Pharmacology: Mechanism of Action: FSH is required for folliculogenesis, it stimulates growth of the preantral follicle, maturation of preantral follicle in preovulatory follicle by bringing about granulose cell aromatase activity and enzymes involved in progesterone biosynthesis. FSH also triggers receptor for luteinizing hormone on granulosa cells that leads to ovulation and development of corpus luteum in response to mid-cycle luteinizing hormone surge. Exogenous FSH stimulation has a specific role in follicular recruitment and dominant follicle selection. In normal ovulatory cycle, increase in FSH levels during luteo-follicular transition phase causes sustained growth of 5 to 10 antral follicle in each ovary. However, the FSH levels decline in response to negative feedback mechanism of estradiol and inhibin in late follicular stage thus only a single dominant follicle with increased receptivity to FSH grows, and other follicles undergo atresia. Exogenous FSH administration expands the FSH window thus resulting in pool of maturing follicles that attains dominance and do not undergo atresia.
Clinical Trials: Several studies have been conducted to determine the efficacy of urofollitropin as a method of inducing ovulation. Urofollitropin seems to be as effective as recombinant follicle
stimulating hormone for ovulation induction.
In a study by Liu et al , the efficacy of urinary follicle stimulating hormone (FSH) was compared with recombinant follicle stimulating hormone in females undergoing assisted reproductive technique. A total of 508 females over 37 years of age were recruited in the study. Patients were randomized into two groups; group 1 received recombinant FSH and group 2 received urinary FSH. Long down-regulation protocol with gonadotropin releasing hormone (GnRH) analogue was used for suppression. The outcomes assessed were days of stimulation, estradiol (E2) level on the day of human chorionic gonadotropin (hCG) administration, endometrial thickness at hCG day, number of oocytes retrieved, amount of FSH used, quantity of FSH/oocyte, 2PN zygote rate, grade І embryo rate, number of embryos cryopreserved, implantation rate, pregnancy rate, abortion rate and the rate of nontransferable embryos. The results showed, individuals treated with urinary FSH had considerably higher 2PN zygote rate and grade I embryo rate as compared to recombinant FSH treatment. The endometrial thickness on the day of hCG administration was 11.8 mm in urinary FSH group and 11.2 mm in recombinant FSH group. Other measures were similar in both the groups. Urinary FSH produced more grade I embryos with lower chances of nontransferable embryos. Both the agents were equipotent.
Cochrane conducted a systemic review to compare the efficacy and tolerability of urinary FSH and recombinant FSH as a method of inducing ovulation in females with polycystic ovarian syndrome resistant to
clomiphene therapy. A total of six randomized controlled trials were included in the study. Three of these trials compared urinary FSH with recombinant FSH.
Ovulation, evidence of clinical pregnancy, miscarriage, multiple pregnancy, ovarian stimulation syndrome, total dose used and total duration of stimulation were estimated.
The data revealed no difference in any outcomes with urinary FSH and recombinant FSH.
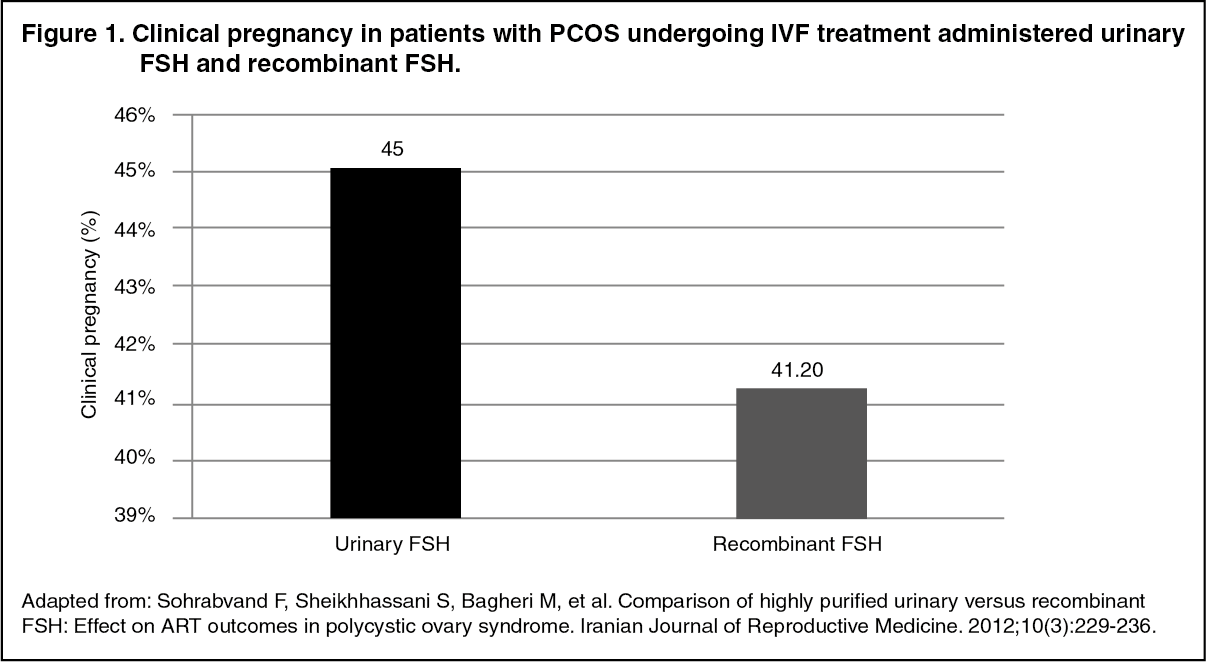
