Each actuation contains 2.0 mg of budesonide.
Excipients/Inactive Ingredients: Cetyl alcohol (Ph.Eur.), Cetostearyl alcohol (Ph.Eur.), Polysorbate 60, Purified water, Disodium edetate (Ph.Eur.), Macrogol stearyl ether (Ph.Eur.), Propylene glycol, Citric acid monohydrate.
Propellant: n-butane, Isobutane, Propane.
Pharmacotherapeutic group: Intestinal anti-inflammatory agent. ATC code: A07EA06, Corticosteroid with local effect.
Pharmacology: Pharmacodynamics: The exact mechanism of action of budesonide in the treatment of ulcerative colitis/proctosigmoiditis is not fully understood. Data from clinical pharmacology and controlled clinical trials strongly indicate that the mode of action of budesonide is predominantly based on a local action in the gut. Budesonide is a glucocorticosteroid with a high local anti-inflammatory effect. At a dosage of 2 mg budesonide, applied rectally, which is clinically equieffective with systemically acting glucocorticoids, budesonide leads to practically no suppression of the HPA axis. Budenofalk rectal foam investigated up to the daily dosage of 4 mg budesonide showed virtually no influence on the plasma cortisol level.
Pharmacokinetics: General aspects of budesonide: Absorption: After oral application, the systemic availability of budesonide is about 10%.
Distribution: Budesonide has a high volume of distribution (about 3 l/kg). Plasma protein binding averages 85-90%.
Biotransformation: Budesonide undergoes extensive biotransformation in the liver (approximately 90%) to metabolites of low glucocorticosteroid activity. The glucocorticosteroid activity of the major metabolites, 6β-hydroxybudesonide and 16α-hydroxyprednisolone - both of which are formed via CYP3A - is less than 1% of that of budesonide.
Elimination: The average elimination half-life after oral administration is about 3-4 hours. The mean clearance rate is about 10 l/min for budesonide.
Special patient groups (patients with impaired hepatic function): Depending on the type and severity of the liver disease, the metabolism of budesonide via CYP3A can be reduced in these patients.
Specific aspects of Budenofalk rectal foam: Absorption: The areas under the concentration-time curves after rectal administration are somewhat higher than after oral administration (historical controls). Peak levels with application of Budenofalk rectal foam are obtained after an average of 2-3 hours. Accumulation after repeated application can be ruled out.
Spread: A scintigraphic investigation with technetium-marked Budenofalk rectal foam in patients with ulcerative colitis showed that the foam spreads out over the entire sigmoid.
Toxicology: Preclinical safety data: After repeated oral administration of budesonide in rats (dose comparable to that used in humans), a reduction in the leukocyte count (especially lymphocytes) and regression of the thymus gland were observed. There was evidence of adrenal atrophy due to inactivity. Increased lactiferous duct proliferation and secretory activity were found in the mammary glands. In a long-term study (104 weeks), the haematocrit, haemoglobin and red cell count were reduced in female rats. In the same dosage group, there was a tendency for the neutrophil count to increase and values for lymphocytes, eosinophils and normocytes to decrease. The number of lymphocytes was significantly reduced (immunosuppressant effect) and alkaline phosphatase was slightly increased only in male animals.
In dogs, packed cell volume was reduced, alkaline phosphatase and alanine aminotransferase were elevated, the adrenals and lymphatic system were atrophied, and myocardial fat count and hepatic glycogen content (hepatomegaly) were increased.
Mutagenicity: Budesonide had no mutagenic effects in a number of in vitro and in vivo tests.
Carcinogenicity: Male rats treated with budesonide for up to 104 weeks developed a slightly increased number of basophilic hepatic foci compared with control animals. In the carcinogenicity study, the incidences of primary hepatocellular neoplasms (0.025 and 0.05 mg/kg body weight/day), astrocytomas (male rats 0.05 mg/kg body weight/day) and mammary tumours (female rats 0.05 mg/kg body weight/day) were significantly increased. The hepatic tumours are probably due anabolic effects and the increased metabolic load on the liver. The findings represent a class effect probably involving glucocorticoid receptors.
