Pharmacology: Mechanism of action: Octreotide is a synthetic octapeptide derivative of naturally occurring somatostatin with similar pharmacological effects, but with a considerably prolonged duration of action. It inhibits pathologically increased secretion of growth hormone (GH) and of peptides and serotonin produced within the gastro-entero-pancreatic (GEP) endocrine system.
In animals, octreotide is a more potent inhibitor of GH, glucagon and insulin release than somatostatin, with greater selectivity for GH and glucagon suppression.
In healthy subjects octreotide, like somatostatin, has been shown to inhibit: release of GH stimulated by arginine, exercise and insulin-induced hypoglycemia; post-prandial release of insulin, glucagon, gastrin, other peptides of the GEP system, and arginine-stimulated release of insulin and glucagon; thyrotropin-releasing hormone (TRH)-stimulated release of thyroid-stimulating hormone (TSH).
Pharmacodynamics: Unlike somatostatin, octreotide inhibits GH preferentially over insulin and its administration is not followed by rebound hypersecretion of hormones (i.e. GH in patients with acromegaly).
In patients with acromegaly, Sandostatin LAR, a galenical formulation of octreotide suitable for repeated administration at intervals of 4 weeks, delivers consistent and therapeutic octreotide serum concentrations thus consistently lowering GH and normalizing IGF 1 serum concentrations in the majority of patients. In most patients, Sandostatin LAR markedly reduces the clinical symptoms of the disease, such as headache, perspiration, paresthesia, fatigue, osteoarthralgia and carpal tunnel syndrome. In previously untreated acromegaly patients with GH-secreting pituitary adenoma, Sandostatin LAR treatment resulted in a tumor volume reduction of > 20% in a significant proportion (50%) of patients.
For patients with functional tumors of the gastro-entero-pancreatic endocrine system, treatment with Sandostatin LAR provides continuous control of symptoms related to the underlying disease. The effect of octreotide in different types of gastro-entero-pancreatic tumors are as follows:
Carcinoid tumors: Administration of octreotide may result in improvement of symptoms, particularly of flushing and diarrhea. In many cases, this is accompanied by a fall in plasma serotonin and reduced urinary excretion of 5 hydroxyindole acetic acid.
VIPomas: The biochemical characteristic of these tumors is overproduction of vasoactive intestinal peptide (VIP). In most cases, administration of octreotide results in alleviation of the severe secretory diarrhea typical of the condition, with consequent improvement in quality of life. This is accompanied by an improvement in associated electrolyte abnormalities, e.g. hypokalemia, enabling enteral and parenteral fluid and electrolyte supplementation to be withdrawn. In some patients, computer tomography scanning suggests a slowing or arrest of progression of the tumor, or even tumor shrinkage, particularly of hepatic metastases. Clinical improvement is usually accompanied by a reduction in plasma VIP levels, which may fall into the normal reference range.
Glucagonomas: Administration of octreotide results in most cases in substantial improvement of the necrolytic migratory rash which is characteristic of the condition. The effect of octreotide on the state of mild diabetes mellitus which frequently occurs is not marked and, in general, does not result in a reduction of requirements for insulin or oral hypoglycemic agents. Octreotide produces improvement of diarrhea, and hence weight gain, in those patients affected. Although administration of octreotide often leads to an immediate reduction in plasma glucagon levels, this decrease is generally not maintained over a prolonged period of administration, despite continued symptomatic improvement.
Gastrinomas/Zollinger-Ellison syndrome: Although therapy with proton pump inhibitors or H
2-receptor blocking agents controls the recurrent peptic ulceration which results from chronic gastrin-stimulated hypersecretion of gastric acid, such control may be incomplete. Diarrhea may also be a prominent symptom not alleviated in all patients by this therapy. Octreotide alone or in conjunction with proton pump inhibitors or H
2-receptor antagonists may reduce gastric acid hypersecretion and improve symptoms, including diarrhea. Other symptoms possibly due to peptide production by the tumor, e.g. flushing, may also be relieved. Plasma gastrin levels fall in some patients.
Insulinomas: Administration of octreotide produces a fall in circulating immunoreactive insulin. In patients with operable tumors, octreotide may help to restore and maintain normoglycemia pre-operatively. In patients with inoperative benign or malignant tumors, glycemic control may be improved even without concomitant sustained reduction in circulating insulin levels.
