Each vial of Biopharm Levo injection contains a solution with the equivalent of 750mg Levofloxacin in 150mL.
INN: Levofloxacin hemihydrate.
Salt form I Hydrate form: Hydrate form.
IUPAC name: (-)-(S)-9-Fluoro-2,3-dihydro-3-methyl-10-(4-methyl-1-piperazinyl)-7-oxo-7H-pyrido[1,2,3-de]-1,4-benzoxazine-6-carboxylic acid·hemihydrate.
Synonyms: (-)-9-Fluoro-3-(S)-methyl-10-(4-methyl-1-piperazinyl)-7-oxo2,3 dihydro-7H-pyrido[1,2,3- de]-1,4-benzoxazine-6-carboxylic acid hemihydrate.
Empirical Formula: C18H20FN304·1/2 H20.
Molecular mass: 370.38.
Excipients/Inactive Ingredients: Hydrochloric Acid, Sodium Hydroxide, Sodium Chloride.
Pharmacology: Pharmacodynamics: Levofloxacin is the L-isomer of the racemate, ofloxacin, a quinolone antimicrobial agent. The antibacterial activity of ofloxacin resides primarily in the L-isomer. The mechanism of action oflevofloxacin and other fluoroquinolone antimicrobials involves inhibition of bacterial topoisomerase IV and DNA gyrase (both of which are type II topoisomerases), enzymes required for DNA replication, transcription, repair and recombination.
Pharmacokinetics: Absorption: Rapid and complete.
Distribution: Vd 74-112 L.
Protein binding: 24% to 38%.
Metabolism: Minimally hepatic.
Bioavailability: 99%.
Half-life elimination: 6-8 hours.
Excretion: Urine (87% as unchanged drug, <5% as metabolites) and Feces (<4%).
Toxicology: Preclinical Safety Data: Acute toxicity data: Rat i.v. 423 mg/kg (♂), 395 mg/kg (♀) Dog i.v. 200 mg/kg (♀).
Chronic toxicity data: Beagle i.v. 3 mg/kg/day 4 weeks.
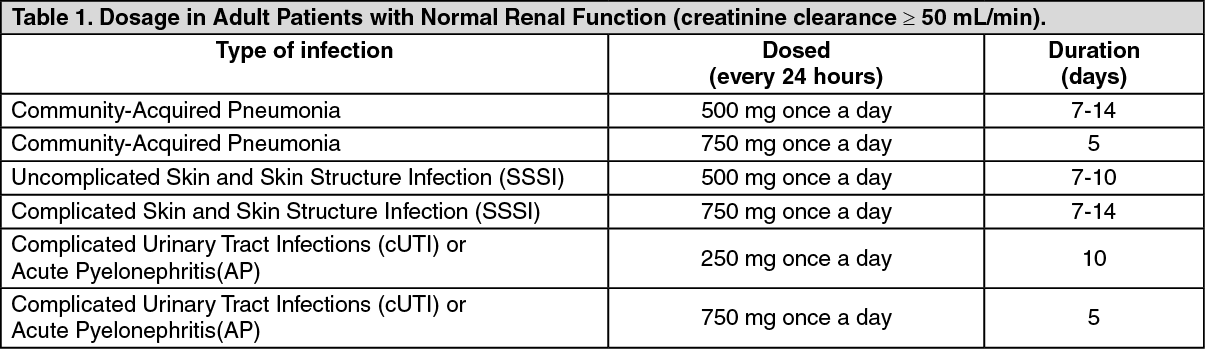
Community-Acquired Pneumonia; Skin and Skin Structure Infections; Complicated Urinary Tract Infections; Acute Pyelonephritis.
Biopharm Levo Injection should only be administered by intravenous infusion. It is not for intramuscular, intrathecal, intraperitoneal, or subcutaneous administration. The dosage depends on the type and severity of the infection and the sensitivity of the presumed causative pathogen. The duration of therapy varies according to the course of the disease. As with antibiotic therapy in general, administration of Biopharm Levo Injection should be continued for a minimum of 48 to 72 hours after the patient has become afebrile. It is usually possible to switch from initial intravenous treatment to the oral route after a few days.
The usual dose is 500mg administered by slow infusion over 60 minutes every 24 hours or 750mg administered by slow infusion over 90 minutes every 24 hours, as described in the following dosing table. (See Tables 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In the event of an acute overdosage, the stomach should be emptied. The patient should be observed and appropriate hydration maintained. Levofloxacin is not efficiently removed by hemodialysis or peritoneal dialysis.
