Sustained-release tablet: Each sustained-release tablet contains: Metformin hydrochloride 500 mg.
Pharmacology: Tablet: Metformin HCl is a biguanide oral antihyperglycemic agent. It improves glucose tolerance in type 2 diabetes mellitus patients and lowers both basal and postprandial plasma glucose. Metformin decreases hepatic glucose production and improves insulin sensitivity by increasing peripheral glucose uptake and utilization.
Metformin has beneficial effects on serum lipid profiles in patients with type 2 diabetes. It lowers mean fasting serum triglycerides, total cholesterol and low-density lipoprotein cholesterol levels and has no adverse effects on other lipid levels. Increased fibrinolytic activity and decreased platelet aggregability have been observed in diabetic patients after treatment with metformin.
Sustained-release tablet: Metformin is a biguanide antidiabetic agent that reduces both basal and postprandial plasma glucose concentrations in patients with type 2 diabetes mellitus by improving both peripheral and hepatic sensitivity to insulin. It does not stimulate insulin secretion and therefore does not produce hypoglycemia when used alone. Fasting insulin levels and day-long insulin response remain the same or may even decrease with metformin therapy.
Metformin may act via three mechanisms: It reduces hepatic glucose production by inhibiting gluconeogenesis and glycogenolysis; increases insulin sensitivity in the skeletal muscles and adipocytes, improving peripheral glucose uptake and utilization; delays intestinal glucose absorption.
Metformin stimulates intracellular glycogen synthesis by acting on glycogen synthase. It also increases the transport capacity of all types of membrane glucose transporters.
Metformin has demonstrated modest favorable effects on lipid metabolism in patients with type 2 diabetes. It lowers total cholesterol, mean fasting serum triglycerides and low density lipoprotein cholesterol levels; it has no adverse effects on other lipid levels.
Pharmacokinetics: Tablet: Metformin HCl, when given in fasting conditions, has a bioavailability of 50-60%. Food decreases the extent and slightly delays the absorption of metformin. It is negligibly bound to plasma proteins. It partitions into erythrocytes, most likely as a function of time. Steady-state plasma concentrations are reached within 24-48 hrs and are generally <1 mcg/mL. Following oral administration, approximately 90% of the absorbed Metformin is eliminated via the renal route within the first 24 hrs. The plasma elimination half-life of metformin is approximately 6.2 hrs.
Sustained-release tablet: Metformin HCl sustained-release tablet is intended for once a day dosing. Once a day dosing is possible through control of metformin release rate and prolonging absorption in the upper gastrointestinal tract.
At steady-state, after administration of sustained-release metformin tablet, the AUC and peak plasma concentrations are not dose proportional within the range of 500 mg to 2,000 mg. Time to reach maximum plasma concentrations (Tmax) is approximately 7 hours (range from 4 to 8 hours). The extent of metformin absorption (based on AUC) for metformin sustained-release tablet at 2,000 mg once a day dose is similar as that for metformin immediate-release tablet at 1,000 mg twice a day dose.
Metformin distributes rapidly to peripheral body tissues and fluids. It also appears to distribute slowly into erythrocytes and into a deep tissue compartment. Metformin is negligibly bound plasma proteins. Steady-state plasma concentration of metformin are generally <1 mcg/mL and are reached within 24 to 48 hours at usual clinical doses and dosing schedules.
Renal elimination of metformin is via glomerular filtration and secretion by the proximal convolutes tubules as unchanged drug. The principal plasma elimination half-life of metformin is about 6.2 hours with 90% of the total dose being cleared within 24 hours in patients with normal renal function. In blood, the elimination half-life is about 17.6 hours.
Special Populations: Renal Insufficiency: The plasma and blood half-life of metformin is prolonged and the renal clearance decreased in proportion to the decrease in creatinine clearance in patients with decreased renal function (based on measured creatinine levels).
Geriatrics: The limited pharmacokinetic data of metformin in healthy elderly subjects suggest that total plasma clearance of metformin is decreased, half-life is prolonged, and Cmax is increased, compared to healthy young subjects. It appears that the change in metformin pharmacokinetics with aging is primarily related to a change in renal function.
