The following CIOMS frequency rating is used, when applicable: Very common ≥ 10%; Common ≥ 1 and < 10%; Uncommon ≥ 0.1 and < 1%; Rare ≥ 0.01% and < 0.1%; Very rare < 0.01%; Unknown (cannot be estimated from available data).
Glimepiride and Metformin: The use of a combination of both compounds, either as a free combination or as a fixed combination, is associated with the same safety characteristics as the use of each compound separately.
Glimepiride: Metabolism and nutrition disorders: As a result of the blood glucose-lowering action of glimepiride, hypoglycaemia may occur, which may also be prolonged.
Possible symptoms of hypoglycaemia include headache, ravenous hunger, nausea, vomiting, lassitude, sleepiness, disordered sleep, restlessness, aggressiveness, impaired concentration, impaired alertness and reactions, depression, confusion, speech disorders, aphasia, visual disorders, tremor, pareses, sensory disturbances, dizziness, helplessness, loss of self-control, delirium, cerebral convulsions, somnolence and loss of consciousness up to and including coma, shallow respiration and bradycardia.
In addition, signs of adrenergic counter-regulation may be present such as sweating, clammy skin, anxiety, tachycardia, hypertension, palpitations, angina pectoris, and cardiac arrhythmias.
The clinical picture of a severe hypoglycaemic attack may resemble that of a stroke.
The symptoms nearly always subside when hypoglycaemia is corrected.
Eye disorders: Especially at the start of treatment, there may be temporary visual impairment due to the change in blood glucose levels. The cause is a temporary alteration in the turgidity and hence the refractive index of the lens, this being dependent on blood glucose level.
Gastrointestinal disorders: Occasionally, gastrointestinal symptoms such as nausea, vomiting, sensations of pressure or fullness in the epigastrium, abdominal pain and diarrhoea may occur.
In isolated cases, there may be hepatitis, elevation of liver enzyme levels and/or cholestasis and jaundice, which may progress to life-threatening liver failure but can regress after withdrawal of glimepiride.
Dysguesia (frequency not known).
Blood and lymphatic system disorders: Changes in the blood picture may occur: Rarely, thrombocytopenia and in, isolated cases, leucopenia, haemolytic anaemia, erythrocytopenia, granulocytopenia, agranulocytosis or pancytopenia may develop. Cases of severe thrombocytopenia with platelet count less than 10,000/μl and thrombocytopenic purpura have been reported in post-marketing experience (frequency not known).
Skin and subcutaneous tissues disorders: Alopecia (frequency not known).
General disorders: Occasionally, allergic or pseudo-allergic reactions may occur, e.g. in the form of itching, urticaria or rashes. Such mild reactions may develop into serious reactions with dyspnea and a fall in blood pressure, sometimes progressing to shock. In the event of urticaria a physician must therefore be notified immediately.
In isolated cases, a decrease in serum sodium concentration and allergic vasculitis or hypersensitivity of the skin to light may occur.
Investigations: Glimepiride, like all sulfonylureas, can cause weight gain (frequency not known).
Metformin: Gastrointestinal symptoms such as nausea, vomiting, diarrhoea, abdominal pain and loss of appetite (>10%) are very common: these occur most frequently during initiation of therapy and resolve spontaneously in most cases. To prevent these gastrointestinal symptoms, it is recommended that metformin be taken in 2 or 3 daily doses during or after meals. A slow increase of the dose may also improve gastrointestinal tolerability.
Metallic taste (3%) is common.
Mild erythema has been reported in some hypersensitive individuals. The incidence of such effects is regarded as very rare (<0.01%).
A decrease of vitamin B12 absorption with decrease of serum levels has been observed in patients treated long-term with metformin and appears generally to be without clinical significance (<0.01%).
However, cases of peripheral neuropathy in patients with vitamin B12 deficiency have been reported in post-marketing experience (frequency not known) (see Precautions).
Lactic acidosis (0.03 cases/1,000 patient-years) is very rare (see Precautions).
Hemolytic anemia (frequency unknown).
Reduction of thyrotropin level in patients with hypothyroidism (see Precautions) (frequency unknown).
Hypomagnesemia in the context of diarrhea (frequency unknown).
Encephalopathy (frequency unknown).
Photosensitivity (frequency unknown).
Hepatobiliary disorders: Reports of liver function tests abnormalities and hepatitis resolving upon metformin discontinuation.


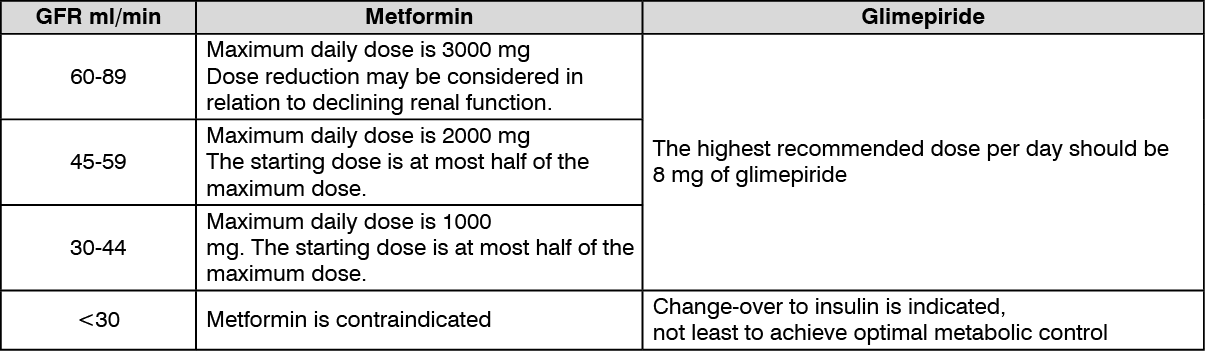 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