Levofloxacin exhibits a low potential for acute toxicity. Mice, rats, dogs and monkeys exhibited the following clinical signs after receiving a single high dose of Levofloxacin; ataxia, ptosis, decreased locomotor activity, dyspnea, prostration, tremors, and convulsions.
Levofloxacin is contraindicated in persons with known hypersensitivity to levofloxacin, or other quinolone antibacterials.
Fluoroquinolones, including levofloxacin, are associated with an increased risk of tendinitis and tendon rupture in all ages. This risk is further increased in older patients usually over 60 years of age, in patients taking corticosteroid drugs, and in patients with kidney, heart or lung transplants.
Fluoroquinolones, including levofloxacin, may exacerbate muscle weakness in persons with myasthenia gravis. Avoid levofloxacin in patients with a known history of myasthenia gravis.
Tendinopathy and Tendon Rupture: Fluoroquinolones, including Levofloxacin, are associated with an increased risk of tendinitis and tendon rupture in all ages. This adverse reaction most frequently involves the Achilles tendon, and rupture of the Achilles tendon may require surgical repair. Tendinitis and tendon rupture in the rotator cuff (the shoulder), the hand, the biceps, the thumb, and other tendon sites have also been reported. The risk of developing fluoroquinolone-associated tendinitis and tendon rupture is further increased in older patients usually over 60 years of age, in those taking corticosteroid drugs, and in patients with kidney, heart or lung transplants. Factors, in addition to age and corticosteroid use, that may independently increase the risk of tendon rupture include strenuous physical activity, renal failure, and previous tendon disorders such as rheumatoid arthritis. Tendinitis and tendon rupture have been reported in patients taking fluoroquinolones who do not have the above risk factors. Tendon rupture can occur during or after completion of therapy; cases occurring up to several months after completion of therapy have been reported. Levofloxacin should be discontinued if the patient experiences pain, swelling, inflammation or rupture of a tendon. Patients should be advised to rest at the first sign of tendinitis or tendon rupture, and to contact their healthcare provider regarding changing to a non-quinolone antimicrobial drug.
Hypersensitivity Reactions: Serious and occasionally fatal hypersensitivity and/or anaphylactic reactions have been reported in patients receiving therapy with fluoroquinolones, including Levofloxacin. These reactions often occur following the first dose. Some reactions have been accompanied by cardiovascular collapse, hypotension/shock, seizure, loss of consciousness, tingling, angioedema (including tongue, laryngeal, throat, or facial edema/swelling), airway obstruction (including bronchospasm, shortness of breath, and acute respiratory distress), dyspnea, urticaria, itching, and other serious skin reactions. Levofloxacin should be discontinued immediately at the first appearance of a skin rash or any other sign of hypersensitivity. Serious acute hypersensitivity reactions may require treatment with epinephrine and other resuscitative measures, including oxygen, intravenous fluids, antihistamines, corticosteroids, pressor amines, and airway management.
Other Serious and Sometimes Fatal Reactions: Other serious and sometimes fatal events, some due to hypersensitivity, and some due to uncertain etiology, have been reported rarely in patients receiving therapy with fluoroquinolones, including Levofloxacin. These events may be severe and generally occur following the administration of multiple doses. Clinical manifestations may include one or more of the following: fever, rash, or severe dermatologic reactions (e.g., toxic epidermal necrolysis, Stevens-Johnson Syndrome); vasculitis, arthralgia, myalgia, serum sickness; allergic pneumonitis; interstitial nephritis, acute renal insufficiency or failure; hepatitis, jaundice, acute hepatic necrosis or failure; anemia, including hemolytic and aplastic, thrombocytopenia, including thrombotic thrombocytopenic purpura, leukopenia, agranulocytosis, pancytopenia, and/or other hematologic abnormalities.
The drug should be discontinued immediately at the first appearance of skin rash, jaundice, or any other sign of hypersensitivity and supportive measures instituted.