Pediatrics: The safety and efficacy of metformin HCl sustained-release tablet has not been established in pediatric patients. Pharmacokinetic studies have not been conducted in these patients.
Tablet: As an adjunct to diet and exercise to lower blood glucose in type 2 diabetes patients whose hyperglycemia cannot be controlled by diet and exercise alone.
Metformin can be used alone or in combination with other oral antidiabetic agents or with insulin.
Sustained-release tablet: As an adjunct to diet and exercise to improve glycemic control in patients with type 2 diabetes mellitus.
Metformin may be used as monotherapy or in combination with other oral antidiabetic agents or with insulin.
Tablet: Individualize dosage on the basis of both effectiveness and tolerance but should not exceed 2550 mg/day.
500-mg Tablet: Usual Starting Dose: 500 mg every 12 hrs, given with or after meals. Dosage increases should be made in increments of 500 mg every week, given in divided doses. Maximum Dose: 2000 mg/day.
850-mg Tablet: Usual Starting Dose: 850 mg once a day, given with or after meals. Dosage increases should be made in increments of 850 mg every other week, given in divided doses. Maximum Dose: 2550 mg/day. Usual Maintenance Dose: 850 mg twice a day, with or after meals. When necessary, patients may be given 850 mg 3 times a day with meals. Dosage can also be increased from 500 mg twice a day to 850 mg twice a day after 2 weeks.
Patients requiring additional glycemic control: Maximum Dose: 2550 mg/day. Doses >2000 mg may be better tolerated given 3 times a day with meals.
Metformin HCl should be given in divided doses with meals and should be started at a low dose, with gradual dose escalation, both to reduce GI side effects and to permit identification of the minimum dose required for adequate glycemic control of the patient.
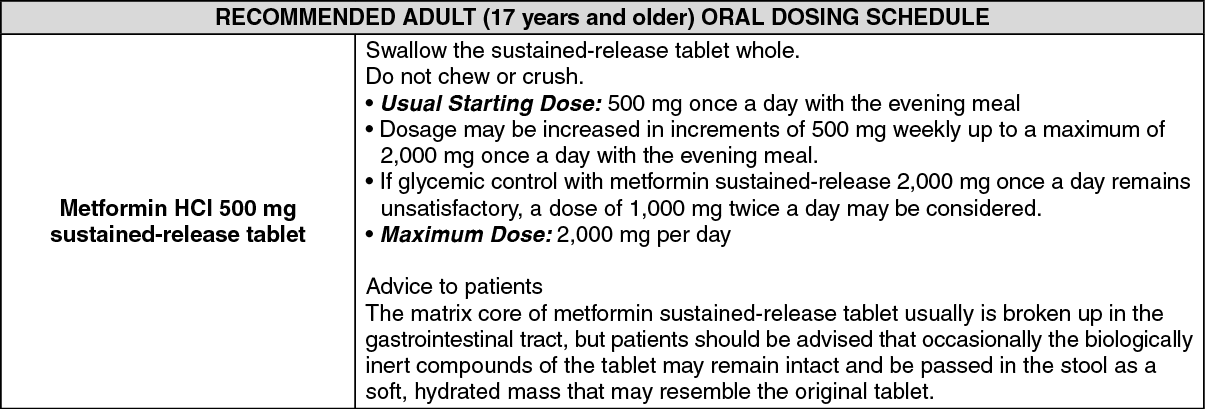
Sustained-release tablet: General Dosing Recommendations: There is usually no fixed dosage regimen with any antidiabetic agent for the management of hyperglycemia in patients with diabetes mellitus. Dosage of metformin HCl tablets must be individualized based on both effectiveness and tolerance while not exceeding the maximum recommended daily doses.
During treatment initiation and dose titration, fasting plasma glucose should be used to determine the therapeutic response to metformin HCl tablet and identify the minimum effective dose. Thereafter, glycosylated hemoglobin (HbA1c) should be measured at intervals of approximately three months. The therapeutic goal should be to decrease both fasting plasma glucose and glycosylated hemogloin levels to normal or near normal by using the lowest effective dose of metformin when used as monotherapy or in combination with other oral antidiabetic agents or insulin.