GRFomas: These rare tumors are characterized by production of GH releasing factor (GRF) alone or in conjunction with other active peptides. Octreotide produces improvement in the features and symptoms of the resulting acromegaly. This is probably due to inhibition of GRF and GH secretion, and a reduction in pituitary enlargement may follow.
Clinical Studies: Acromegaly: Two dose finding studies (SMSC 201-E-01 and SMSC 202-E-00) were initially carried out with Sandostatin LAR in acromegalic patients. These studies were prospective single dose, double-blind, randomized, multi-centre studies designed to assess the following doses of Sandostatin LAR injected intramuscularly: 10, 20 and the 30 mg.
Patients who showed GH suppression on t.i.d. Sandostatin s.c. pre-treatment were selected for these studies. Out of the 93 patients included, 78 were "responders" (mean 12-hour GH serum concentrations below 5 μg/L during pre-treatment with Sandostatin s.c.) and 15 patients were "partial responders" to Sandostatin s.c. (GH mean concentrations suppressed to approximately 50% of pretreatment levels but not to below 5 μg/L).
The primary efficacy parameter was the mean 12-hour GH serum concentrations. The results of the double-blind studies SMSC 201-E-01 and SMSC 202-E-00 showed that the 20 and 30 mg doses of Sandostatin LAR are able to suppress GH levels below 5μg/L from day 14 until day 42. The i.m. injection was well tolerated locally and the adverse events analysis reflected the known gastro-intestinal reactions to octreotide.
To document the long-term tolerability, safety and efficacy of Sandostatin LAR in acromegalic patients, three prospective open-label extensions for each of the two double-blind studies were completed (SMSC 201-E-02/-03/-04 and SMSC 202-E-01/-02/-03).
All patients that had participated to studies SMSC 201-E-01 and SMSC 202-E-00 and had well tolerated the study drug were offered to continue treatment with additional injections of Sandostatin LAR in the open label extension studies. A total of 101 patients entered these studies and 87 completed all extensions, thus receiving 28 injections of Sandostatin LAR.
Investigators were allowed to titrate patients to their optimal therapeutic response (using 10, 20, 30 or exceptionally 40 mg doses). An interval of 28 days between injections was considered optimal for providing consistent steady-state concentrations of octreotide, based on pharmacokinetic simulation of single dose profiles and considering the linearity of pharmacokinetics of octreotide. The primary efficacy endpoint in the extension studies was the 8-hours GH serum concentrations.
These extension studies demonstrated that long-term treatment of acromegalic patients with Sandostatin LAR administered at doses of 10-30 mg i.m. in patients known to be responsive to Sandostatin s.c. results in a sustained suppression of mean 8-hour GH levels throughout the dosing interval. These effects were accompanied by a marked reduction in IGF-I concentrations and a persistent regression of the symptoms of acromegaly.
Long-term systemic tolerability of Sandostatin LAR was good, the pattern, severity and duration of adverse events was similar to those historically reported for the s.c. treatment with Sandostatin and for short-term treatment with Sandostatin LAR.
