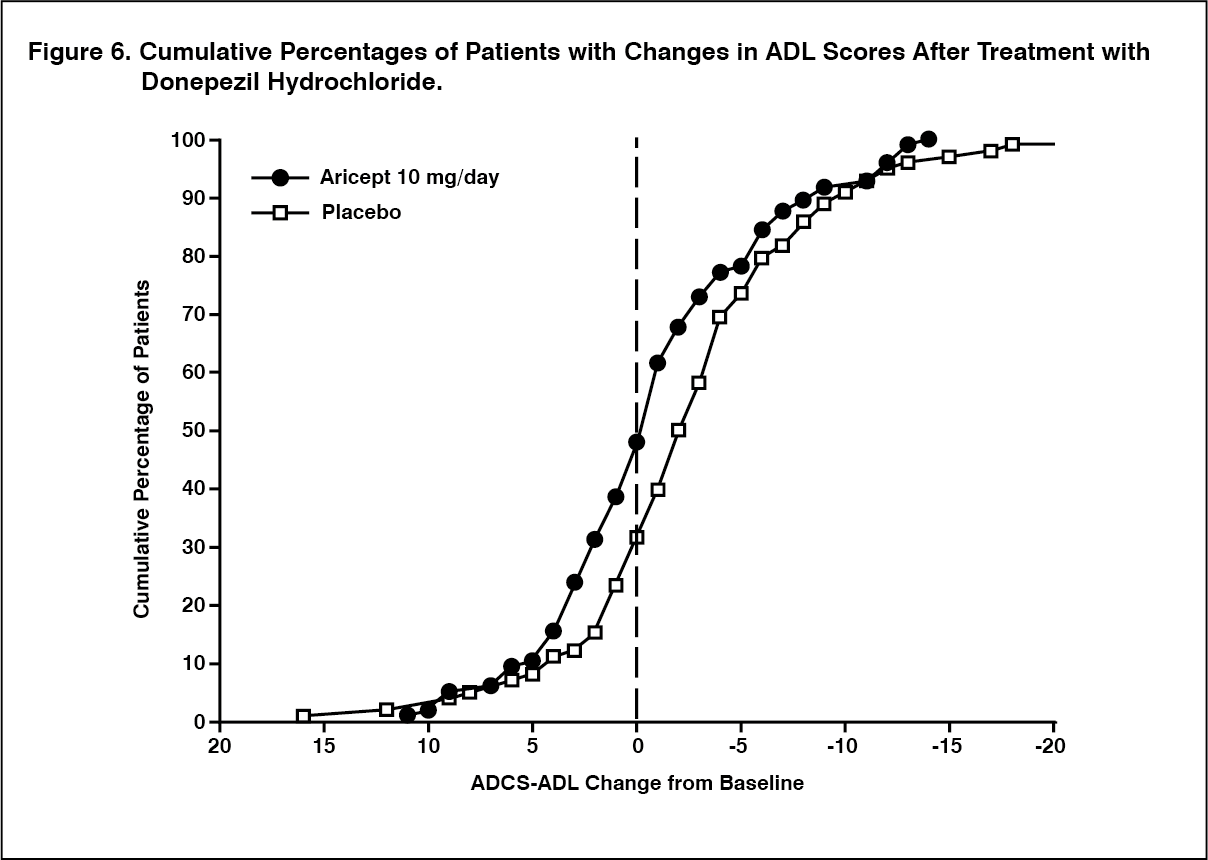 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image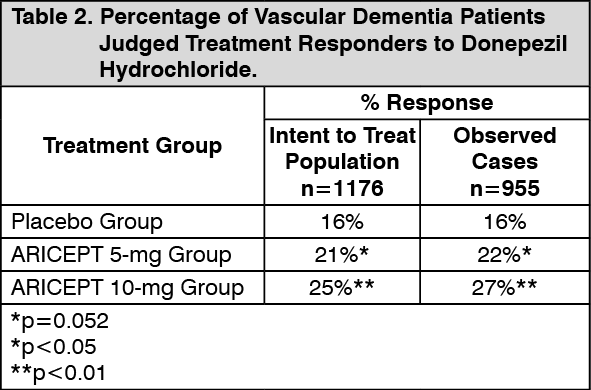 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image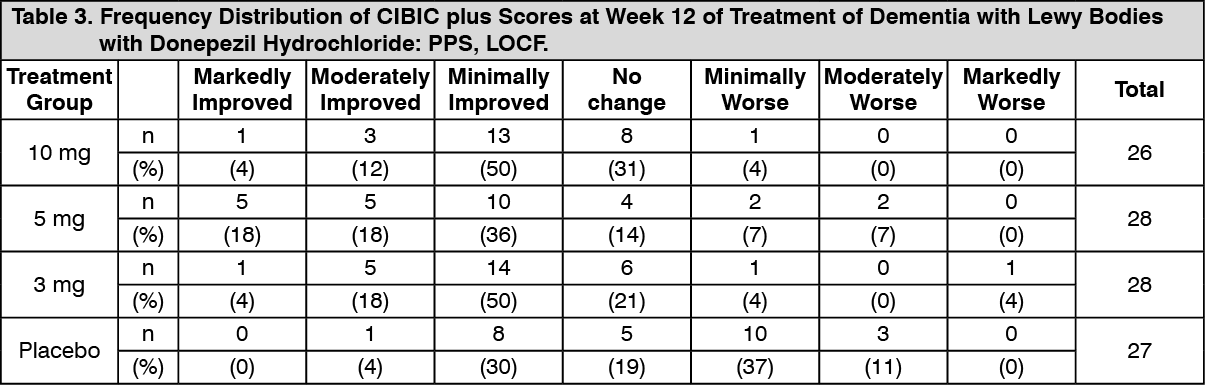 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image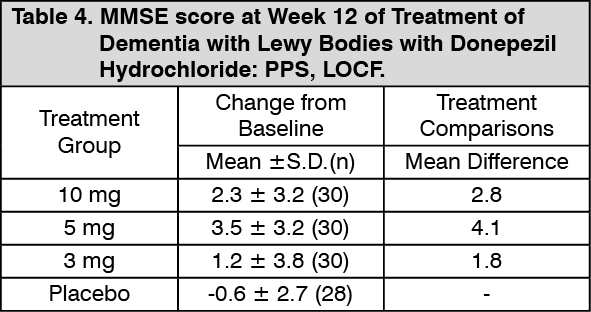 