Hepatotoxicity: Post-marketing reports of severe hepatotoxicity (including acute hepatitis and fatal events) have been received for patients treated with Levofloxacin. No evidence of serious drug-associated hepatotoxicity was detected in clinical trials of over 7,000 patients. Severe hepatotoxicity generally occurred within 14 days of initiation of therapy and most cases occurred within 6 days. Most cases of severe hepatotoxicity were not associated with hypersensitivity. The majority of fatal hepatotoxicity reports occurred in patients 65 years of age or older and most were not associated with hypersensitivity. Levofloxacin should be discontinued immediately if the patient develops signs and symptoms of hepatitis.
Central Nervous System Effects: Convulsions and toxic psychoses have been reported in patients receiving fluoroquinolones, including Levofloxacin. Fluoroquinolones may also cause increased intracranial pressure and central nervous system stimulation which may lead to tremors, restlessness, anxiety, lightheadedness, confusion, hallucinations, paranoia, depression, nightmares, insomnia, and, rarely, suicidal thoughts or acts. These reactions may occur following the first dose. If these reactions occur in patients receiving Levofloxacin, the drug should be discontinued and appropriate measures instituted. As with other fluoroquinolones, Levofloxacin should be used with caution in patients with a known or suspected central nervous system (CNS) disorder that may predispose them to seizures or lower the seizure threshold (e.g., severe cerebral arteriosclerosis, epilepsy) or in the presence of other risk factors that may predispose them to seizures or lower the seizure threshold (e.g., certain drug therapy, renal dysfunction).
Clostridium difficile-Associated Diarrhea: Clostridium difficile-associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including Levofloxacin, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.
C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents.
If CDAD is suspected or confirmed, ongoing antibiotic use not directed against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated.
Peripheral Neuropathy: Rare cases of sensory or sensorimotor axonal polyneuropathy affecting small and/or large axons resulting in paresthesias, hypoesthesias, dysesthesias and weakness have been reported in patients receiving fluoroquinolones, including Levofloxacin. Levofloxacin should be discontinued if the patient experiences symptoms of neuropathy including pain, burning, tingling, numbness, and/or weakness or other alterations of sensation including light touch, pain, temperature, position sense, and vibratory sensation in order to prevent the development of an irreversible condition.
Prolongation of the QT Interval: Some fluoroquinolones, including Levofloxacin, have been associated with prolongation of the QT interval on the electrocardiogram and infrequent cases of arrhythmia. Rare cases of torsade de pointes have been spontaneously reported during post-marketing surveillance in patients receiving fluoroquinolones, including Levofloxacin. Levofloxacin should be avoided in patients with known prolongation of the QT interval, patients with uncorrected hypokalemia, and patients receiving Class IA (quinidine, procainamide), or Class III (amiodarone, sotalol) antiarrhythmic agents. Elderly patients may be more susceptible to drug-associated effects on the QT interval.
Musculoskeletal Disorders in Pediatric Patients and Arthropathic Effects in Animals: Levofloxacin is indicated in pediatric patients (≥ 6 months of age) only for the prevention of inhalational anthrax (post-exposure). An increased incidence of musculoskeletal disorders (arthralgia, arthritis, tendonopathy, and gait abnormality) compared to controls has been observed in pediatric patients receiving Levofloxacin.
In immature rats and dogs, the oral and intravenous administration of levofloxacin resulted in increased osteochondrosis. Histopathological examination of the weight-bearing joints of immature dogs dosed with levofloxacin revealed persistent lesions of the cartilage. Other quinolones also produce similar erosions in the weight-bearing joints and other signs of arthropathy in immature animals of various species.
Blood Glucose Disturbances: As with other fluoroquinolones, disturbances of blood glucose, including symptomatic hyper- and hypoglycemia, have been reported with Levofloxacin, usually in diabetic patients receiving concomitant treatment with an oral hypoglycemic agent (e.g., glyburide) or with insulin. In these patients, careful monitoring of blood glucose is recommended. If a hypoglycemic reaction occurs in a patient being treated with Levofloxacin, Levofloxacin should be discontinued and appropriate therapy should be initiated immediately.
Photosensitivity/Phototoxicity: Moderate to severe photosensitivity/phototoxicity reactions, the latter of which may manifest as exaggerated sunburn reactions (e.g., burning, erythema, exudation, vesicles, blistering, edema) involving areas exposed to light (typically the face, "V" area of the neck, extensor surfaces of the forearms, dorsa of the hands), can be associated with the use of fluoroquinolones after sun or UV light exposure. Therefore, excessive exposure to these sources of light should be avoided. Drug therapy should be discontinued if photosensitivity/phototoxicity occurs.