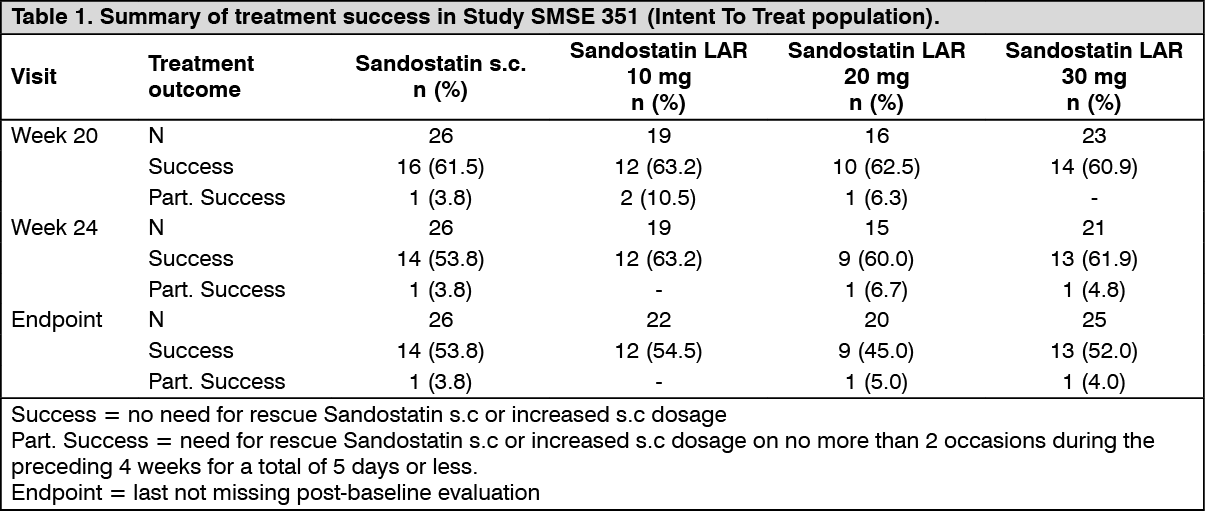
GEP tumours: The clinical trial program for Sandostatin LAR in GEP tumors consisted of one controlled clinical study (SMSE 351) which was carried out in patients with malignant carcinoid syndrome symptomatically controlled by Sandostatin s.c..
Study SMSE351 was a randomized, double-blind, multicenter prospective study of efficacy, safety and tolerability of multiple dose levels of Sandostatin LAR (10, 20 and 30 mg doses) administered at 4-week intervals versus open-label subcutaneous Sandostatin. Ninety-three patients were enrolled and 80 completed the study.
Assessment of treatment success, partial treatment success or treatment failure was based on the degree and duration of suppression of carcinoid symptoms as indicated by the need for rescue therapy with Sandostatin in patients randomized to one of the Sandostatin LAR groups, or by the need for an increase in dosage in patients randomized to the Sandostatin group, at the end of Week 20 and Week 24.
A level of efficacy comparable to that achieved with Sandostatin s.c. was observed with Sandostatin LAR after the 5
th and 6
th injections at Weeks 20 and 24 respectively, and at endpoint (see Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The data recorded in Study SMSE 351 showed that Sandostatin LAR is as effective and as well tolerated as Sandostatin s.c. injections in the treatment of patients with carcinoid symptoms.
Advanced Neuroendocrine Tumors of the midgut or unknown primary tumor location: A Phase III, randomized, double-blind, placebo-controlled study (PROMID) demonstrated that Sandostatin LAR inhibits tumor growth in patients with advanced Neuroendocrine Tumors of the midgut.
85 patients were randomized to receive Sandostatin LAR 30 mg every 4 weeks (n = 42) or placebo (n = 43) for 18 months, or until tumor progression or death.
Main inclusion criteria were: treatment naïve; histologically confirmed; locally inoperable or metastatic well-differentiated; functionally active or inactive neuroendocrine tumors/carcinomas; with primary tumor located in the midgut or unknown origin believed to be of midgut origin if a primary within the pancreas, chest, or elsewhere was excluded.
The primary endpoint was time to tumor progression or tumor-related death (TTP) based on central radiological review using WHO criteria.
Sandostatin LAR was superior to placebo for TTP with 26 and 38 progressions or tumor-related deaths in the Sandostatin LAR and placebo groups, respectively (HR = 0.36; 95% CI, 0.21 to 0.61; p-value =.0001). (See Figure.)
Median time to tumor progression was 14.3 months (95% CI, 11.0 to 28.8 months) in the Sandostatin LAR group and 5.9 months (95% CI, 3.7 to 9.2 months) in the placebo group. (See Figure.)
Click on icon to see table/diagram/image
Treatment effect was similar in patients with functioning (HR = 0.41; 95% CI, 0.18 to 0.92) and non-functioning tumors (HR = 0.32; 95% CI, 0.15 to 0.66).
Based on the significant clinical benefit of Sandostatin LAR observed in the pre-planned interim analysis the recruitment was stopped.
