Adult patients with newly-diagnosed glioblastoma multiforme: TEMOZOLOMIDE (TEMOVEX) hard capsules is administered in combination with focal radiotherapy (concomitant phase) followed by up to 6 cycles of temozolomide (TMZ) monotherapy (monotherapy phase).
Concomitant phase: TMZ is administered orally at a dose of 75 mg/m
2 daily for 42 days concomitant with focal radiotherapy (60 Gy administered in 30 fractions). No dose reductions are recommended, but delay or discontinuation of TMZ administration should be decided weekly according to haematological and non-haematological toxicity criteria. TMZ administration can be continued throughout the 42 day concomitant period (up to 49 days) if all of the following conditions are met: absolute neutrophil count (ANC) ≥1.5 x 10; thrombocyte count ≥100 x 10; common toxicity criteria (CTC) non-haematological toxicity ≤Grade 1 (except for alopecia, nausea and vomiting).
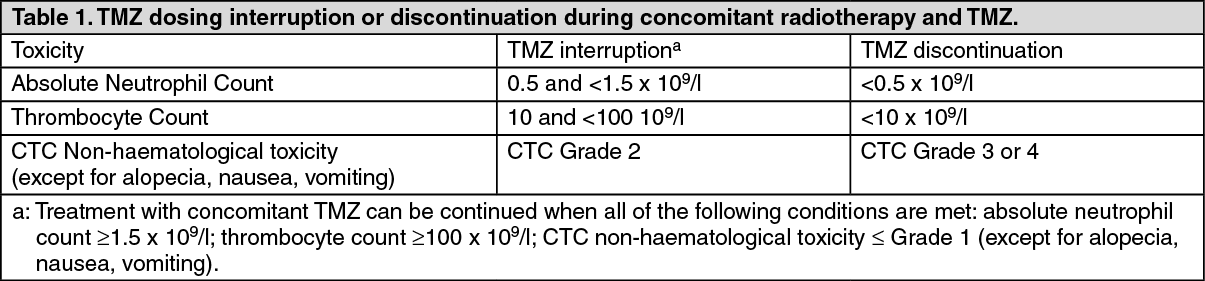
During treatment a complete blood count should be obtained weekly. TMZ administration should be temporarily interrupted or permanently discontinued during the concomitant phase according to the haematological and non-haematological toxicity criteria as noted in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Monotherapy phase:
Click on icon to see table/diagram/image
Monotherapy phase: Four weeks after completing the TMZ + RT concomitant phase, TMZ is administered for up to 6 cycles of monotherapy treatment. Dose in Cycle 1 (monotherapy) is 150 mg/m
2 once daily for 5 days followed by 23 days without treatment. At the start of Cycle 2, the dose is escalated to 200 mg/m
2 if the CTC nonhaematological toxicity for Cycle 1 is Grade ≤2 (except for alopecia, nausea and vomiting), absolute neutrophil count (ANC) is ≥1.5 x 10
9/l, and the thrombocyte count is ≥100 x 10
9/l. If the dose was not escalated at Cycle 2, escalation should not be done in subsequent cycles. Once escalated, the dose remains at 200 mg/m
2 per day for the first 5 days of each subsequent cycle except if toxicity occurs. Dose reductions and discontinuations during the monotherapy phase should be applied according to Tables 2 and 3. (See Table 2.)
Click on icon to see table/diagram/image
During treatment a complete blood count should be obtained on Day 22 (21 days after the first dose of TMZ). The dose should be reduced or administration discontinued according to Table 3 (see Table 3).
Click on icon to see table/diagram/image
Adult and paediatric patients 3 years of age or older with recurrent or progressive malignant glioma: A treatment cycle comprises 28 days. In patients previously untreated with chemotherapy, TMZ is administered orally at a dose of 200 mg/m
2 once daily for the first 5 days followed by a 23 day treatment interruption (total of 28 days). In patients previously treated with chemotherapy, the initial dose is 150 mg/m
2 once daily, to be increased in the second cycle to 200 mg/m
2 once daily, for 5 days if there is no haematological toxicity (see Adverse Reactions).
If vomiting occurs after the dose is administered, a second dose should not be administered that day.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image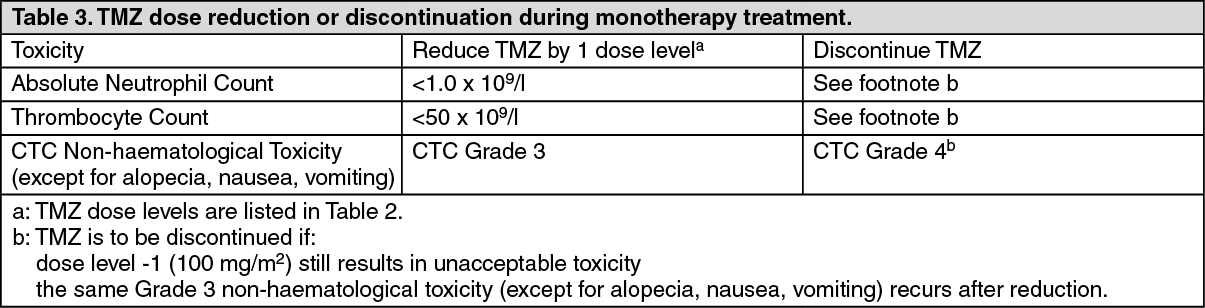 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out