Development of Drug Resistant Bacteria: Prescribing Levofloxacin in the absence of a proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
Antibacterial Resistance: Antibacterial drugs including Levofloxacin should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When Levofloxacin is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by Levofloxacin or other antibacterial drugs in the future.
Effect on ability to drive and use machine: Patients should know how they react to Biopharm Levo before they operate an automobile or machinery or engage in other activities requiring mental alertness and coordination.
Pregnancy (Category C): Levofloxacin was not teratogenic in rats at oral doses as high as 810 mg/kg/day which corresponds to 9.4 times the highest recommended human dose based upon relative body surface area, or at intravenous doses as high as 160 mg/kg/day corresponding to 1.9 times the highest recommended human dose based upon relative body surface area. The oral dose of 810 mg/kg/day to rats caused decreased fetal body weight and increased fetal mortality. No teratogenicity was observed when rabbits were dosed orally as high as 50 mg/kg/day which correspond to 1.1 times the highest recommended human dose based upon relative body surface area, or when dosed intravenously as high as 25 mg/kg/day, corresponding to 0.5 times the highest recommended human dose based upon relative body surface area.
There are, however, no adequate and well-controlled studies in pregnant women. Levofloxacin should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Nursing Mothers: Based on data on other fluoroquinolones and very limited data on levofloxacin, it can be presumed that levofloxacin will be excreted in human milk. Because of the potential for serious adverse reactions from levofloxacin in nursing infants, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Serious and Otherwise Important Adverse Reactions: The following serious and otherwise important adverse drug reactions are discussed in greater details in other sections of labeling: Tendon Effects; Hypersensitivity Reactions; Other Serious and Sometimes Fatal Reactions; Hepatotoxicity; Central Nervous System Effects;
Clostridium difficile-Associated Diarrhea; Peripheral Neuropathy; Prolongation of the QT Interval; Musculoskeletal Disorders in Pediatric Patients; Blood Glucose Disturbances; Photosensitivity/Phototoxicity; Development of Drug Resistant Bacteria.
See Precautions for detail.
Hypotension has been associated with rapid or bolus intravenous infusion of Biopharm Levo should be infused slowly over 60 to 90 minutes, depending on dosage.
Crystalluria and cylindruria have been reported with quinolones, including Biopharm Levo. Therefore, adequate hydration of patients receiving Biopharm Levo should be maintained to prevent the formation of a high concentrated urine.
Biopharm Levo (levofloxacin) Injection: There are no data concerning an interaction of intravenous fluoroquinolones with oral antacids, sucralfate, multivitamins, didanosine, or metal cations. However, no fluoroquinolone should be co-administered with any solution containing multivalent cations, e.g., magnesium, through the same intravenous line.
Warfarin: No significant effect of Biopharm Levo (levofloxacin) on the peak plasma concentrations, AUC, and other disposition parameters for R- and S- warfarin was detected in a clinical study involving healthy volunteers. Similarly, no apparent effect of warfarin on levofloxacin absorption and disposition was observed. However, there have been reports during the post-marketing experience in patients that Biopharm Levo (levofloxacin) enhances the effects of warfarin. Elevations of the prothrombin time in the setting of concurrent warfarin and Biopharm Levo (levofloxacin) use have been associated with episodes of bleeding. Prothrombin time, International Normalized Ratio (INR), or other suitable anticoagulation tests should be closely monitored if Biopharm Levo (levofloxacin) is administered concomitantly with warfarin. Patients should also be monitored for evidence of bleeding.
Antidiabetic Agents: Disturbances of blood glucose, including hyperglycemia and hypoglycemia, have been reported in patients treated concomitantly with fluoroquinolones and an antidiabetic agent. Therefore, careful monitoring of blood glucose is recommended when these agents are coadministered.
Non-Steroidal Anti-Inflammatory Drugs: The concomitant administration of a non-steroidal anti-inflammatory drug with a fluoroquinolones, including Biopharm Levo (levofloxacin), may increase the risk of CNS stimulation and convulsive seizures.