Reproductive toxicity: Glucocorticoids induce teratogenic effects (cleft palate, skeletal malformations) in animal studies in several species. The clinical relevance of these properties is not yet known. In rodents, subcutaneous budesonide showed the changes already known from other glucocorticoids. Animal studies have also shown that administration of synthetic glucocorticoids during gestation can lead to a higher risk of intrauterine growth retardation and can contribute to cardiovascular and/or metabolic diseases in adults, as well as a permanent change in glucocorticoid receptor density, neurotransmitter turnover and behaviour.
For the acute treatment of active ulcerative colitis that is limited to the rectum and the sigmoid colon.
Posology: Adults: One actuation of 2 mg budesonide daily.
Children and adolescents: Budenofalk rectal foam should not be taken by children and adolescents due to insufficient experience in this age group.
Method of administration: For rectal use.
This medicine may only be used rectally, so it has to be inserted through the anus. It is not intended to be taken by mouth. Do not swallow.
Budenofalk Rectal Foam may be used in the morning or evening.
The best results are obtained if the patient uses Budenofalk Rectal Foam after he/she has defecated.
The applicator (insertion aid) is in a special rail. Hold the rail firmly and pull the applicator out sharply.
Preparing to use the foam: Ensure that Budenofalk Rectal Foam is at room temperature before use. Push the applicator firmly onto the nozzle of the spray can. Mix contents by shaking the spray can vigorously for 10 to 15 seconds.
Before first use, remove the safety tab under the pump dome.
Twist the pump dome on top of the canister until the semi-circular notch underneath it is in line with the nozzle. The spray can is now ready for use.
Using the foam: Place the forefinger on the top of the pump dome and turn the spray can upside down. Note that the spray can will only work properly when held with the pump dome pointing down as vertically as possible.
Insert the applicator into the rectum as far as possible. The easiest way to use Budenofalk Rectal Foam is to keep one foot on the floor and raise the other foot onto a firm surface such as a chair or stool. To apply a dose of Budenofalk Rectal Foam, push the pump dome down fully once and hold it in this position for about 2 seconds. Then release it very slowly. The foam is now released into the rectum. Wait 10-15 seconds before withdrawing the applicator from the rectum, as the foam still expands a little and would otherwise drop out of the applicator unused.
After applying the foam, remove the applicator and dispose of it as domestic waste, using the plastic bag provided. Use a new applicator for each application. In order to prevent the inadvertent loss of foam from the spray can between applications, turn the pump dome around so that the semi-circular notch faces the direction opposite to the nozzle.
The best results are obtained when the intestine is evacuated prior to administration of Budenofalk rectal foam.
Duration of treatment: The attending physician determines the duration of use. An acute episode generally subsides after 6 to 8 weeks. Budenofalk rectal foam should not be used after this period of time.
To date, no cases of overdose with budesonide are known.
Budenofalk rectal foam must not be used in: hypersensitivity to budesonide or any of the ingredients; hepatic cirrhosis.
Treatment with Budenofalk rectal foam results in lower systemic steroid levels than conventional oral glucocorticosteroid therapy with systemically acting corticoids. Transfer from another glucocorticosteroid therapy may result in reappearance or recurrence of symptoms relating to the change in systemic steroid levels.
Caution is required in patients suffering from one or several of the following diseases: tuberculosis, hypertension, diabetes mellitus, osteoporosis, peptic ulcer (gastric or duodenal ulcer), glaucoma, cataract, family history of diabetes, family history of glaucoma, or any other condition in which glucocorticosteroids may have undesirable effects.
Systemic effects of glucocorticosteroids may occur, particularly when prescribed at high doses and for prolonged periods. Such effects may include Cushing’s syndrome, adrenal suppression, growth retardation, decreased bone mineral density, cataract, glaucoma and a wide range of psychiatric/behavioural effects (see Adverse Reactions).
