PHARMACOLOGY: AlphaNine SD is a purified formulation of Factor IX containing not less than 150 IU Factor IX activity/mg of total protein. AlphaNine SD contains non-therapeutic levels of Factor II, Factor VII and Factor X.
Thrombogenicity of AlphaNine SD in animals is markedly lower than that of Factor IX Complex, Profilnine Heat-Treated. Five lots of AlphaNine SD (three lots of non-virus filtered product and two lots of virus filtered product) failed to show any evidence of thrombogenicity when tested directly in the Wessler rabbit stasis model for thrombogenicity at a dose of 200 IU Factor IX/kg body weight. When various lots of AlphaNine SD were further tested at doses between 300 and 650 IU Factor IX/kg, only 5 out of 40 animals (12.5%) showed evidence of thrombus formation (Wessler scores of +1, +2, +1, +1, +1 out of +4 maximum). In comparison, Factor IX Complex concentrate, Profilnine, was thrombogenic in 100% of the animals tested at a dose of 100 IU Factor IX/kg.
At a dose of 200 IU Factor IX/kg body weight in a porcine model, the heptane heat-treated formulation of this product (AlphaNine) showed little evidence of disseminated intravascular coagulation (DIC) following infusion. This model exhibited no depletion of coagulation factors, a minimal increase in fibrin monomer (+1 in protamine test), a slight temporary decrease in platelet counts, and no evidence of intravascular coagulation upon gross autopsy. In contrast, Harrison, et al., report that all Factor IX Complex concentrates studied in the same porcine model were thrombogenic at doses between 50 and 100 IU of Factor IX/kg animal weight.
A clinical evaluation of AlphaNine SD half-life and recovery characteristics was performed. A total of 18 patients with severe to moderate hemophilia B each received a single infusion of 40 to 50 IU Factor IX/kg body weight of AlphaNine SD. Following the administration of AlphaNine SD, the mean half-life of Factor IX observed was approximately 21 hours. This half-life value was computed using the biphasic linear regression model recommended by the International Society of Thrombosis and Haemostasis. The half-life obtained for the solvent detergent treated product is comparable to that of AlphaNine (approximately 19 hours) as well as the range of 18 to 36 hours reported for Factor IX Complex preparations. The mean recovery observed in clinical trials was approximately 48% and was comparable to that of AlphaNine (approximately 51%).
A clinical trial was conducted using the heptane heat-treated product, AlphaNine, to evaluate the efficacy of the product in providing hemostatic protection during and after surgery in 13 patients with hemophilia B. The types of surgical procedures performed included bilateral knee replacement (1), total knee replacement with synovectomy (2), hip replacement (1), below the knee amputation (1), herniorrhaphy (2), hemorrhoidectomy (1), rhinoplasty (2), oral surgery (2) and Hickman catheter insertion with temporalis muscle transfer (1). Presurgery doses ranged from 30.1 to 65.0 IU Factor IX/kg; postsurgery replacement therapy doses ranged from approximately 9.4 to 52.0 IU Factor IX/kg. The number of postsurgery days of treatment ranged from 1 to 23; the number of postsurgery infusions ranged from 2 to 26. No bleeding episodes were reported and hemostasis was maintained during the course of postsurgery therapy. None of the hematologic parameters examined (hematocrit, partial thromboplastin time, prothrombin time, fibrinogen/fibrin degradation products, fibrin monomers, D-dimers and platelet counts) provided any evidence that AlphaNine possessed thrombogenic potential.
