Pharmacology: Zocef: Suspension: Mechanism of Action: Like other beta-lactam drugs, cefuroxime exerts antibacterial activity by binding to and inhibiting the action of certain bacterial cell wall synthetic enzymes namely the penicillin-binding proteins. This results in the interruption of cell wall (peptidoglycan) biosynthesis which leads to bacterial cell lysis and death.
Mechanisms of resistance: Bacterial resistance to cefuroxime may be due to one or more of the following mechanisms: Hydrolysis by beta-lactamases; cefuroxime may be efficiently hydrolysed by certain extended-spectrum beta-lactamases (ESBLs) and by the chromosomally encoded (AmpC) enzyme that may be induced or stably depressed in certain aerobic gram-negative bacterial species; Reduced affinity of penicillin-binding proteins for cefuroxime; Outer membrane impermeability, which restricts access of cefuroxime to penicillin-binding proteins in gram-negative organisms; Drug efflux pumps.
Breakpoints: The following clinical MIC breakpoints for bacteria have been defined for cefuroxime according to EUCAST: Enterobacteriaceae: :≤8 mg/L for susceptible, >8 mg/L for resistant;
S. pneumoniae: ≤0.5 mg/L for susceptible, >1 mg/L for resistant;
Streptococcus spp.: ≤0.5 mg/L for susceptible, >0.5 mg/L for resistant;
H. influenzae and
M. catarrhalis: ≤1 mg/L for susceptible, >2 mg/L for resistant; Non-species related breakpoints: ≤4 mg/L for susceptible, >8 mg/L for resistant.
Susceptibility: The prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence is such that the utility of the agent in at least some types of infections are questionable.
Zocef Hospi: Mechanism of action: Cefuroxime inhibits bacterial cell wall synthesis following attachment to penicillin binding proteins (PBPs). This results in the interruption of cell wall (peptidoglycan) biosynthesis, which leads to bacterial cell lysis and death.
Mechanism of resistance: Bacterial resistance to cefuroxime may be due to one or more of the following mechanisms: hydrolysis by beta-lactamases including (but not limited to) extended-spectrum beta-lactamases (ESBLs), and Amp-C enzymes, that may be induced or stably derepressed in certain aerobic Gram-negative bacterial species; reduced affinity of penicillin-binding proteins for cefuroxime; outer membrane impermeability, which restricts access of cefuroxime to penicillin binding proteins in Gram-negative bacteria; bacterial efflux pumps.
