Fixcom 2: Most TB patients complete their treatment without any significant adverse effects of drugs. However, a few patients do experience adverse effects. It is therefore important that patients be clinically monitored during treatment so that adverse effects can be detected promptly and managed properly. Routine laboratory monitoring is not necessary.
Health personnel can monitor adverse effects of drugs by teaching patients how to recognize symptoms of common adverse effects and to report if they develop such symptoms, and by asking about symptoms when patients report to collect drugs.
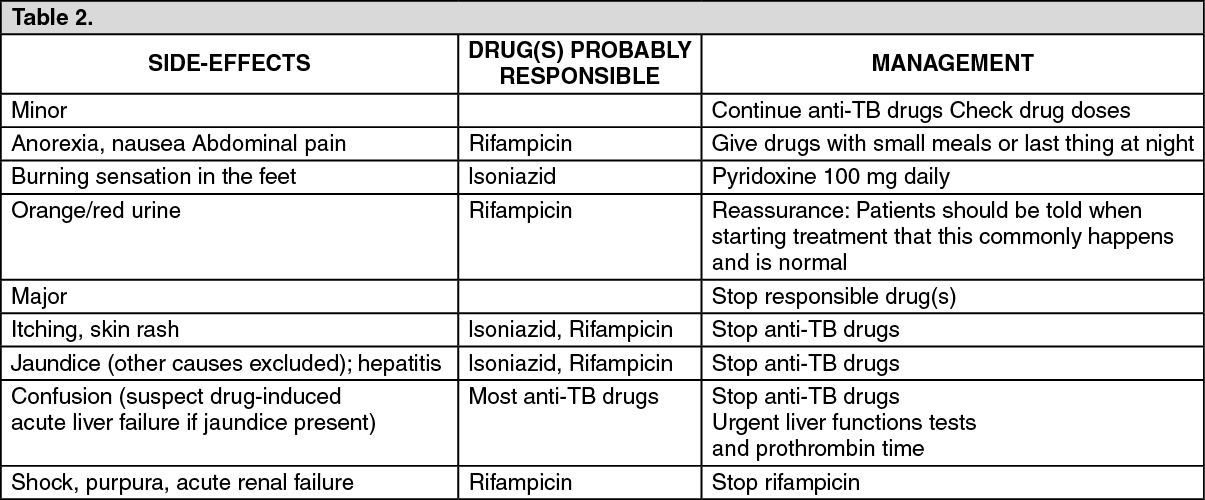
In general, a patient who develops minor adverse effects should continue the TB treatment, sometimes at a reduced dose. The patient also receives symptomatic treatment. If a patient develops a major side effect, the treatment or the offending drug is stopped. Further management depends on the nature of the adverse reaction.
Patients with major adverse reactions should be managed in a hospital. (See Table 2).
 Click on icon to see table/diagram/image
Fixcom 3: Rifampicin:
Click on icon to see table/diagram/image
Fixcom 3: Rifampicin: Rifampicin is usually well-tolerated. Adverse effects are more common during intermittent therapy or after restarting interrupted treatment.
Some patients may experience a cutaneous syndrome which presents 2-3 hrs after a daily or intermittent dose eg, facial flushing, itching, rash or rarely, eye irritation. A 12-hr "flu" syndrome of fever, chills, bone pains, shortness of breath and malaise has been associated with intermittent administration. It usually occurs after 3-6 months of intermittent administration and has a higher incidence with doses of ≥20 mg/kg body weight given once weekly than with currently recommended regimens. Anaphylaxis or shock has occurred rarely.
GI adverse effects include nausea, vomiting, anorexia, diarrhea and epigastric distress. GI bleeding and erosive gastritis, ulcerative and eosinophilic colitis have been reported. Administration on an empty stomach is recommended for maximal absorption, but this has to be balanced against administration after a meal to minimize GI intolerance. Pseudomembranous colitis has been reported. Rifampicin produces transient abnormalities in liver function. Hepatitis occurs rarely. Fatalities due to hepatotoxicity have been reported occasionally. Rifampicin can cause thrombocytopenia and purpura, usually when administered as an intermittent regiment and if this occurs, further administration of rifampicin is contraindicated. Other hematological adverse effects include eosinophilia, leucopenia and hemolytic anemia.
Alterations in kidney function and renal failure have occurred, particularly during intermittent therapy. Menstrual disturbances have been reported.
Nervous system adverse effects include headache, drowsiness, ataxia, dizziness and numbness.
Edema, myopathy and muscular weakness have been reported.
Rifampicin causes a harmless orange-red discoloration of the urine and other body fluids.
Isoniazid: Isoniazid is generally well-tolerated at currently recommended doses. However, patients who are slow acetylators of isoniazid appear to have a higher incidence of some adverse effects. Also, patients whose nutrition is poor are at risk of peripheral neuritis which is 1 of the commonest adverse effects of isoniazid. Other neurological adverse effects include psychotic reactions and convulsions. Pyridoxine may be given to prevent or treat these adverse effects. Transient increase in liver enzymes occur in 10-20% of patients during the 1st few months and usually return to normal despite continued treatment. Elevated liver enzymes associated with clinical signs of hepatitis eg, nausea and vomiting or fatigue may indicate hepatic damage: In these circumstances, isoniazid should be stopped pending evaluation and should only be reintroduced cautiously once hepatic functions has recovered. The incidence of liver damage is highest in patients >35 years. The influence of acetylator status is uncertain. Fatalities have occurred following liver necrosis. Hematological effects reported following use of isoniazid include various anemias, agranulocytosis, thrombocytopenia and eosinophilia.
Hypersensitivity reactions occur infrequently and include skin eruptions (including erythema multiforme), fever and vasculitis.
Other adverse effects include nausea, vomiting, pellagra, purpura, hyperglycemia, lupus-like syndrome, urinary retention and gynecomastia.
Ethambutol: The most important adverse effect of ethambutol is retrobulbar neuritis with a reduction in visual acuity, constriction of visual field, central or peripheral scotoma and green-red color blindness. One or both eyes may be affected. The degree of visual color blindness. One or both eyes may be affected. The degree of visual impairment appears to depend on the dose and duration of therapy; toxicity is observed most frequently at daily doses of 25 mg/kg body weight and after 2 months of therapy. Recovery of vision usually takes place over a period of a few weeks or months, but in rare cases, it may take up to ≥1 year or the effect may be permanent. Retinal hemorrhage has occurred rarely.
Renal clearance of urate may be reduced and acute gout has been precipitated rarely.
Hypersensitivity reactions including skin rashes, pruritus, leucopenia, fever and joint pains have occurred but appear to be rare with ethambutol. Other adverse effects which have been reported include confusion, disorientation, hallucinations, headache, dizziness, malaise, jaundice or transient liver dysfunction, peripheral neuritis, thrombocytopenia, pulmonary infiltrates, eosinophilia and GI disturbances eg, nausea, vomiting, anorexia and abdominal pain.
Fixcom 4: Pyrazinamide: Hepatotoxicity is the most serious side effect of pyrazinamide therapy and its frequency appears to be dose-related. However, in currently recommended dose, when given with isoniazid and rifampicin, the incidence of hepatitis has been reported to be <3%. Patients may experience transient increase in liver enzyme values, more seriously hepatomegaly, splenomegaly and jaundice may develop and on rare occasions, death has occurred. Hyperuricemia commonly occurs and may lead to attacks of gout. Other side effects are anorexia, nausea, vomiting, arthralgia, malaise, fever, sideroblastic anemia and dysuria. Photosensitivity and skin rashes have been reported on rare occasions.

 Sign Out
Sign Out