After an additional 4.5 years of follow-up, the hazard ratio of Sandostatin LAR versus placebo for overall survival was 0.86 (95% CI: 0.46, 1.60) favoring Sandostatin LAR. The overall survival results should be interpreted with caution due to the low number of events and the large number of patients in the placebo group who received follow-up therapy with somatostatin analogues.
The safety of Sandostatin LAR in this trial was consistent with its established safety profile.
Pharmacokinetics: After single i.m. injections of Sandostatin LAR, the serum octreotide concentration reaches a transient initial peak within 1 hour after administration, followed by a progressive decrease to a low undetectable octreotide level within 24 hours. After this initial peak on day 1, octreotide remains at sub-therapeutic levels in the majority of the patients for the following 7 days. Thereafter, octreotide concentrations increase again, and reach plateau concentrations around day 14 and remain relatively constant during the following 3 to 4 weeks. The peak level during day 1 is lower than levels during the plateau phase and no more than 0.5% of the total drug release occurs during day 1. After about day 42, the octreotide concentration decreases slowly, concomitant with the terminal degradation phase of the polymer matrix of the dosage form.
In patients with acromegaly, plateau octreotide concentrations after single doses of 10 mg, 20 mg and 30 mg Sandostatin LAR amount to 358 ng/L, 926 ng/L, and 1,710 ng/L, respectively. Steady-state octreotide serum concentrations, reached after 3 injections at 4 week intervals, are higher by a factor of approximately 1.6 to 1.8 and amount to 1,557 ng/L and 2,384 ng/L after multiple injections of 20 mg and 30 mg Sandostatin LAR, respectively.
In patients with carcinoid tumors, the mean (and median) steady-state serum concentrations of octreotide after multiple injections of 10 mg, 20 mg and 30 mg of Sandostatin LAR given at 4 week intervals also increased linearly with dose and were 1,231 (894) ng/L, 2,620 (2,270) ng/L and 3,928 (3,010) ng/L, respectively.
No accumulation of octreotide beyond that expected from overlapping release profiles occurred over a duration of up to 28 monthly injections of Sandostatin LAR.
The pharmacokinetic profile of octreotide after injection of Sandostatin LAR reflects the release profile from the polymer matrix and its biodegradation. Once released into the systemic circulation, octreotide distributes according to its known pharmacokinetic properties, as described for s.c. administration. The volume of distribution of octreotide at steady-state is 0.27 L/kg and the total body clearance is 160 mL/min. Plasma protein binding amounts to 65% and essentially no drug is bound to blood cells.
Toxicology: Non-Clinical Safety Data: Repeat dose toxicity: In two repeat dose studies performed in rats by i.m. injection of 2.5 mg Sandostatin LAR in 50 mg microspheres every 4 weeks for 21/24 weeks, no drug-related necropsy findings were observed. The only histopathological findings considered to be of significance were at the injection site in treated and control animals, where the microspheres had provoked a reversible granulomatous myositis.
Genotoxicity: Octreotide and/or its metabolites were devoid of mutagenic potential when investigated
in vitro in validated bacterial and mammalian cell test systems. In one study, an increased frequency of chromosomal changes were observed in V79 Chinese hamster cells, albeit at high and cytotoxic concentrations only. Chromosomal aberrations were however not increased in human lymphocytes incubated with octreotide acetate.
In vivo, no clastogenic activity was observed in the bone marrow of mice treated with octreotide i.v. (micronucleus test) and no evidence of genotoxicity was obtained in male mice using a DNA repair assay on sperm heads. The microspheres were devoid of mutagenic potential when tested in standard assays for genotoxicity .
Carcinogenicity/chronic toxicity: In studies in rats in which s.c. Sandostatin at daily doses up to 1.25 mg/kg body weight were administered, fibrosarcomas were observed, predominantly in a number of male animals, at the s.c. injection site after 52, 104 and 113/116 weeks. Local tumors occurred also in the control rats, however development of these tumors was attributed to disordered fibroplasia produced by sustained irritant effects at the injection sites, enhanced by the acidic lactic acid/mannitol vehicle. This non-specific tissue reaction appeared to be particular to rats. Neoplastic lesions were observed neither in mice receiving daily s.c. injections of Sandostatin at doses up to 2 mg/kg for up to 99 weeks, nor in dogs which were treated with daily s.c. doses of the drug for 52 weeks.