Organisms that have acquired resistance to other injectable cephalosporins are expected to be resistant to cefuroxime. Depending on the mechanism of resistance, organisms with acquired resistance to penicillins may demonstrate reduced susceptibility or resistance to cefuroxime.
Pharmacodynamics: Zocef Kids: Cefuroxime (as axetil) is an oral prodrug of the bactericidal cephalosporin antibiotic cefuroxime, which is resistant to most β (beta)-lactamases and is active against a wide range of Gram-positive and Gram-negative organisms.
It is indicated for the treatment of infections caused by susceptible bacteria.
Susceptibility to Cefuroxime (as axetil) will vary with geography and time and local susceptibility data should be consulted where available.
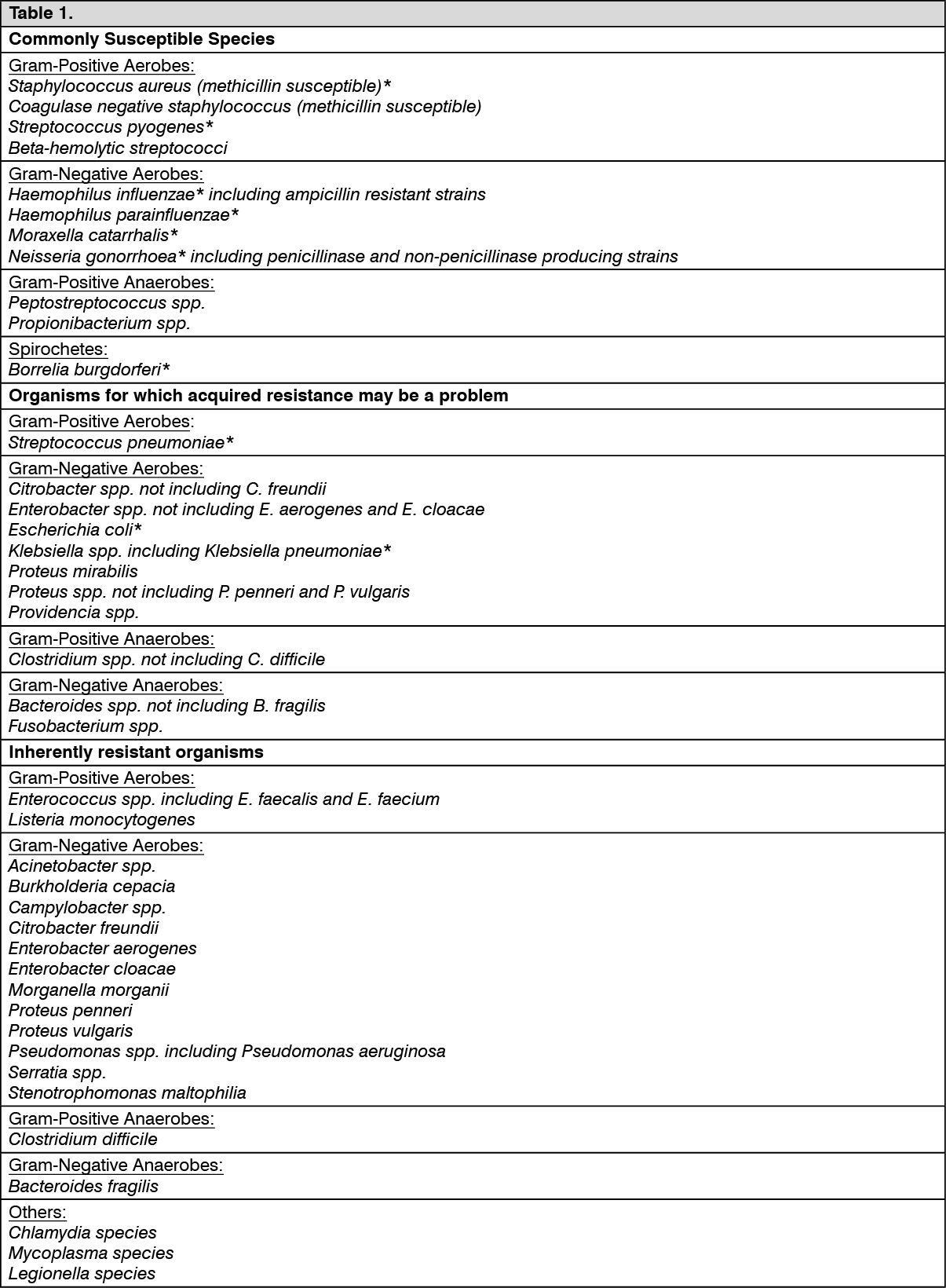
The prevalence of acquired resistance is geographically and time dependent and for select species may be very high. Local information on resistance is desirable, particularly when treating severe infections. (See Table 1.)
 Click on icon to see table/diagram/image
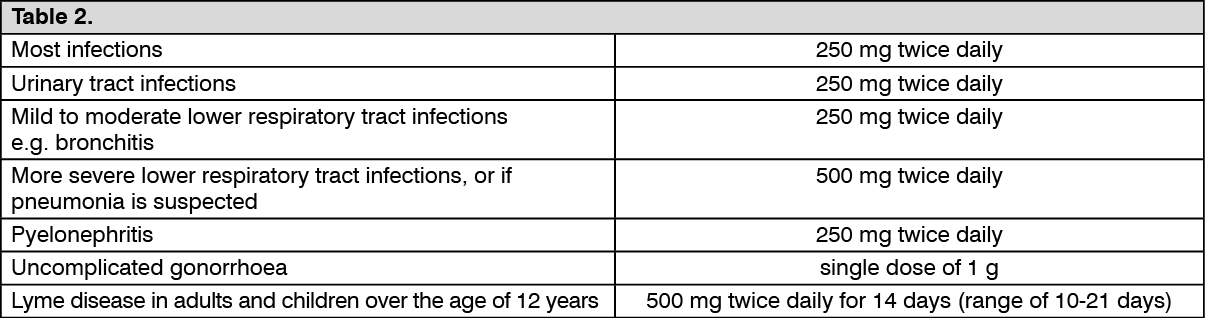
Pharmacokinetics: Zocef: Tablet:
Click on icon to see table/diagram/image
Pharmacokinetics: Zocef: Tablet: Cefuroxime axetil is absorbed from the gastrointestinal tract and is rapidly hydrolysed in the intestinal mucosa and blood to cefuroxime; absorption is enhanced in the presence of food. Peak plasma concentrations are reported about 2 to 3 hours after an oral dose. Up to 50% of cefuroxime in the circulation is bound to plasma proteins. The plasma half-life is about 70 minutes and is prolonged in patients with renal impairment and in neonates. Cefuroxime is widely distributed in the body including pleural fluid, sputum, bone, synovial fluid and aqueous humour, but only achieves therapeutic concentrations in the CSF when the meninges are inflamed. It crosses the placenta and has been detected in breast milk. Cefuroxime is excreted unchanged, by glomerular filtration and renal tubular secretion and high concentrations are achieved in the urine. Probenecid competes for renal tubular secretion with cefuroxime resulting in higher and more prolonged plasma concentrations of cefuroxime. Small amounts of cefuroxime are excreted in bile. Plasma concentrations are reduced by dialysis.