Monitoring of glycemic control through frequent measurements of fasting blood glucose and periodic testing of HbA1c will detect primary failure (i.e., inadequate lowering of blood glucose at the maximum recommended dose of medication), and secondary failure (i.e., loss of adequate blood glucose lowering response after an initial period of effectiveness).
It is recommended that metformin HCl be administered with meals to ensure optimum delivery of metformin to the systemic circulation and minimize gastric intolerance. Administration of metformin in the fed state has been shown to significantly increase the systemic delivery of metformin compared to the fasted state. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Sustained-release tablet: There were no cases of overdose reported in clinical studies. Symptoms of metformin overdose include extensions of the common adverse effects (e.g., epigastric discomfort, nausea, vomiting, diarrhea, drowsiness, weakness, dizziness, malaise, and headache).
Should these symptoms occur, lactic acidosis should be excluded. Metformin therapy should be discontinued and proper supportive therapy should be instituted.
Metformin ingestion of up to 50 g has been reported. Hypoglycemia was reported in 10% of cases, but no causal relationship with metformin has been established. Lactic acidosis has been reported in approximately 32% of metformin overdose cases. Metformin is dialyzable with a clearance of up to 170 mL/min under good hemodynamic conditions. Therefore, hemodialysis maybe useful for removal of accumulated drug from patients in whom metformin overdosage is suspected.
Sustained-release tablet: Hypersensitivity to metformin HCl or to any ingredient in the product.
Unstable and/or type 1 (insulin-dependent) diabetes mellitus.
History of lactic acidosis irrespective of precipitating factors.
Acute or chronic metabolic acidosis, including diabetic ketoacidosis, with or without coma. Treat diabetic ketoacidosis with insulin.
Severe renal impairment (eGFR <30mL/min/1.73 m2).
Acute conditions with the potential to alter renal function such as: Dehydration due to persistent or severe diarrhea, recurrent vomiting; Severe infection; Diagnostic examinations (e.g., intravenous urography, angiography) that would involve the use of iodinated contrast agents/media.
Acute or chronic disease which may cause tissue hypoxia such as: Cardiac or respiratory failure; Recent myocardial infarction; Shock.
Acute or chronic alcoholism.
Severe liver disease.
Pregnancy or breastfeeding.
Sustained-release tablet: Warning on Lactic Acidosis: Lactic acidosis is a rare, but serious (high mortality in the absence of prompt treatment), metabolic complication that can occur due to metformin accumulation. Reported cases of lactic acidosis in patients on metformin have occurred primarily in diabetic patients with significant renal failure. The incidence of lactic acidosis can be reduced by also assessing other associated risk factors such as poorly controlled diabetes, ketosis, prolonged fasting, excessive alcohol intake, hepatic insufficiency, and any condition associated with hypoxia.
Lactic acidosis is characterized by elevated blood lactate levels (>5 mmol/L), reduced blood pH, electrolyte disturbance with an increased anion gap, and an increased lactate/pyruvate ratio. When metformin is implicated as the cause of lactic acidosis, metformin plasma levels >5 mcg/mL are generally found.
Lactic acidosis is usually accompanied by nonspecific symptoms such as acidotic dyspnea, vomiting, abdominal pain with muscle cramps, and/or a general feeling of malaise with severe fatigue. Hypothermia followed by coma, hypotension, and resistant bradyarrhythmias may be seen with marked acidosis. Instruct patients to immediately alert their physicians if these symptoms occur. Serum electrolytes, ketones, blood glucose, and if indicated, blood pH, lactate levels, and even blood metformin levels may be useful.
Lactic acidosis is a medical emergency that must be treated in a hospital setting. In a patient with lactic acidosis who is taking metformin, the drug should be discontinued immediately and general supportive measures promptly instituted. Because metformin HCl is dialyzable, prompt hemodialysis is recommended to correct the acidosis and remove the accumulated metformin. Such management often results in prompt reversal of symptoms and recovery.