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image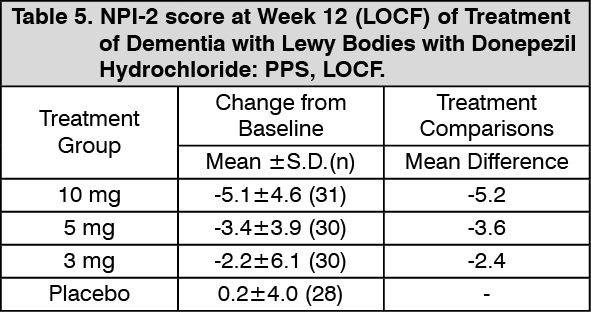 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image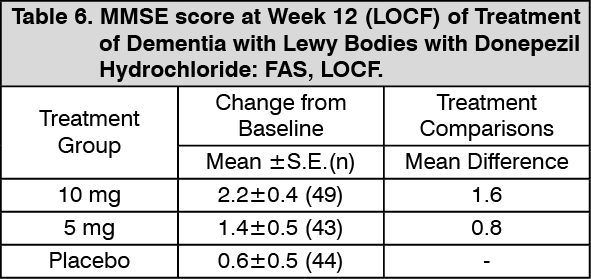 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image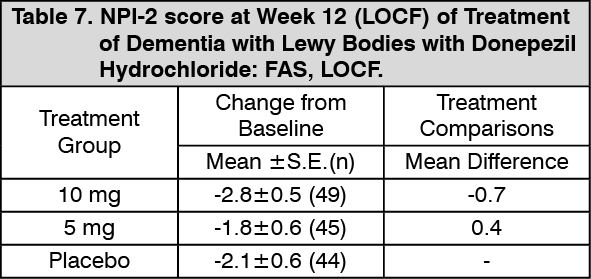 