Most Common: Dizziness, somnolence.
Body as a Whole: Asthenia, accidental injury, back pain, chest pain, face edema, infection, headache, pain, flu syndrome.
Digestive: Dry mouth, constipation, flatulence, vomiting, increased appetite, abnormal distention.
General Disorders and Administrative Site Conditions: Fatigue, peripheral edema, chest pain, feeling abnormal, edema, feeling drunk.
Infections and Infestations: sinusitis, nasopharyngitis.
Metabolic and Nutritional: Peripheral edema, weight gain, edema, hypoglycemia.
Musculoskeletal and Connective Tissue Disorders: Myasthenia, arthralgia, muscle spasms, back pain, pain in extremity, muscular weakness, neck pain, joint swelling.
Nervous: Dizziness, somnolence, neuropathy, ataxia, vertigo, confusion, euphoria, incoordination, thinking abnormal, tremor, abnormal gait, amnesia, nervousness, speech disorder, twitching, confusion, myoclonus, disturbance in attention, memory impairment, hypoesthesia, lethargy, paresthesia.
Psychiatric: Euphoric mood, confusional state, anxiety, disorientation, depression, insomnia.
Respiratory, Thoracic, and Mediastinal Disorders: Dyspnea, bronchitis, pharyngolaryngeal pain.
Skin and Subcutaneous Tissue Disorders: Decubitus ulcer.
Special Senses: Blurred vision, abnormal vision, diplopia, eye disorder, vertigo.
Urogenital: Urinary incontinence.
Vascular: Hypertension, hypotension.
Other:
Body as a Whole: Frequent: Abdominal pain, allergic reaction, fever. Infrequent: Abscess, cellulitis, chills, malaise, neck rigidity, overdose, pelvic pain.
Photosensitivity Reaction: Rare: Anaphylactoid reaction, ascites, granuloma, hangover effect, intentional injury, retroperitoneal fibrosis, shock.
Cardiovascular System: Infrequent: Deep thrombophlebitis, heart failure, hypotension, postural hypotension, retinal vascular disorder, syncope. Rare: ST depressed, ventricular fibrillation.
Digestive System: Frequent: Gastroenteritis, increased appetite. Infrequent: Cholecystitis, cholelithiasis, colitis, dysphagia, esophagitis, gastritis, gastrointestinal hemorrhage, melena, mouth ulceration, pancreatitis, rectal hemorrhage, tongue edema. Rare: Aphthous stomatitis, esophageal ulcer, periodontal abscess.
Hemic and Lymphatic System: Frequent: Ecchymosis. Infrequent: Anemia, eosinophilia, hypochromic anemia, leukocytosis, leukopenia, lymphadenopathy, thrombocytopenia. Rare: Myelofibrosis, polycythemia, prothrombin decreased, purpura, thrombocythemia.
Metabolic and Nutritional Disorders: Rare: Glucose tolerance decreased, urate crystalluria.
Musculoskeletal System: Frequent: Arthralgia, leg cramps, myalgia, myasthenia. Infrequent: Arthrosis. Rare: Chondrodystrophy, generalized spasm.
Nervous System: Frequent: Anxiety, depersonalization, hypertonia, hypoesthesia, libido decreased, nystagmus, paresthesia, sedation, stupor, twitching. Infrequent: Abnormal dreams, agitation, apathy, aphasia, circumoral paresthesia, dysarthria, hallucinations, hostility, hyperalgesia, hyperesthesia, hyperkinesia, hypokinesia, hypotonia, libido increased, myoclonus, neuralgia. Rare: Addiction, cerebellar syndrome, cogwheel rigidity, coma, delirium, delusions, dysautonomia, dyskinesia, dystonia, encephalopathy, extrapyramidal syndrome, Guillain-Barre syndrome, hypalgesia, intracranial hypertension, manic reaction, paranoid reaction, peripheral neuritis, personality disorder, psychotic depression, schizophrenic reaction, sleep disorder, torticollis, trismus.
Respiratory System: Rare: Apnea, atelectasis, bronchiolitis, hiccup, laryngismus, lung edema, lung fibrosis, yawn.
Skin Appendages: Frequent: Pruritus. Infrequent: Alopecia, dry skin, eczema, hirsutism, skin ulcer, urticaria, vesiculobullous rash. Rare: Angioedema, exfoliative dermatitis, lichenoid dermatitis, melanosis, nail disorder, petechial rash, purpuric rash, pustular rash, skin atrophy, skin necrosis, skin nodule, Stevens-Johnson syndrome, subcutaneous nodule.
Special Senses: Frequent: Conjunctivitis, diplopia, otitis media, tinnitus. Infrequent: Abnormality of accommodation, blepharitis, dry eyes, eye hemorrhage, hyperacusis, photophobia, retinal edema, taste loss, taste perversion. Rare: Anisocoria, blindness, corneal ulcer, exophthalmos, extraocular palsy, iritis, keratitis, keratoconjunctivitis, miosis, mydriasis, night blindness, opthalmoplegia, optic atrophy, papilledema, parosmia, ptosis, uveitis.
Urogenital System: Frequent: Anorgasmia, impotence, urinary frequency, urinary incontinence. Infrequent: Abnormal ejaculation, albuminuria, amenorrhea, dysmenorrhea, dysuria, hematuria, kidney calculus, leukorrhea, menorrhagia, metrorrhagia, nephritis, oliguria, urinary retention, urine abnormality. Rare: Acute kidney failure, balanitis, bladder neoplasm, cervicitis.
Post Marketing Experience:
Nervous System Disorders: Headache.
Gastrointestinal Disorders: Nausea, diarrhea.
Reproductive System and Breast Disorders: Gynecomastia, breast enlargement.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image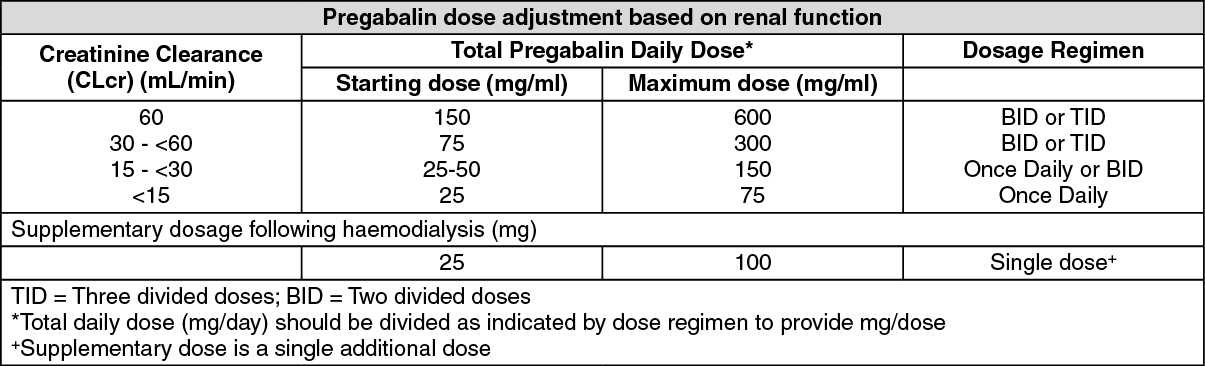 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