Infections: Suppression of the inflammatory response and immune function increases the susceptibility to infections and their severity. The risk of deterioration of bacterial, fungal, amoebic and viral infections during glucocorticosteroid treatment should be carefully considered. The clinical presentation may often be atypical and serious infections such as septicaemia and tuberculosis may be masked, and therefore may reach an advanced stage before being recognised.
Chickenpox is of particular concern since this illness may be serious or fatal in immunosuppressed patients. Patients without a definite history of chickenpox should be advised to avoid close contact with persons suffering from chickenpox or shingles (herpes zoster) and, if exposed, they should seek urgent medical attention. Passive immunisation with varicella-zoster immunoglobulin is needed by exposed non-immunised patients who are receiving systemic glucocorticosteroids or who have used them within the previous 3 months. Immunisation should be given within 10 days of exposure to chickenpox. If a diagnosis of chickenpox is confirmed, the illness warrants specialist care and urgent treatment. Glucocorticosteroids should not be stopped and the dose may need to be increased. Corresponding precautionary measures must also be taken for a possible infection with measles.
Vaccines: Live vaccines should not be given to individuals with chronic glucocorticosteroid use. The antibody response to other(inactivated) vaccines may be diminished.
Patients with liver function disorders: Based on the experience with patients suffering from late stage primary biliary cirrhosis (PBC) with hepatic cirrhosis an increased systemic availability of budesonide in all patients with severely impaired hepatic function is to be expected. However, in patients with liver disease without hepatic cirrhosis budesonide in daily oral doses of 9 mg was safe and well tolerated. There is no evidence that a specific dose recommendation for patients with non-cirrhotic liver diseases or only slightly impaired liver function is necessary.
Visual disturbance: Visual disturbance may be reported with systemic and topical corticosteroid use. If a patient presents with symptoms such as blurred vision or other visual disturbances, the patient should be considered for referral to an ophthalmologist for evaluation of possible causes which may include cataract, glaucoma or rare diseases such as central serous chorioretinopathy (CSCR) which have been reported after use of systemic and topical corticosteroids.
Others: Budenofalk rectal foam may cause suppression of the hypothalamic-pituitary-adrenal (HPA) axis and reduce the stress response. When patients are subject to surgery or other stresses, supplementary systemic glucocorticosteroid treatment is recommended.
Concomitant treatment with ketoconazole or other CYP3A inhibitors should be avoided because inhibition of the oxidative biotransformation of budesonide can result in elevated plasma levels of budesonide (see Interactions).
It should also be noted that systemic glucocorticoid-like side effects can occur with doses that are higher than recommended (see Adverse Reactions).
Cetyl alcohol can cause local skin irritation (e.g. contact dermatitis). Propylene glycol can cause skin irritation. Budenofalk rectal foam does not contain preservatives.
Effects on ability to drive and use machines: No studies on the effects on the ability to drive and use machines have been performed.
Use in Children: Due to insufficient experience, Budenofalk rectal foam should not be used in children and adolescents.
Pregnancy: Administration during pregnancy should be avoided unless there are compelling reasons for therapy with Budenofalk 2mg rectal foam. There are few data of pregnancy outcomes after oral administration of budesonide in humans. Although data on the use of inhaled budesonide in a large number of exposed pregnancies indicate no adverse effect, the maximal concentration of budesonide in plasma has to be expected to be higher in the treatment with Budenofalk 2mg rectal foam compared to inhaled budesonide. In pregnant animals, budesonide, like other glucocorticosteroids, has been shown to cause abnormalities of fetal development (see Pharmacology: Toxicology: Preclinical safety data under Actions). The relevance of this to man has not been established.
Breast-feeding: Budesonide is excreted in human milk (data on excretion after inhalative use is available). However, only minor effects on the breast-fed child are anticipated after application of Budenofalk 2mg rectal foam within the therapeutic range. A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from budesonide therapy taking into account the benefit of breast feeding for the child and the benefit of therapy for the woman.
Fertility: There are no data on the effect of budesonide on human fertility. Fertility was unaffected following budesonide treatment in animal studies (see Pharmacology: Toxicology: Preclinical safety data under Actions).
