General: Fatigue, hypersensitivity reactions (e.g., bronchospasm, anaphylaxis and angioedema).
Cardiovascular: Tachycardia, palpitations, hypotension.
Gastrointestinal: Dry mouth, GI disturbance including nausea and vomiting, diarrhea.
Hematologic: Blood disorders.
Hepatic: Liver dysfunction.
Musculoskeletal: Muscle twitching, muscular weakness, myalgia.
Nervous System: Sedation, drowsiness, disturbance in attention, unsteadiness, dizziness, convulsions, headache, paresthesia, dyskinesia, confusion, paradoxical excitation (e.g., increased energy, restlessness, nervousness), incoordination, euphoria, extrapyramidal effects, depression, sleep disturbances, tremors.
Renal: Urinary difficulty, urinary retention, dysuria.
Respiratory: Thickening of bronchial secretions, tightness of chest, dyspnea.
Skin and Appendages: Rash, urticaria, photosensitivity reactions, sweating, hair loss.
Special Senses: Blurred vision, tinnitus.


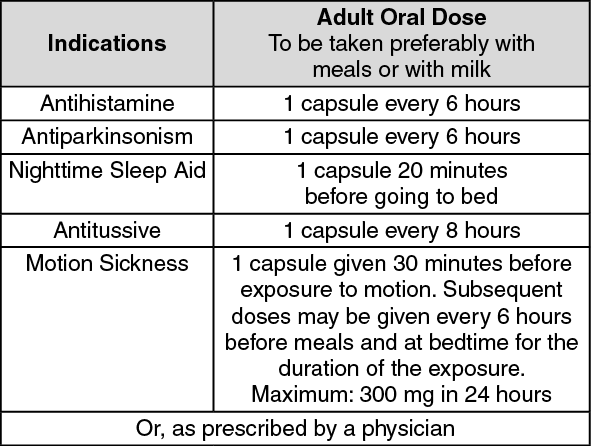 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out