Theophylline: No significant effect of Biopharm Levo (levofloxacin) on the plasma concentrations, AUC, and other disposition parameters for theophylline was detected in a clinical study involving healthy volunteers. Similarly, no apparent effect of theophylline on levofloxacin absorption and disposition was observed. However, concomitant administration of other fluoroquinolones with theophylline has resulted in prolonged elimination half-life, elevated serum theophylline levels, and a subsequent increase in the risk of theophylline-related adverse reactions in the patient population. Therefore, theophylline levels should be closely monitored and appropriate dosage adjustments made when Biopharm Levo (levofloxacin) is co-administered. Adverse reactions, including seizures, may occur with or without an elevation in serum theophylline levels.
Cyclosporine: No significant effect of Biopharm Levo (levofloxacin) on the peak plasma concentrations, AUC, and other disposition parameters for cyclosporine was detected in a clinical study involving healthy volunteers. However, elevated serum levels of cyclosporine have been reported in the patient population when co-administered with some other fluoroquinolones. Levofloxacin Cmax and ke were slightly lower while Tmax and t1/2 were slightly longer in the presence of cyclosporine than those observed in other studies without concomitant medication. The differences, however, are not considered to be clinically significant. Therefore, no dosage adjustment is required for Biopharm Levo (levofloxacin) or cyclosporine when administered concomitantly.
Digoxin: No significant effect of Biopharm Levo (levofloxacin) on the peak plasma concentrations, AUC, and other disposition parameters for digoxin was detected in a clinical study involving healthy volunteers. Levofloxacin absorption and disposition kinetics were similar in the presence or absence of digoxin. Therefore, no dosage adjustment for Biopharm Levo (levofloxacin) or digoxin is required when administered concomitantly.
Probenecid and Cimetidine: No significant effect of probenecid or cimetidine on the Cmax of levofloxacin was observed in a clinical study involving healthy volunteers. The AUC and t½ of levofloxacin were higher while CLIF and CLR were lower during concomitant treatment of Biopharm Levo (levofloxacin) with probenecid or cimetidine compared to Biopharm Levo (levofloxacin) alone. However, these changes do not warrant dosage adjustment for Biopharm Levo (levofloxacin) when probenecid or cimetidine is co-administered.
Interactions with Laboratory or Diagnostic Testing: Some fluoroquinolones, including Biopharm Levo (levofloxacin), may produce false-positive urine screening results for opiates using commercially available immunoassay kits. Confirmation of positive opiate screens by more specific methods may be necessary.
Incompatibilities: Biopharm Levo (levofloxacin) Injection should not be co-administered with any solution containing multivalent cations, e.g., magnesium, through the same intravenous line.
Caution: Rapid or bolus intravenous infusion of levofloxacin has been associated with hypotension and must be avoided. Levofloxacin injection should be infused intravenously slowly over a period of 60 or 90 minutes, depending on the dosage. Levofloxacin injection should be administered only by intravenous infusion. It is not for intramuscular, intrathecal, intraperitoneal, or subcutaneous administration.
Biopharm Levo should not be mixed with heparin or alkaline solutions (e.g. sodium hydrogen carbonate).
Biopharm Levo (levofloxacin in 0.9% sodium chloride) Injection is supplied as a single-use, premixed solution in vials. Each vial contains a dilute solution with the equivalent of 250 mg, 500 mg or 750 mg of levofloxacin, respectively, in 0.9% sodium chloride. NO FURTHER DILUTION OF THESE PREPARATIONS IS NECESSARY.
Store this medicine at below 30°C in a hermetic container way from light.
Shelf-Life: 24 months.
Patients should be informed of the following serious adverse reactions that have been associated with Biopharm Levo or other fluoroquinolones use: Tendon Disorders: Patients should contact their healthcare provider if they experience pain, swelling, or inflammation of a tendon, or weakness or inability to use one of their joints; rest and refrain from exercise; and discontinue Biopharm Levo treatment. The risk of severe tendon disorders with fluoroquinolones is higher in older patients usually over 60 years of age, in patients taking corticosteroid drugs, and in patients with kidney, heart or lung transplants.
Hypersensitivity Reactions: Patients should be informed that Biopharm Levo can cause hypersensitivity reactions, even following the first dose. Patients should discontinue the drug at the first sign of a skin rash, hives or other skin reactions, a rapid heartbeat, difficulty in swallowing or breathing, any swelling suggesting angioedema (e.g., swelling of the lips, tongue, face, tightness of the throat, hoarseness), or other symptoms of an allergic reaction.