Suspension: Cefuroxime is widely distributed in the body including pleural fluid, sputum, bone, synovial fluid, and aqueous humour, but only achieves therapeutic concentrations in the CSF when the meninges are inflamed. It crosses the placenta and has been detected in breast milk. It is excreted unchanged by glomerular filtration and renal tubular secretion, and high concentrations are achieved in the urine. Following injection, most of a dose of cefuroxime is excreted within 24 hours, the majority within 6 hours. Probenecid competes for renal tubular secretion with cefuroxime resulting in higher and more prolonged plasma concentrations of cefuroxime. Small amounts of cefuroxime are excreted in bile. Plasma concentrations are reduced by dialysis.
Zocef Kids: Absorption: After oral administration Cefuroxime (as axetil) is slowly absorbed from the gastrointestinal tract and rapidly hydrolysed in the intestinal mucosa and blood to release cefuroxime into the circulation.
Optimum absorption occurs when it is administered shortly after a meal.
Following administration of Cefuroxime (as axetil) tablets peak serum levels (2.1 mg/l for a 125 mg dose, 4.1 mg/l for a 250 mg dose, 7.0 mg/l for a 500 mg dose and 13.6 mg/l for a 1 g dose) occur approximately 2 to 3 hours after dosing when taken with food.
Distribution: Protein binding has been variously stated as 33 to 50% depending on the methodology used.
Metabolism: Cefuroxime is not metabolized.
Elimination: The serum half life is between 1 and 1.5 hours.
Cefuroxime is excreted by glomerular filtration and tubular secretion. Concurrent administration of probenecid increases the area under the mean serum concentrations time curve by 50%.
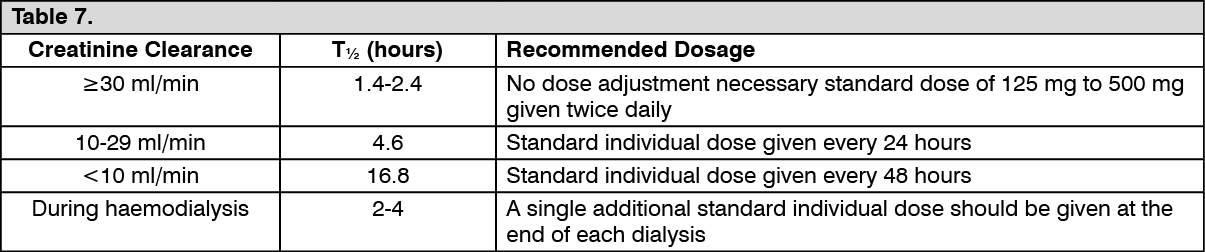
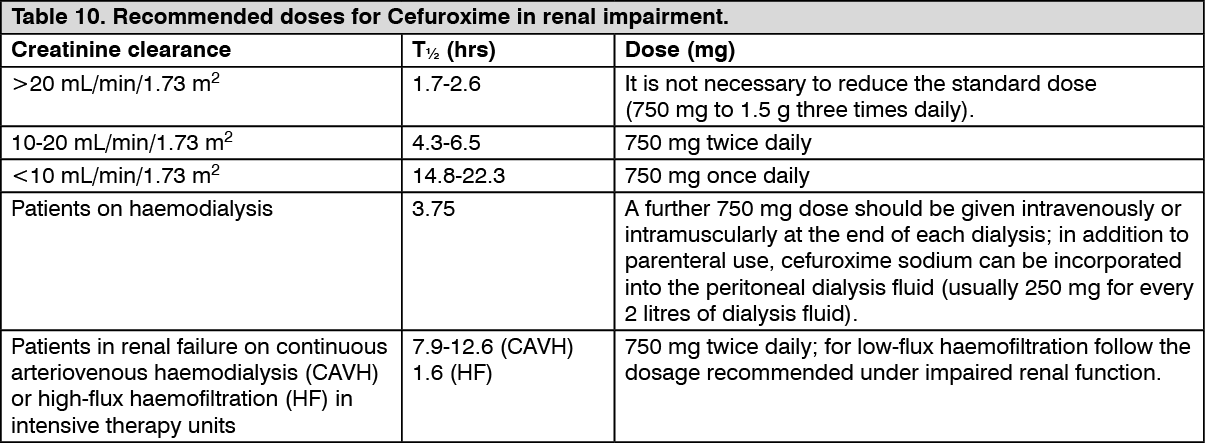
Renal Impairment: Cefuroxime pharmacokinetics have been investigated in patients with various degrees of renal impairment. Cefuroxime elimination half life increases with decrease in renal function which serves as the basis for dosage adjustment recommendations in this group of patients. In patients undergoing haemodialysis, at least 60% of the total amount of cefuroxime present in the body at the start of dialysis will be removed during a 4-hour dialysis period. Therefore, an additional single dose of cefuroxime should be administered following the completion of haemodialysis.