Do not use metformin in patients with congestive heart failure receiving drugs such as digoxin and furosemide because of the risk of hypoperfusion and hypoxemia which may lead to lactic acidosis.
Tablet: Age, hepatic and renal impairment are independent risk factors for hypoglycemia. Use with caution in patients with hepatic impairment, malnourished or debilitated conditions, or adrenal or pituitary insufficiency.
Use with caution in patients with renal impairment. Metformin is substantially excreted by the kidney. The risk of accumulation and lactic acidosis increases with the degree of impairment in renal function.
Alcohol intake may potentiate lactic acidosis.
Cardiovascular collapse (shock) from whatever cause, acute congestive heart failure, acute myocardial infarction and other conditions characterized by hypoxemia have been associated with lactic acidosis and may also cause prerenal azotemia. When such events occur in patients on metformin therapy, metformin should be promptly discontinued.
Use of concomitant medications that may affect renal function (ie, tubular secretion) may affect metformin disposition.
Suspend treatment for surgical procedures which restrict the intake of food and fluids; do not restart treatment until oral intake and renal function are normal.
Metformin may cause a decrease to subnormal levels of previously normal serum vitamin B12, without clinical manifestations. Measurement of hematologic parameters on an annual basis is advised in patients receiving metformin and any apparent abnormalities should be appropriately investigated and managed.
Intravascular contrast studies with iodinated materials can lead to acute alteration of renal function and have been associated with lactic acidosis in patients receiving metformin. Therefore, in patients in whom such study is planned, metformin HCl should be temporarily discontinued at the time of or prior to the procedure and reinstituted only after renal function has been re-evaluated and found to be normal.
Metformin should not be administered as a substitute for proper dietary regimen. It will not prevent the development of complications associated with diabetes mellitus.
Sustained-release tablet: Monitoring of Renal Function: Impaired renal function would increase the risk of metformin accumulation and lactic acidosis. Renal function should be assessed and verified as normal before initiation of metformin HCl therapy. Estimated glomerular filtration rate (eGFR) should be determined at least annually in all patients taking metformin. In patients at increased risk for the development of renal impairment (e.g., the elderly), renal function should be assessed more frequently.
Initiating metformin HCl therapy in patients with eGFR between 30 to 45 mL/min/1.73 m2 is not recommended. In patients taking metformin whose eGFR later falls below 45 mL/minute/1.73 m2, the benefits and risks of continuing treatment should be assessed. Discontinue metformin if the patient's eGFR later falls below 30 mL/minute/1.73 m2.
Medications which may affect renal function or result in significant hemodynamic change or interfere with the disposition of metformin (i.e., cationic drugs) should be used with caution since these drugs are eliminated by renal tubular secretion.
Macrovascular Outcomes: Macrovascular risk reduction with the use of metformin or any antidiabetic drug has not been established in clinical studies.
Radiologic Studies: Administration of parenteral iodinated contrast agents has led to an acute decrease in renal function and the occurrence of lactic acidosis in patients receiving metformin. Discontinue metformin at the time of, or prior to, an iodinated contrast imaging procedure in patients with an eGFR between 30 and 60 mL/minute/1.73 m2, history of liver disease, alcoholism, or heart failure; or in patients who will be administered intra-arterial iodinated contrast. Re-evaluate eGFR 48 hours after the imaging procedure, and restart metformin if renal function is stable.
Hypoxic States: Cardiovascular collapse (shock) from whatever cause, acute congestive heart failure, acute myocardial infarction and other conditions characterized by hypoxemia have been associated with lactic acidosis and may also cause prerenal azotemia. Promptly discontinue metformin when such events occur in patients on metformin HCl therapy.
Surgical Procedures: Temporarily discontinue metformin use in patients undergoing surgery associated with restricted food or fluid intake. Metformin therapy may be reinstituted when the patient's oral intake has resumed and renal function has been found normal.
Impaired Hepatic Function: Metformin HCl should generally be avoided in patients with clinical or laboratory evidence of hepatic disease since impaired hepatic function has been associated with lactic acidosis.