Hepatotoxicity: Severe hepatotoxicity (including acute hepatitis and fatal events) has been reported in patients taking Biopharm Levo. Patients should inform their physician and be instructed to discontinue Biopharm Levo treatment immediately if they experience any signs or symptoms of liver injury including: loss of appetite, nausea, vomiting, fever, weakness, tiredness, right upper quadrant tenderness, itching, yellowing of the skin and eyes, light colored bowel movements or dark colored urine.
Convulsions: Convulsions have been reported in patients taking fluoroquinolones, including Biopharm Levo. Patients should notify their physician before taking this drug if they have a history of convulsions.
Neurologic Adverse Effects (e.g., dizziness, lightheadedness): Patients should know how they react to Biopharm Levo before they operate an automobile or machinery or engage in other activities requiring mental alertness and coordination.
Diarrhea: Diarrhea is a common problem caused by antibiotics which usually ends when the antibiotic is discontinued. Sometimes after starting treatment with antibiotics, patients can develop watery and bloody stools (with or without stomach cramps and fever) even as late as two or more months after having taken the last dose of the antibiotic. If this occurs, patients should contact their physician as soon as possible.
Peripheral Neuropathies: If symptoms of peripheral neuropathy including pain, burning, tingling, numbness, and/or weakness develop, patients should discontinue treatment and contact their physician.
Prolongation of the QT Interval: Patients should inform their physician of any personal or family history of QT prolongation or proarrhythmic conditions such as hypokalemia, bradycardia, or recent myocardial ischemia; if they are taking any Class IA (quinidine, procainamide), or Class III (amiodarone, sotalol) antiarrhythmic agents. Patients should notify their physicians if they have any symptoms of prolongation of the QT interval, including prolonged heart palpitations or a loss of consciousness.
Musculoskeletal Disorders in Pediatric Patients: Parents should inform their child's physician if their child has a history of jointrelated problems before taking this drug. Parents of pediatric patients should also notify their child's physician of any tendon or joint-related problems that occur during or following Biopharm Levo therapy.
Photosensitivity/Phototoxicity: Patients should be advised that photosensitivity/phototoxicity has been reported in patients receiving fluoroquinolones antibiotics. Patients should minimize or avoid exposure to natural or artificial sunlight (tanning beds or UVA/B treatment) while taking fluoroquinolones. If patients need to be outdoors when taking fluoroquinolones, they should wear loose-fitting clothes that protect skin from sun exposure and discuss other sun protection measures with their physician. If sunburn like reaction or skin eruption occurs, patients should contact their physician.
J01MA12 - levofloxacin ; Belongs to the class of fluoroquinolones. Used in the systemic treatment of infections.
Biopharm Levo inj 750 mg/150 mL
150 mL x 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image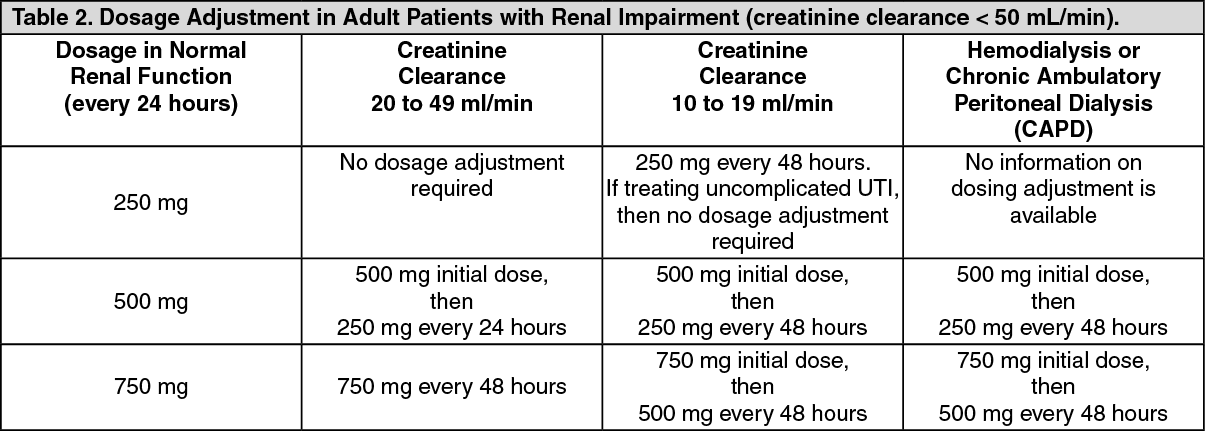 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out