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image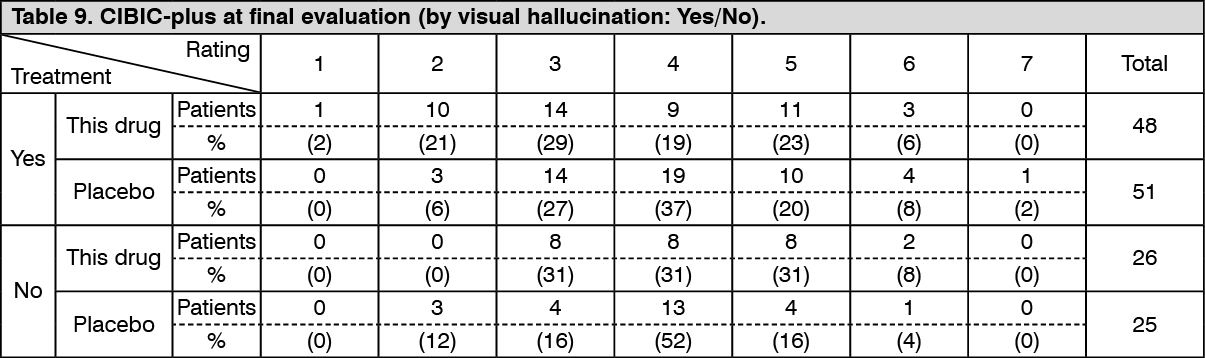 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image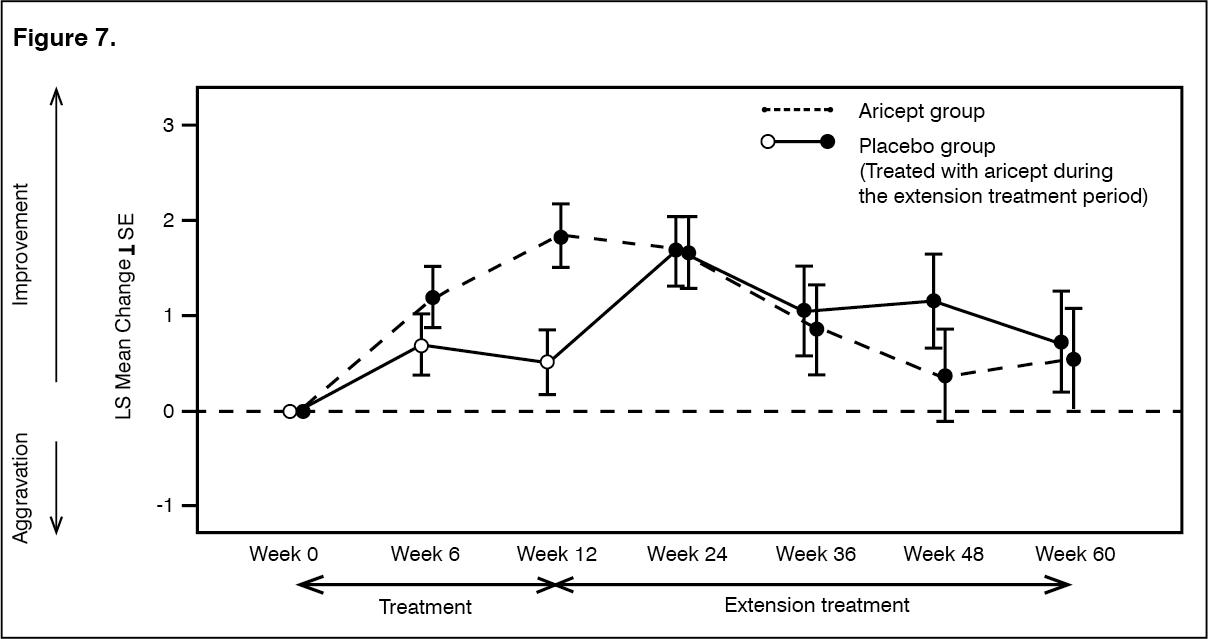 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out