Alcohol: Combined use of alcohol and metformin may increase the risk of hypoglycemia and lactic acidosis since alcohol decreases lactate clearance and hepatic gluconeogenesis, and may increase insulin secretion. Excessive alcohol intake on an acute or chronic basis should be avoided in patients receiving metformin.
Vitamin B12 Levels: Evaluate hematologic parameters prior to initiation of metformin therapy and at least annually since decreases in serum vitamin B12 have been associated with metformin use.
Hypoglycemia: Hypoglycemia does not occur in patients receiving metformin alone under usual circumstances of use, but could occur when caloric intake is deficient, when strenuous exercise is not compensated by caloric supplementation, or during concomitant use with other glucose-lowering agents (such as sulfonylureas and insulin) or ethanol.
Elderly, debilitated or malnourished patients, and those with adrenal or pituitary insufficiency or alcohol intoxication are particularly susceptible to hypoglycemia. It may be difficult to recognize hypoglycemic states in the elderly, and in people who are taking beta-adrenergic blocking drugs.
Maintaining Adequate Glycemic Control during Periods of Stress: Temporary discontinuation of metformin and administration of insulin may be necessary in periods of stress such as fever, trauma, infection, or surgery to maintain adequate glucose control. Metformin may be reinstituted after the acute episode is resolved.
Effects on Ability to Drive and Use Machines: Patients should be warned about driving a vehicle or operating machinery under conditions where risk of hypoglycemia is present.
Use in Children: Sustained-release tablet: The safety and efficacy of metformin sustained-release tablet have not been established in these patients.
Use in the Elderly: Tablet: In elderly patients, renal function should be monitored regularly.
Sustained-release tablet: Aging is associated with reduced renal function and metformin is known to be substantially excreted in the kidney. The risk of serious adverse reactions to metformin is greater in patients with reduced/impaired renal function especially in the elderly. Care should be taken in dose selection and should be based on careful and regular monitoring of renal function. Generally, dose of elderly patients should not be titrated to the maximum dose. Metformin treatment should not be initiated in patients ≥80 years old unless creatinine clearance demonstrates that renal function is not reduced.
Tablet: Metformin should not be used by pregnant and breastfeeding mothers. Although metformin treatment has not been linked with adverse embryonic effects in pregnant women with diabetes, insulin rather than oral antihyperglycemic agents should be used to control hyperglycemia in pregnancy.
Sustained-release tablet: Pregnancy: Pregnancy Category B. Oral hypoglycemic agents (including metformin) are not recommended during pregnancy. Maintaining blood glucose levels as close to normal as possible is necessary during pregnancy since abnormal blood glucose levels are associated with a higher incidence of congenital abnormalities. Insulin is recommended during pregnancy.
Lactation: Metformin is excreted into human milk and should therefore not be used by breastfeeding mothers. The importance of metformin HCl to the mother should be considered when deciding whether to discontinue breastfeeding or discontinue metformin because the potential for hypoglycemia in breastfeeding infants may exist. Consider insulin therapy for adequate glycemic control if metformin HCl is discontinued.
Tablet: Diarrhea, lactic acidosis, anorexia, abdominal discomfort, nausea and metallic taste.
Impaired GI absorption of vitamin B12 and folic acid has been associated with long-term metformin therapy.
Individual case reports of megaloblastic anemia, pneumonitis with vasculitis with metformin have been reported.
Sustained-release tablet: Metformin may provoke or augment lactic acidosis particularly if it is present in high concentrations in the blood. Some of the symptoms of lactic acidosis may mimic certain adverse effects of metformin. Physicians should instruct their patients to recognize the onset of symptoms of lactic acidosis to avoid this adverse reaction.
The most frequent adverse effects reported with metformin include nausea, vomiting, diarrhea, abdominal pain and loss of appetite. These adverse effects occur during initiation of treatment and resolve spontaneously in most cases.
Blood and lymphatic system disorders: Decrease in serum vitamin B
12, megaloblastic anemia (rare); serum folic acid concentrations do not appear to decrease substantially in patients receiving metformin.
Metabolism and nutrition disorders: Hyperglycemia, hypoglycemia (may occur when metformin is given concomitantly with sulfonylureas and/or alcohol), lactic acidosis, weight decreased.