The 116 week carcinogenicity study in rats with s.c. Sandostatin also revealed uterine endometrial adenocarcinomas, their incidence reaching statistical significance at the highest s.c. dose level of 1.25 mg/kg per day. The finding was associated with an increased incidence of endometritis, a decreased number of ovarian corpora lutea, a reduction in mammary adenomas and the presence of uterine glandular and luminal dilation, suggesting a state of hormonal imbalance. The available information clearly indicates that the findings of endocrine-mediated tumors in rats are species-specific and are not relevant for the use of the drug in humans.
Reproduction toxicity: Reproduction studies have been performed with Sandostatin in rats and rabbits at parenteral doses of up to 1 mg/kg body weight per day. Some retardation of the physiological growth was noted in the offspring of rats which was transient and most likely attributable to GH inhibition brought about by excessive pharmacodynamic activity. There was no evidence of teratogenic, embryo/fetal or other reproduction effects due to octreotide.
The microspheres were devoid of reproductive toxicological effects when tested in standard studies for reproductive toxicity in rats and rabbits.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image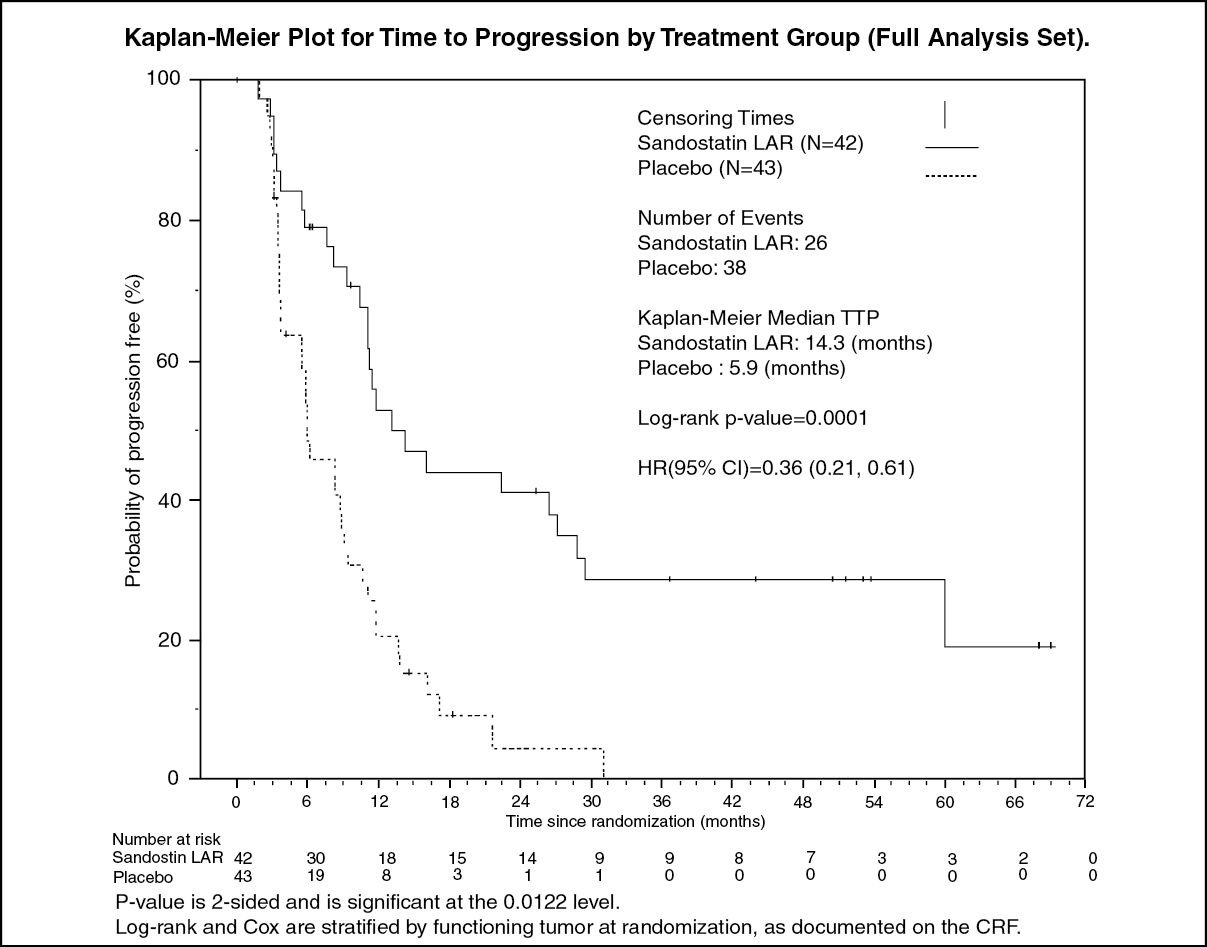 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image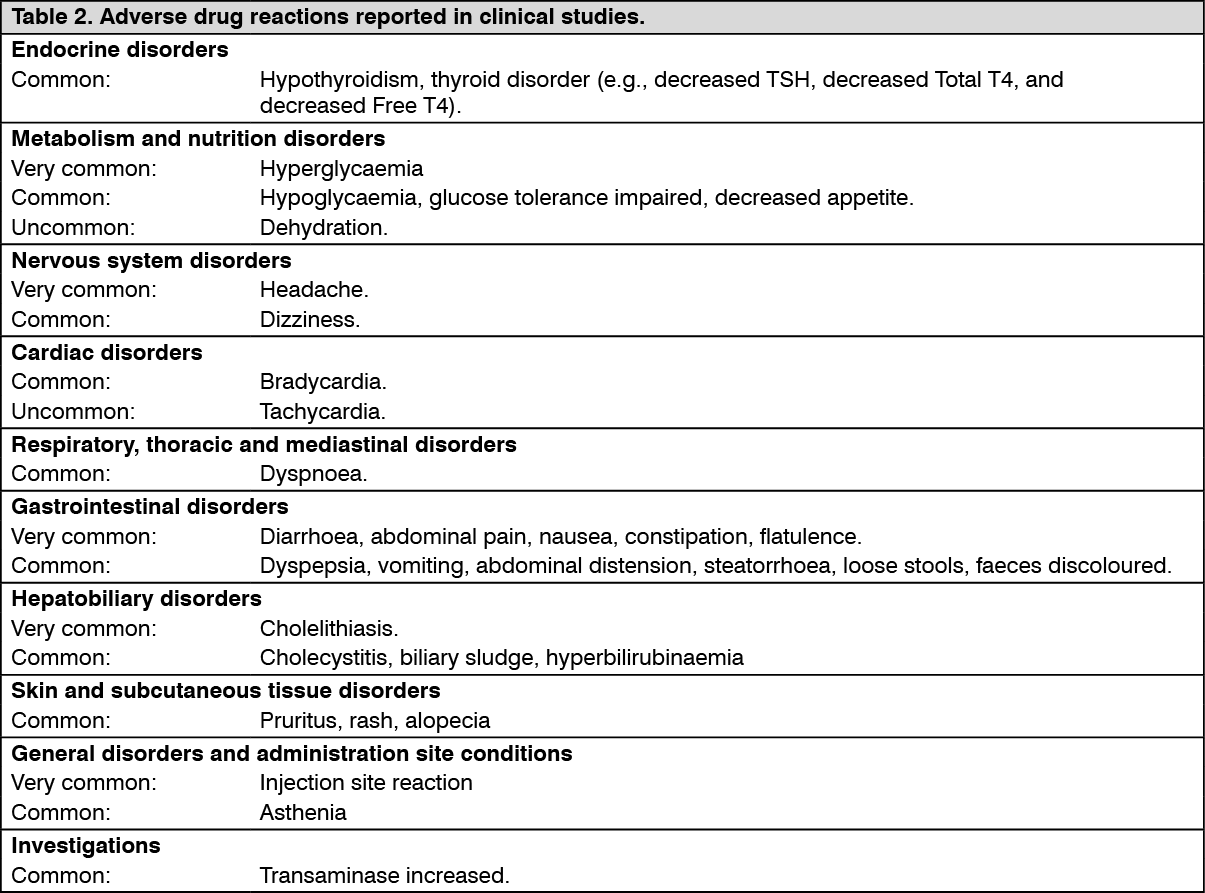 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out