Pharmacology: Pharmacodynamics: Azithromycin monohydrate (Zenith) is an azalide, derived from the macrolide class of antibiotics. The mode of action of Azithromycin monohydrate (Zenith)is inhibition of protein synthesis in bacteria by binding to the 50s ribosomal subunit and preventing translocation of peptides. Azithromycin monohydrate 9Zenith) is usually bacteriostatic. However, in high concentrations, azithromycin may be bactericidal against selected microorganisms. Azithromycin monohydrate (Zenith) is active against many gram-positive and gram-negative aerobic and anaerobic bacteria and bacterial pathogens such as
Mycobacterium avium complex,
Mycoplasma spp,
Borrelia burgdorferi,
Chlamydia spp and
Campylobacter spp. In addition, Azithromycin monohydrate (Zenith) has activity against protozoan microorganisms such as
Toxoplasma gondii.
Breakpoints: According to the (CLSI) Clinical and Laboratory Standards Institute in 2001, the following breakpoints have been defined for azithromycin: 2 μg/mL susceptible; 4 μg/mL intermediate; ≥8 μg/mL resistant.
Haemophilus spp: ≤4 μg/mL susceptible.
Streptococcus pneumoniae and
Streptococcus pyogenes: ≤0.5 μg/mL susceptible; 1 μg/mL intermediate; ≥2 μg/mL resistant.
Note that national breakpoints may differ from those recommended by CLSI. There are currently no recommended CLSI breakpoints for Enterobacteriaceae,
Neisseria gonorrhoeae,
Moraxella catarrhalis and
Mycobacterium avium complex.
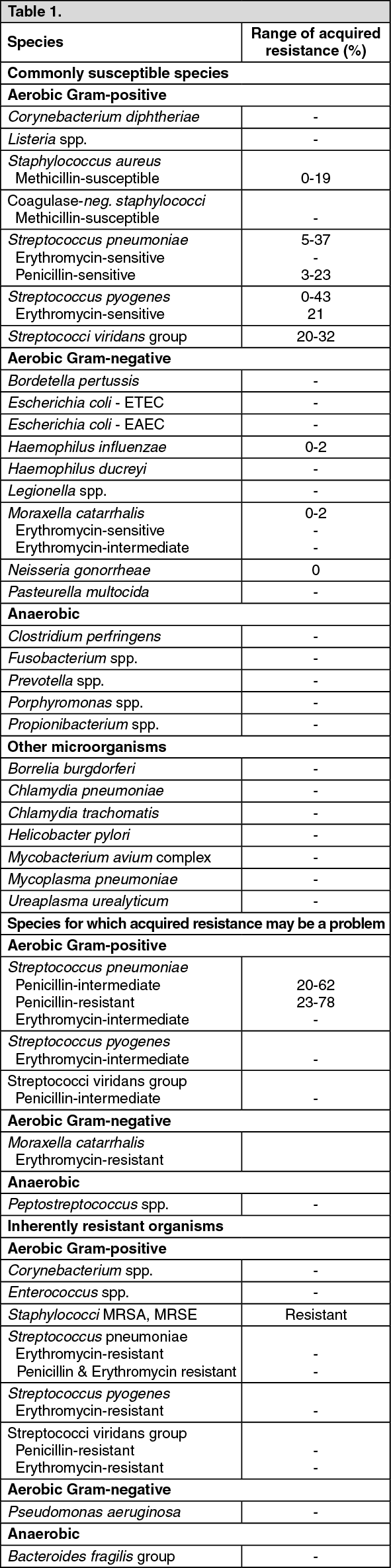
Susceptibility: The prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent in at least some types of infections is questionable. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Other Information: The diagnostic procedures available in vitro at this moment to determine the susceptibility of
Mycobacterium avium complex (MAC) organisms are not generally accepted and validated.
Streptococci and staphylococci that are resistant to erythromycin are also resistant to Azithromycin monohydrate (Zenith). Cross-resistance to
Mycobacterium avium complex organisms occurs between clarithromycin and azithromycin.