A trial was conducted in patients with PCOS undergoing assisted reproduction technique with ovulation induction using either urinary FSH or recombinant FSH. A group of 623 patients was included in the study. Patients underwent down regulation with GnRH analogue. Patients were randomized into two groups; each received either urinary FSH (n=80) or recombinant FSH (n=80). Clinical pregnancy was evident in 45% patients receiving urinary FSH as against 41.2% patients receiving recombinant FSH (Figure 1). The total number of oocyte retrieved was more in urinary FSH group.
Additionally, quality and number of embryos was also better in urinary FSH group.
Endometrial thickness was 10.36±1.35 mm in group receiving urinary FSH. Both urinary and recombinant form of FSH appeared to have similar effect on ART outcomes in PCOS patients.
Clinical efficacy of low-dose step up and step down protocols of urofollitropin were compared in a study among normogonadotropic clomiphene-resistant infertile females. The following parameters were compared: duration of treatment, ovarian stimulation (serum FSH levels) and response to the therapy (assessed by measuring serum estradiol levels and number and size of follicles). The duration of treatment in step-up group was 18 days and in step-down group was 9 days. The serum FSH levels from the first day of ovarian response until the administration of hCG were constant.
Monofollicular growth was evident in 56% patients in low dose step up group and 88% patients in step down group. A total of 33% and 71% patients had normal range periovulatory estradiol levels in low dose step up and step down group, respectively. The efficacy of step down protocol appeared rational. Step down regimen was associated with shorter duration of treatment, higher number of monofollicular cycles and more probability of periovulatory E2 levels within the normal range.
The efficacy of highly purified urofollitropin used for ovarian stimulation was assessed in a parallel randomized open-label 8 trial conducted in assisted reproduction centers. The effect of highly purified urofollitropin on oocyte and embryo quality was determined. A total of 267 infertile couples undergoing in vitro fertilization were recruited in the study. Highly purified urinary FSH was administered to 133 patients and recombinant FSH was administered to 134 patients. The number of morphologically mature oocytes retrieved, embryo quality and pregnancy and implantation rates were assessed. Pregnancy and implantation rates in urinary FSH group were higher than recombinant group (Figure 2) (pregnancy rate: 46.5% and 36.8%; implantation rate: 22.1% and 15.8%). The grade 1 embryo score was appreciably higher in group receiving urinary FSH as compared to recombinant FSH.
Number live birth was higher in urinary FSH group compared to recombinant FSH group.
The findings attested the efficacy of highly purified urinary FSH.
Baker and colleagues compared the efficacy of highly purified urinary follicle stimulating hormone and human recombinant follitropin alpha in patients undergoing ovarian stimulation for IVF. A total of 152 IVF patients were recruited in the study; 76 patients received highly purified urinary follicle stimulating hormone and 76 patients received recombinant follitropin alpha. The number of oocytes retrieved was comparable in both the groups. Clinical pregnancy rate was 48.7% in highly purified urinary follicle stimulating hormone group and 44.7% in recombinant follicle stimulating hormone group. Live birth rate was 38.2% in both the groups (Figure 3). Highly purified urinary follicle stimulating hormone and recombinant follicle stimulating hormone were equally efficacious.