Nervous system disorders: Agitation, dizziness, headache, lightheadedness.
Cardiac disorders: Chest discomfort, palpitations.
Vascular disorders: Flushing, hypertension.
Respiratory, thoracic and mediastinal disorders: Dyspnea, flu syndrome, pneumonitis with vasculitis, rhinitis, upper respiratory infection.
Gastrointestinal disorders: Abdominal discomfort (e.g., bloating, abdominal cramps), abdominal distention, abnormal stools/loose stools, anorexia, constipation, dry mouth, dyspepsia/heartburn, epigastric discomfort, flatulence, gastric disorder, gastric ulcer, gastrointestinal disorder, indigestion, taste disturbance specifically metallic taste in the mouth.
Hepatobiliary disorders: Abnormal liver function tests, autoimmune hepatitis, cholestasis, hepatic injury, hepatitis.
Skin and subcutaneous tissue disorders: Erythema, nail disorder, pruritus, rash, skin lesion, urticaria.
Musculoskeletal and connective tissue disorders: Asthenia, chills, musculoskeletal pain, myalgia.
Renal and urinary disorders: Urinary tract infection.
General disorders and administration site conditions: Fatigue, increased sweating.
Tablet: Antidiabetic Agents: Acarbose reduced the bioavailability of metformin. In patients with type 2 diabetes mellitus, co-administration of glibenclamide with metformin showed variable decrease in the area under the blood concentration-time curve (AUC) and peak blood concentration of glibenclamide.
Diuretics: Thiazide diuretics can exacerbate diabetes mellitus resulting in increased requirements of oral antidiabetic agents, temporary loss of diabetic control or secondary failure to antidiabetic agent. Concomitant administration of furosemide and metformin increased the peak plasma and blood concentrations of metformin by approximately 22%, AUC of metformin by approximately 15%; peak plasma furosemide concentrations and AUC by approximately 31% and 12%, respectively. Half-life of furosemide was decreased by 32%.
Nifedipine: Concomitant administration of metformin and nifedipine in healthy individuals enhanced the absorption and increased the urinary excretion of metformin.
Drugs eliminated by renal tubular secretion (ie, amiloride, digoxin, morphine, procainamide, quinidine, quinine, ranitidine, triamterene, trimethoprim, vancomycin): May cause an increase in metformin peak plasma, whole blood concentrations and whole blood AUC.
Cimetidine: In single- and multiple-dose studies in healthy individuals, concomitant administration of cimetidine and metformin increased the peak plasma and whole blood concentrations of metformin by approximately 60-81% and the AUC of metformin by approximately 40-50%.
β-Adrenergic Blocking Agents: β-adrenergic blocking agents may impair glucose tolerance; increase the frequency and severity of hypoglycemia; block hypoglycemia-induced tachycardia and increase hypoglycemic sweating; delay the rate of recovery of blood glucose concentration following drug-induced hypoglycemia; alter hemodynamic response and impair peripheral circulation.
Alcohol: Combined use of alcohol and metformin increases the risk of hypoglycemia and lactic acidosis.
Angiotensin-Converting Enzyme (ACE) Inhibitors: ACE inhibitors (eg, captopril, enalapril) reduce fasting blood glucose concentration in nondiabetic individuals and increase insulin sensitivity.
Others: Drugs that cause hyperglycemia and may exacerbate glycemic control in patients with diabetes mellitus include corticosteroids, oral contraceptives, sympathomimetics, phenothiazines, niacin, calcium-channel blocking agents and isoniazid.
Sustained-release tablet: Cationic Drugs: Cationic drugs such as amiloride, digoxin, morphine, procainamide, quinidine, quinine, ranitidine, triamterene, trimethoprim, and vancomycin that are eliminated by renal tubular secretion, theoretically may cause an increase in metformin peak plasma concentrations, whole blood concentrations and whole blood AUC by competing with metformin for common renal tubular transport systems. Concomitant administration of metformin and cimetidine has been observed to result in reduced urinary metformin excretion and increased plasma metformin concentrations.
