Montelukast & Levocetirizine are generally well tolerated. Common side effects, which might be seen with the combination, are dyspepsia, abdominal pain, rash, dizziness, headache, fatigue, and somnolence. Sometimes, hypersensitivity, irritability, restlessness, insomnia, vomiting and diarrhoea may occur. In rare cases, patients may present with systemic eosinophilia, sometimes presenting with clinical features of consistent with Churg-Strauss Syndrome.
Adults and adolescents above 12 years of age: In therapeutic studies in women and men aged 12 to 71 years, 15.1% of the patients in the levocetirizine 5 mg group had at least one adverse drug reaction compared to 11.3% in the placebo group. 91.6 % of these adverse drug reactions were mild to moderate.
In therapeutic trials, the dropout rate due to adverse events was 1.0% (9/935) with levocetirizine 5 mg and 1.8% (14/771) with placebo.
Clinical therapeutic trials with levocetirizine included 935 subjects exposed to the medicinal product at the recommended dose of 5 mg daily. From this pooling, following incidence of adverse drug reactions were reported at rates of 1 % or greater (common: ≥1/100 to <1/10) under levocetirizine 5 mg or placebo: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Further uncommon incidences of adverse reactions (uncommon ≥1/1000, <1/100) like asthenia or abdominal pain were observed.
The incidence of sedating adverse drug reactions such as somnolence, fatigue, and asthenia was altogether more common (8.1 %) under levocetirizine 5 mg than under placebo (3.1%).
Paediatric population: In two placebo-controlled studies in pediatric patients aged 6-11 months and aged 1 year to less than 6 years, 159 subjects were exposed to levocetirizine at the dose of 1.25 mg daily for 2 weeks and 1.25 mg twice daily respectively. The following incidence of adverse drug reactions was reported at rates of 1% or greater under levocetirizine or placebo. (See Table 2.)
Click on icon to see table/diagram/image
In children aged 6-12 years double blind placebo controlled studies were performed where 243 children were exposed to 5 mg levocetirizine daily for variable periods ranging from less than 1 week to 13 weeks. The following incidence of adverse drug reactions was reported at rates of 1% or greater under levocetirizine or placebo. (See Table 3.)
Click on icon to see table/diagram/image
The frequency is defined as follows: Very common (≥1/10); Common (≥1/100 to <1/10); Uncommon (≥1/1,000 to <1/100); Rare (≥1/10,000 to <1/1,000); Very rare (≤1/10,000) Not known (cannot be estimated from the available data).
Immune system disorders: Not known: hypersensitivity including anaphylaxis.
Metabolism and nutrition disorders: Not known: increased appetite.
Psychiatric disorders: Not known: aggression, agitation, hallucination, depression, insomnia, suicidal ideation, nightmare.
Nervous system disorders: Not known: convulsion, paraesthesia, dizziness, syncope, tremor, dysgeusia.
Ear and labyrinth disorders: Not known: vertigo.
Eyes disorders: Not known: visual disturbances, blurred vision, oculogyration.
Cardiac disorders: Not known: palpitations, tachycardia.
Gastrointestinal disorders: Not known: nausea, vomiting, diarrhea.
Hepatobiliary disorders: Not known: hepatitis.
Renal and urinary disorders: Not known: dysuria, urinary retention.
Skin and subcutaneous tissue disorders: Not known: angioneurotic edema, fixed drug eruption, pruritus, rash, urticaria.
Musculoskeletal, connective tissues, and bone disorders: Not known: myalgia, arthralgia.
General disorders and administration site conditions: Not known: edema.
Montelukast has been evaluated in clinical studies as follows: The following drug-related adverse reactions in clinical studies were reported commonly (1/100 to <1/10) in asthmatic patients treated with montelukast and at a greater incidence than in patients treated with placebo: See Table 4.
Click on icon to see table/diagram/image
With prolonged treatment in clinical trials with a limited number of patients for up to 2 years for adults, and up to 12 months for paediatric patients 6 to 14 years of age, the safety profile did not change.
Tabulated list of Adverse Reactions: Adverse reactions reported in post-marketing use are listed, by System Organ Class and specific Adverse Experience Term, in the table as follows. Frequency Categories were estimated based on relevant clinical trials. (See Table 5.)