A study examined the efficacy of highly purified human follicle stimulating hormone after subcutaneous administration for follicular development in females undergoing IVF. A group of 139 patients was initially recruited for the study. Highly purified human follicle stimulating hormone was started in 122 patients, of which 118 patients received 10,000 I.U. of human chorionic gonadotropin hormone for follicular maturation and oocyte recovery. The mean plasma luteinizing hormone concentrations at baseline was 1.6 ± 0.8 mIU/ml which reduced significantly by the day of human chorionic hormone
administration (1.2±0.8 mIU/ml). In patients who received human chorionic gonadotropin after highly purified human urinary follicle stimulating hormone, mean number of oocytes retrieved were 8.4 ± 4.7. Embryo transfer took place in 86% patients of which 23% patients attained clinical pregnancy and 15% live births occurred. Thus, the efficacy of highly purified urinary follicle stimulating hormone was confirmed. (See Figures 1, 2, and 3).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics: Follicle stimulating hormone exists in several isoforms. The metabolism of FSH isoforms occurs in the liver. The liver metabolism of acidic isoforms is lower as compared to less acidic isoforms. Urinary FSH contains more of acidic isoforms. The acidic isoforms have a longer plasma half life and slow clearance associated with higher biological activity.
A study evaluated the pharmacokinetics of highly purified urinary human follicle stimulating hormone and standard urinary follicle stimulating hormone. Both the preparations were administered as single dose of 150 I.U. as intravenous injection and as intramuscular or subcutaneous injections. The pharmacokinetic parameters were similar for both the preparations after intravenous administration. Immunoassay of follicle stimulating hormone showed that renal clearance was 0.1 I/h, volume of distribution at steady state was 9 I, distribution was 2 hours and terminal half-life was 17 hours. After parental administration, the absorption half-life of follicle stimulating hormone was 3 hours and terminal half-life was 1.5 days. The bioavailability was 100% for intramuscular
and subcutaneous route.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image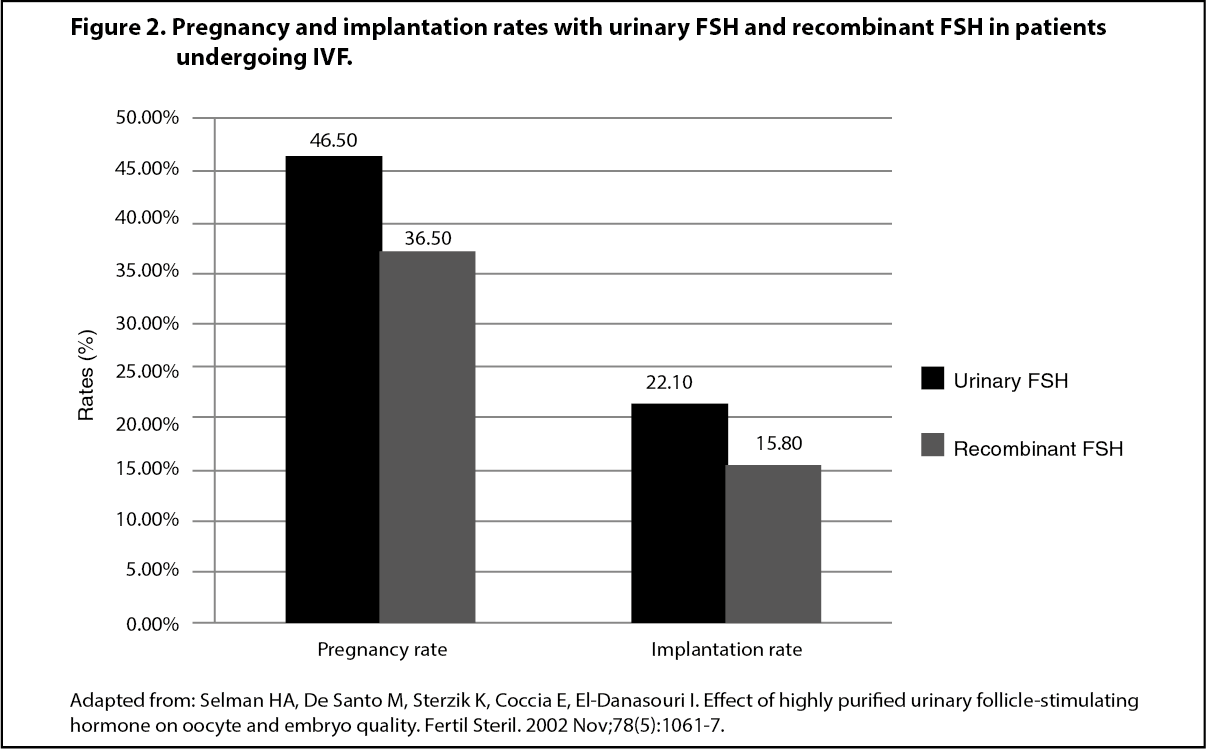 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out