Pharmacokinetics: Absorption: After oral administration, the bioavailability of Azithromycin monohydrate (Zenith) is approximately 37%. Peak plasma levels are reached after 2-3 hours (C
max after a single dose of 500 mg orally was approximately 0.4 mg/L).
Distribution: Kinetic studies have shown markedly higher Azithromycin monohydrate (Zenith) levels in tissue than in plasma (up to 50 times the maximum observed concentration in plasma) indicating that the active substance is heavily tissue bound (steady-state distribution volume of approximately 31 L/kg). Concentrations in target tissues eg, lung, tonsil, and prostate exceed the MIC
90 so for likely pathogens after a single dose of 500 mg.
In experimental in vitro and in vivo studies, Azithromycin monohydrate (Zenith) accumulates in the phagocytes, freeing is stimulated by active phagocytosis. In animal studies, this process appeared to contribute to the accumulation of Azithromycin monohydrate (Zenith) in the tissue.
In serum the protein binding of Azithromycin monohydrate (Zenith) is variable and depending on the serum concentration varies from 50% in 0.05 mg/L to 12% in 0.5 mg/L.
Excretion: Plasma terminal elimination half-life closely reflects the tissue depletion half-life of 2 to 4 days. About 12% of an IV administered dose is excreted in the urine unchanged over a period of 3 days; the majority in the first 24 hours. Biliary excretion of Azithromycin monohydrate (Zenith), predominantly in unchanged form, is a major route of elimination.
The identified metabolites (formed by N- and O-demethylizing, by hydroxylizing of the desosamine and aglycone rings, and by the splitting of the cladinose conjugate) are microbiologically inactive.
After a 5 day treatment, slightly higher (29%) AUC values were seen in the elderly volunteers (>65 years) compared to the younger volunteers (<45 years). However these differences are not regarded as clinically relevant; therefore a dose adjustment is not recommended.
Special Populations: Renal insufficiency: Following a single oral dose of azithromycin 1 g, mean C
max and AUC
0-120 increased by 5.1% and 4.2%, respectively, in subjects with mild to moderate renal impairment (glomerular filtration rate of 10-80 mL/min) compared with normal renal function (GFR >80 mL/min). In subjects with severe renal impairment, the mean C
max and AUC
0-120 increased 61% and 35%, respectively compared to normal.
Hepatic insufficiency: In patients with mild to moderate hepatic impairment, there is no evidence of a marked change in serum pharmacokinetics of azithromycin monohydrate compared to normal hepatic function. In these patients, urinary recovery of Azithromycin monohydrate (Zenith) appears to increase perhaps to compensate for reduced hepatic clearance.
Elderly: The pharmacokinetics of azithromycin in elderly men was similar to that of young adults; however, in elderly women, although higher peak concentrations (increased by 30-50%) were observed, no significant accumulation occurred.
Infants, toddlers, children and adolescents: Pharmacokinetics have been studied in children 4 months - 15 years taking capsules, granules or suspension. At 10 mg/kg on day 1 followed by 5 mg/kg on days 2-5, the C
max achieved is slightly lower than adults with 224 μg/L in children 0.6-5 years and after 3 days dosing and 383 μg/L in children 6-15 years. The t
½ of 36 hours in the older children was within the expected range for adults.
Toxicology: Preclinical Safety Data: In high-dose animal studies, giving active substance concentrations 40 fold higher than those expected in clinical practice, azithromycin has been noted to cause reversible phospholipidosis, generally without discernible toxicological consequences. There is no evidence that this is of relevance to the normal use of Azithromycin monohydrate (Zenith) in humans.
Carcinogenic potential: Long-term studies in animals have not been performed to evaluate carcinogenic potential.
Mutagenic potential: Azithromycin monohydrate (Zenith) has shown no mutagenic potential in standard laboratory tests: mouse lymphoma assay, human lymphocyte clastogenic assay and mouse bone marrow clastogenic assay.
Reproductive Toxicity: No teratogenic effects were observed in animal studies of embryotoxicity in mice and rats. In rats, azithromycin dosages of 100 and 200 mg/kg body weight/day led to mild retardations in fetal ossification and in maternal weight gain. In peri-/postnatal studies in rats, mild retardations following treatment with ≥50 mg/kg/day azithromycin were observed.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out