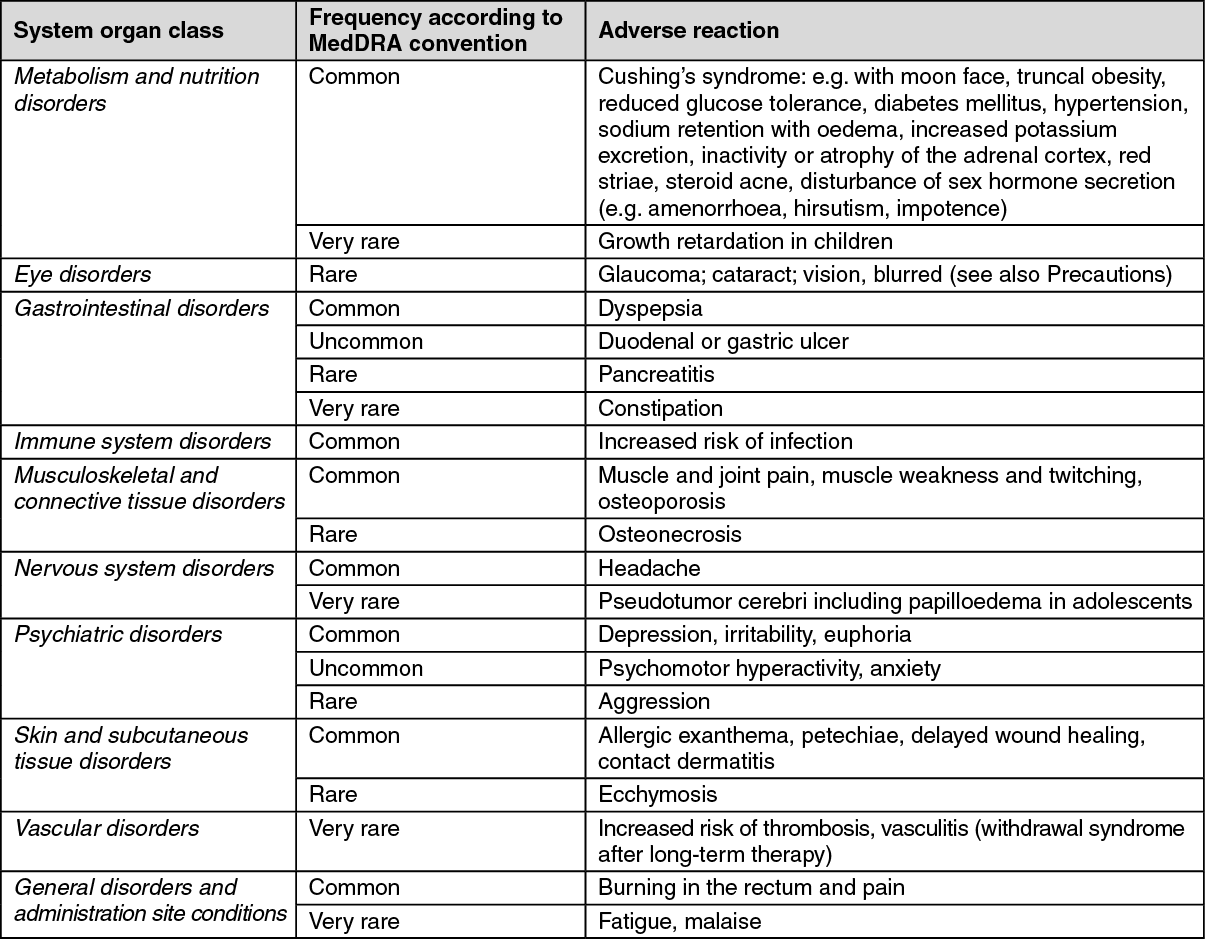
The following frequency conventions are used in the evaluation of undesirable effects: Very common: (<1/10), Common: (<1/100 to <1/10), Uncommon: (<1/1,000 to <1/100), Rare: (<1/10,000 to < 1/1,000), Very rare: (<1/10,000), not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The following adverse reactions were additionally reported in clinical studies with Budenofalk 2mg rectal foam (frequency: uncommon): increased appetite, increase in erythrocyte sedimentation rate, leucocytosis, nausea, abdominal pain, flatulence, paraesthesias in the abdominal region, anal fissure, aphthous stomatitis, frequent urge to defecate, rectal bleeding, increase in transaminases (GOT, GPT), increase in parameters of cholestasis (GGT,AP), increase in amylase, change in cortisol, urinary tract infection, dizziness, disturbances of smell, insomnia, increased sweating, asthenia, increase in body weight.