Zocef Hospi: Absorption: After intramuscular (IM) injection of cefuroxime to normal volunteers, the mean peak serum concentrations ranged from 27 to 35 μg/mL for a 750 mg dose and from 33 to 40 μg/mL for a 1000 mg dose, and were achieved within 30 to 60 minutes after administration. Following intravenous (IV) doses of 750 and 1500 mg, serum concentrations were approximately 50 and 100 μg/mL, respectively, at 15 minutes.
AUC and C
max appear to increase linearly with increase in dose over the single dose range of 250 to 1000 max mg following IM and IV administration. There was no evidence of accumulation of cefuroxime in the serum from normal volunteers following repeat intravenous administration of 1500 mg doses every 8 hours.
Distribution: Protein binding has been stated as 33 to 50%, depending on the methodology used. The average volume of distribution ranges from 9.3 to 15.8 L/1.73 m
2 following IM or IV administration over the dosage range of 250 to 1000 mg. Concentrations of cefuroxime in excess of the minimum inhibitory levels for common pathogens can be achieved in the tonsilla, sinus tissues, bronchial mucosa, bone, pleural fluid, joint fluid, synovial fluid, interstitial fluid, bile, sputum and aqueous humour. Cefuroxime passes the blood-brain barrier when the meninges are inflamed.
Biotransformation: Cefuroxime is not metabolised.
Elimination: Cefuroxime is excreted by glomerular filtration and tubular secretion. The serum half-life after either intramuscular or intravenous administration is approximately 70 minutes. There is an almost complete recovery (85 to 90%) of unchanged cefuroxime in urine within 24 hours of administration. The majority of the cefuroxime is excreted within the first 6 hours. The average renal clearance ranges from 114 to 170 mL/min/1.73 m2 following IM or IV administration over the dosage range of 250 to 1000 mg.
Special patient populations: Gender: No differences in the pharmacokinetics of cefuroxime were observed between males and females following a single IV bolus injection of 1000 mg of cefuroxime as the sodium salt.
Elderly: Following IM or IV administration, the absorption, distribution and excretion of cefuroxime in elderly patients are similar to younger patients with equivalent renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in cefuroxime dose selection, and it may be useful to monitor renal function.
Paediatrics: The serum half-life of cefuroxime has been shown to be substantially prolonged in neonates according to gestational age. However, in older infants (aged >3 weeks) and in children, the serum half-life of 60 to 90 minutes is similar to that observed in adults.
Renal impairment: Cefuroxime is primarily excreted by the kidneys. As with all such antibiotics, in patients with markedly impaired renal function (i.e. C1cr <20 mL/minute) it is recommended that the dosage of cefuroxime should be reduced to compensate for its slower excretion. Cefuroxime is effectively removed by haemodialysis and peritoneal dialysis.
Hepatic impairment: Since cefuroxime is primarily eliminated by the kidney, hepatic dysfunction is not expected to have an effect on the pharmacokinetics of cefuroxime.
PK/PD relationship: For cephalosporins, the most important pharmacokinetic-pharmacodynamic index correlating with
in vivo efficacy has been shown to be the percentage of the dosing interval (%T) that the unbound concentration remains above the minimum inhibitory concentration (MIC) of cefuroxime for individual target species (i.e. %T>MIC).
Microbiology: Zocef: Tablet: The
in vivo bactericidal activity of cefuroxime axetil is due to cefuroxime's binding to essential target proteins and the resultant inhibition of cell-wall synthesis. Cefuroxime has bactericidal activity against a wide range of common pathogens, including many beta-lactamase-producing strains. Cefuroxime is stable to many bacterial beta-lactamases, especially plasmid-mediated enzymes that are commonly found in enterobacteriaceae. Cefuroxime has been demonstrated to be active against most strains of the following microorganisms both
in vitro and in clinical infections.
Aerobic Gram-Positive Microorganisms:
Staphylococcus aureus (including beta-lactamase producing strains),
Streptococcus pneumonia, Streptococcus pyogenes, Staphylococcus epidermidis, Staphylococcus saprophyticus, Streptococcus agalactiae.
Aerobic Gram-Negative Microorganisms:
Escherichia coli, Haemophilus influenzae (including beta-lactamase-producing strains),
Haemophilus parainfluenzae, Klebsiella pneumonia, Moraxella catarrhalis (including beta-lactamase-producing strains),
Neisseria gonorrhoeae (including beta-lactamase-producing strains),
Spirochetes, Borrelia burgdorferi.

 Sign Out
Sign Out