A randomized crossover study with 11 hemophilia B patients was conducted with the heptane heat-treated version of the product, AlphaNine, to determine whether an infusion of AlphaNine caused less activation of the hemostatic system than the Factor IX Complex concentrate preparation, Profilnine Heat-Treated. Each subject received a single infusion of either AlphaNine or Profilnine Heat-Treated for the treatment of a bleeding episode, at a dose of 50 IU Factor IX/kg body weight. Each subject received the other Factor IX concentrate for the treatment of a subsequent bleeding episode, separated by an interval of not less than 10 days. The level of prothrombin fragment 1+2 (F
1 + 2) is a sensitive index of the cleavage of prothrombin by activated Factor X. The level of fibrinopeptide A (FPA) released into the plasma measures the activity of thrombin on fibrinogen in the formation of fibrin. Following infusion of Factor IX Complex, statistically significant increases in F
1 + 2 and in FPA were detected at all monitored time points (15, 60, 90, 120 and 240 minutes postinfusion). The statistically significant elevation in these two hemostatic parameters indicates increased activation of the coagulation cascade. Administration of AlphaNine resulted in no increase in F
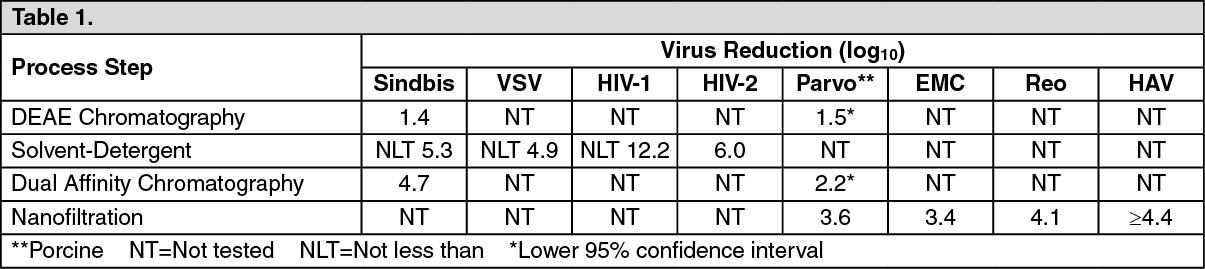
1 + 2 at any monitored time points, and a statistically non-significant increase in FPA at 15, 60, and 90 minutes following infusion. Only at 120 and 240 minutes after infusion of AlphaNine were statistically significant increases in FPA levels detected. These results suggest that the infusion of a high purity factor IX, such as AlphaNine, may result in a lower level of activation of the coagulation cascade than does Factor IX Complex. The ability of the manufacturing process to inactivate and eliminate virus from the Coagulation Factor IX (Human) products was evaluated at key stages in the process (see Table 1). Known amounts of different viruses were added to samples obtained prior to those steps most likely to reduce virus load (DEAE Chromatography, Solvent Detergent, Dual Affinity Chromatography and nanofiltration) in the AlphaNine and AlphaNine SD processes to determine the level of viral inactivation/elimination of these specific steps in the process. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The retrovirus known as human immunodeficiency virus (HIV) has been identified as a causative agent of Acquired Immunodeficiency Syndrome (AIDS) and has been shown to be transmissible via blood or blood products. The solvent detergent process used in the manufacture of AlphaNine SD, was shown to inactivate greater than 12.2 logs of HIV-1 when the retrovirus was intentionally added to product samples under laboratory evaluation (as measured by virus antigen capture and reverse transcriptase assays). In addition, this process was shown to inactivate 6 logs of HIV-2 (as measured by reverse transcriptase assays) when the retrovirus was intentionally added to product samples. In an ongoing efficacy and safety study of 26 patients, no subjects tested positive for HIV or viral hepatitis in relation to the investigation drug.
In order to assess the ability of the solvent detergent treatment process to inactivate other viruses such as hepatitis B and C virus, the inactivation of the model viruses, Sindbis virus, a model virus for hepatitis C virus, and vesicular stomatitis virus (VSV), a model RNA virus for lipid enveloped viruses, by solvent detergent treatment was studied. Prior to solvent detergent treatment, samples were inoculated with a titer of either Sindbis or VSV. The results demonstrated that a minimum of 5.3 logs of Sindbis and a minimum of 4.9 logs of VSV were inactivated after 180 minutes of incubation with solvent detergent (when compared to an untreated control). It should be noted that the incubation time in the actual AlphaNine SD process is twice (360 minutes total) that used in the model virus studies.
The ability of the AlphaNine SD process to eliminate virus, by physically partitioning virus from product, was evaluated at key stages of the manufacturing process. Studies were performed using a lipid-enveloped model virus (Sindbis) and non-lipid model viruses (porcine parvovirus, encephalomyocarditis virus, and reovirus). Known amounts of these viruses were added to samples obtained from the AlphaNine SD process. The amount of virus removed at each subsequent purification step was then determined by plaque assay.
Addition of Sindbis or porcine parvovirus prior to Factor IX Complex adsorption by DEAE chromatography showed this step to eliminate 1.4 logs of Sindbis and 1.5 logs (95% confidence interval: 1.51-2.33) of added porcine parvovirus. When Sindbis or parvovirus was introduced into the process after the barium citrate precipitation step of the AlphaNine SD process, the subsequent dual affinity chromatography step was found to eliminate 4.7 logs of Sindbis and 2.2 logs (95% confidence interval: 2.25-2.75) of added parvovirus. When parvovirus, encephalomyocarditis virus (EMC), or Reovirus was introduced into the process after the dual affinity chromatography step, the subsequent nanofiltration step of the AlphaNine SD process was found to eliminate 3.6 logs of parvovirus, 3.4 logs of EMC and 4.1 logs of added Reovirus. The studies mentioned previously indicate that the manufacturing process of AlphaNine SD is capable of reducing viruses by approximately 6 logs, in addition to virus reduction achieved by the solvent detergent process. In another study, the nanofiltration step removed ≥ 4.4 logs of hepatitis A virus (HAV), a non-lipid enveloped virus. Table 1 summarizes the reduction factors obtained for each virus when individual steps in the manufacturing process for AlphaNine SD were validated for virus removal/inactivation.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