Click on icon to see table/diagram/image


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image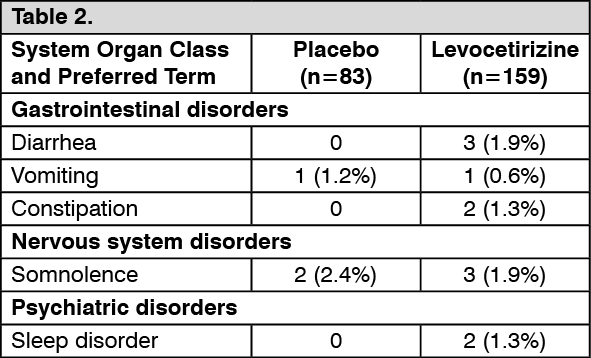 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image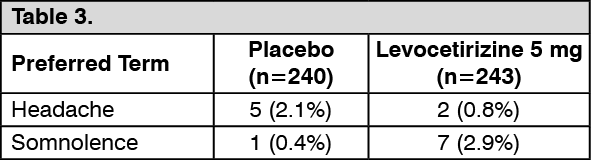 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image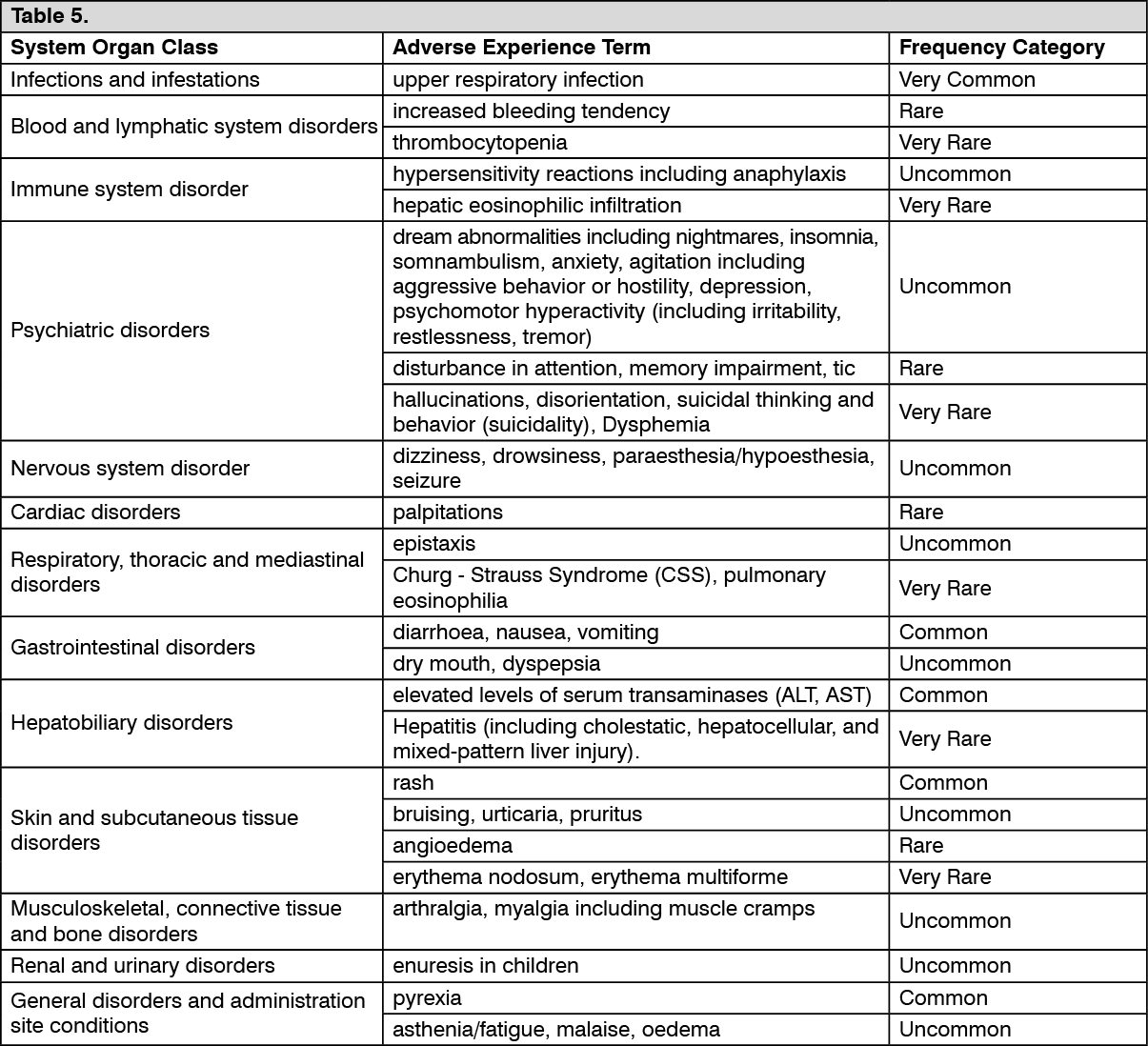 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out