Other Antidiabetic Agents: Hypoglycemia may occur when metformin is used concomitantly with other antidiabetic agents such as sulfonylureas, meglitinides, glitazones, or insulin.
Diuretics: Thiazide diuretics may exacerbate diabetes mellitus and may result in increased requirements of oral antidiabetic agents, metformin included. Temporary loss of diabetic control or secondary failure to the antidiabetic agent may also occur. Potassium-sparing diuretics, which are less diabetogenic, may be considered as a substitute.
Furosemide may increase metformin plasma and blood concentrations and blood AUC without significantly affecting metformin renal clearance.
Nifedipine: Nifedipine increases the absorption, Cmax and AUC of metformin, and increases metformin excretion in the urine. Metformin has minimal effects on nifedipine pharmacokinetics.
β-Adrenergic Blocking Agents: β-adrenergic blocking agents (e.g., propranolol, nadolol) may impair glucose tolerance and mask the true frequency or severity of hypoglycemia, block hypoglycemia-induced tachycardia but not hypoglycemic sweating, delay the rate of recovery of blood glucose concentration following drug-induced hypoglycemia, and impair peripheral circulation. Use these drugs with caution in patients with type 2 diabetes.
Protein-Bound Drugs: Interaction of metformin and highly protein-bound drugs (e.g., salicylates, sulfonamides, chloramphenicol, probenecid) is unlikely because metformin is negligibly bound to plasma proteins.
Angiotensin-Converting Enzyme (ACE) Inhibitors: ACE inhibitors (e.g., captopril, enalapril) may reduce fasting blood glucose concentrations. These drugs have also been associated with unexplained hypoglycemia in diabetic patients. Caution should be exercised when administering metformin together with ACE inhibitors to prevent severe hypoglycemia.
Alcohol: There is an increased risk of hypoglycemia and lactic acidosis when alcohol and metformin are used concomitantly since alcohol decreases lactate clearance and hepatic gluconeogenesis, and may increase insulin secretion. Acute or chronic intake of alcohol should be avoided in patients receiving metformin therapy.
Clomifene: Ovulatory response may be increased when clomifene and metformin are used concomitantly in premenopausal patients with polycystic ovary syndrome.
Anticoagulants: Metformin may affect the pharmacokinetic properties of coumarin anticoagulants when administered concomitantly. An increase in prothrombin time may occur upon cessation of metformin therapy, with an increased risk of hemorrhage. Patients receiving phenprocoumon or other vitamin K anticoagulants should be carefully monitored.
Iodinated Contrast Media: Intravascular administration of iodinated contrast media may lead to renal failure, resulting in metformin accumulation with the risk of lactic acidosis. Metformin should be discontinued prior to, or at the time of the procedure, and withheld for 48 hours afterwards. Metformin may be reinstituted only after renal function has been re-evaluated and found to be normal.
Glyburide: Concomitant administration of metformin and glyburide produced no changes in metformin pharmacokinetics and pharmacodynamics. Decreases in Cmax, blood AUC of glyburide were observed, but were highly variable. The clinical significance of this finding was unclear.
Others: Drugs that may cause hyperglycemia and may exacerbate loss of glycemic control in patients with diabetes include thiazides and other diuretics, corticosteroids, phenothiazines, thyroid products, estrogens, oral contraceptives, phenytoin, nicotinic acid, sympathomimetics, calcium channel blocking drugs, and isoniazid. Close monitoring of glycemic control and metformin dose adjustments are recommended when such drugs are administered or withdrawn in patients.
The pharmacokinetics of metformin and propranolol, and metformin and ibuprofen were not affected when coadministered in single-dose interaction studies in healthy volunteers.
Store at temperatures not exceeding 30°C.
A10BA02 - metformin ; Belongs to the class of biguanides. Used in the treatment of diabetes.
RiteMED Metformin HCl SR tab 500 mg
100's (P6.25/SR tab, P625/box)
RiteMED Metformin HCl tab 500 mg
100's (P3.5/tab, P350/box)
RiteMED Metformin HCl tab 850 mg
100's (P7.5/tab, P750/box)


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out