Most of the adverse events mentioned in this SmPC can also be expected for treatments with other glucocorticosteroids.
Occasionally, adverse events may occur which are typical for systemic glucocorticosteroids. These adverse events depend on the dosage, the period of treatment, concomitant or previous treatment with other glucocorticosteroids and the individual sensitivity.
Some of these undesired effects were reported after long-term use of orally administered budesonide.
Due to its local action, the risk of undesired effects of Budenofalk rectal foam is generally lower than with systemically acting glucocorticoids.
An exacerbation or the reappearance of extra intestinal manifestations (especially affecting skin and joints) can occur on switching a patient from systemically acting glucocorticosteroids to the locally acting budesonide.
Pharmacodynamic interactions: Cardiac glycosides: The action of the glycoside can be potentiated by potassium deficiency.
Saluretics: Potassium excretion can be increased.
Pharmacokinetic interactions: Cytochrome P450 3A (CYP3A): CYP3A inhibitors: Co-treatment with CYP3A inhibitors, including cobicistat-containing products, is expected to increase the risk of systemic side-effects. The combination should be avoided unless the benefit outweighs the increased risk of systemic corticosteroid side-effects, in which case patients should be monitored for systemic corticosteroid side-effects.
Ketoconazole 200 mg once daily p.o. increased the plasma concentrations of budesonide (3 mg single dose) approximately 6-fold during concomitant administration. When ketoconazole was administered 12 hours after budesonide, the concentrations increased approximately 3-fold. As there are not enough data to give dose recommendations, the combination should be avoided.
Other potent inhibitors of CYP3A4 such as ritonavir, itraconazole, clarithromycin and grapefruit juice are also likely to cause a marked increase of the plasma concentrations of budesonide. Therefore concomitant administration of budesonide should be avoided.
CYP3A inducers such as carbamazepine and rifampicin can reduce both the systemic as well as the local exposure of budesonide at the gut mucosa. An adjustment of the budesonide dose might be necessary.
CYP3A substrates such as ethinyl estradiol compete in the metabolism of budesonide. If the affinity of the competing substance for CYP3A is greater, this can lead to higher plasma concentrations of budesonide. If budesonide binds stronger to CYP3A, this can result in higher plasma levels of the competing substance. It may then be necessary to adjust the dose of budesonide or of the competing substance.
Elevated plasma concentrations and increased effects of glucocorticosteroids have been reported in women also receiving oestrogens or oral contraceptives, but this has not been observed with oral low-dose combination contraceptives.
Because adrenal function may be suppressed by treatment with budesonide, an ACTH stimulation test for diagnosing pituitary insufficiency might show false results (low values).
Incompatibilities: Not applicable.
Special precautions for disposal and other handling: No special requirements.
Shelf life: 2 years.
After first actuation: 4 weeks when stored at or below 25°C.
Do not store above 25°C.
Do not refrigerate or freeze.
Do not expose to temperature higher than 50°C.
This is a pressurised container, containing 6.9% by mass of inflammable propellant. It should be kept away from any flames or sparks, including cigarettes. It should be protected from direct sunlight and must not be forced open, pierced or burned even when empty. Do not spray near a flame or incandescent material.
A07EA06 - budesonide ; Belongs to the class of corticosteroids acting locally. Used in the treatment of intestinal inflammation.
Budenofalk Rectal Foam 2 mg/actuation
14 actuation x 1's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out