The most frequently reported adverse effects with lansoprazole include diarrhea, abdominal pain, nausea, constipation, headache, dizziness, vomiting, flatulence, dry mouth or throat, urticaria, itching, rash, and fatigue.
Infections and infestations: Bronchitis,
Clostridium difficile-associated diarrhea, conjunctivitis, otitis media, pneumonia, pseudomembranous colitis, upper respiratory tract infection.
Neoplasms benign, malignant and unspecified (including cysts and polyps): Carcinoid, carcinoma, skin carcinoma.
Blood and lymphatic system disorders: Agranulocytosis, anemia, aplastic anemia, eosinophilia, hemolysis, hemolytic anemia, jaundice, leukopenia, lymph adenopathy, neutropenia, pancytopenia, thrombocytopenia.
Immune system disorders: Allergic reaction, anaphylactic reactions, asthma, erythema multiforme, ulcerative colitis.
Endocrine disorders: Abnormal menses, goiter, hypothyroidism.
Metabolism and nutrition disorders: Anorexia, avitaminosis, dehydration, diabetes mellitus, edema, hunger, hyperglycemia, hyperlipidemia, hypoglycemia, hypomagnesemia, hyponatremia, increased appetite, peripheral edema, thirst.
Psychiatric disorders: Abnormal dreams, aggression, agitation, anxiety, apathy, confusion, dementia, depersonalization, depression, emotional lability, hallucinations, hoarseness, hostility aggravated, insomnia, nervousness, neurosis, sleep disorder, somnolence.
Nervous system disorders: Amnesia, cerebrovascular accident, convulsion, diplopia, hemiplegia, hyperkinesia, hypoesthesia, migraine, myasthenia, numbness of tongue or lips, paresthesia, ptosis, speech disorders, taste loss, taste perversion, thinking abnormality, tremor, vertigo.
Eye disorders: Abnormal vision, amblyopia, blepharitis, blurred vision, cataract, dry eyes, eye pain, glaucoma, photophobia, retinal degeneration, visual disturbances, visual field defect.
Ear and labyrinth disorders: Deafness, tinnitus.
Cardiac disorders: Arrhythmia, bradycardia, chest pain, dyspnea, myocardial infarction, palpitations, tachycardia.
Vascular disorders: Epistaxis, hemoptysis, hypertension, hypotension, rectal hemorrhage, shock (circulatory failure), syncope, vasodilation.
Respiratory, thoracic and mediastinal disorders: Cough, flu syndrome, interstitial pneumonia, laryngeal neoplasia, lung fibrosis, parosmia, pharyngitis, pleural disorder, rhinitis, sinusitis, stridor, upper respiratory tract inflammation.
Gastrointestinal disorders: Abnormal stools, bezoar, candidiasis of the esophagus, cardiospasm, colitis, duodenitis, dyspepsia, dysphagia, enlarged abdomen, enteritis, epigastric discomfort, eructation, esophageal stenosis, esophageal ulcer, esophagitis, fecal discoloration, fundic gland polyps, gastritis, gastroenteritis, gastrointestinal anomaly, gastrointestinal hemorrhage, gastrointestinal moniliasis, glossitis, gum hemorrhage, halitosis, hematemesis, hiatal hernia, hiccup, impaired gastric emptying, increased salivation, melena, mouth ulceration, oral moniliasis, pancreatitis, rectal disorder, stomatitis, tongue disorder, tooth disorder, ulcerative stomatitis.
Hepatobiliary disorders: Cholelithiasis, hepatitis, hepatotoxicity.
Skin and subcutaneous tissue disorders: Acne, alopecia, dry skin, fixed eruption, hair disorder, maculopapular rash, nail disorder, petechiae, pruritus, Stevens-Johnson syndrome, subacute cutaneous lupus erythematosus, thrombotic thrombocytopenic purpura, toxic epidermal necrolysis.
Musculoskeletal and connective tissue disorders: Arthralgia, arthritis, back pain, bone disorder, chills, gout, hypertonia, joint disorder, leg cramps, musculoskeletal pain, myalgia, neck pain, neck rigidity, synovitis, tenesmus.
Renal and urinary disorders: Dysuria, interstitial nephritis, kidney calculus, kidney pain, polyuria, renal impairment, urethral pain, urinary frequency, urinary retention, urinary tract infection, urinary urgency.
Reproductive system and breast disorders: Breast enlargement, breast pain, breast tenderness, dysmenorrhea, gynecomastia, impotence, increased/decreased libido, leukorrhea, menorrhagia, menstrual disorder, pelvic pain, penis disorder, testis disorder, vaginitis.
General disorders and administration site conditions: Asthenia, crepitations, fever, general pain, malaise, metaplasia, sweating.
Investigations: Abnormal liver function tests, elevated alanine aminotransferase, weight gain/loss.
Injury, poisoning and procedural complications: Bone fracture, contact dermatitis, contusion.


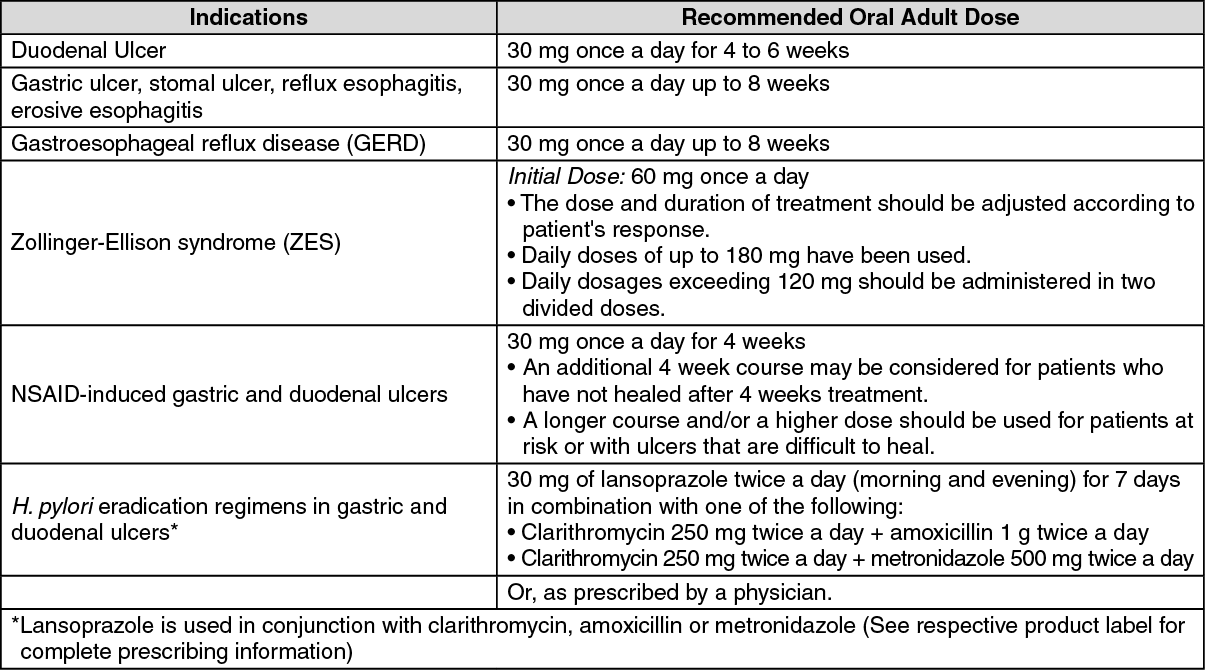 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out