The information highlighted (if any) are the most recent updates for this brand.
Cal-Os & Cal-Os Chew: Calcium carbonate. Cal-Os Plus D: Calcium carbonate, vitamin D3 (cholecalciferol).
Cal-Os: Each capsule contains 350 mg (equivalent to calcium 140 mg) or 835 mg (equivalent to calcium 334 mg).
Each film-coated tablet contains 1,000 mg (equivalent to calcium 400 mg), 1,250 mg (equivalent to calcium 500 mg) or 1,500 mg (equivalent to calcium 600 mg).
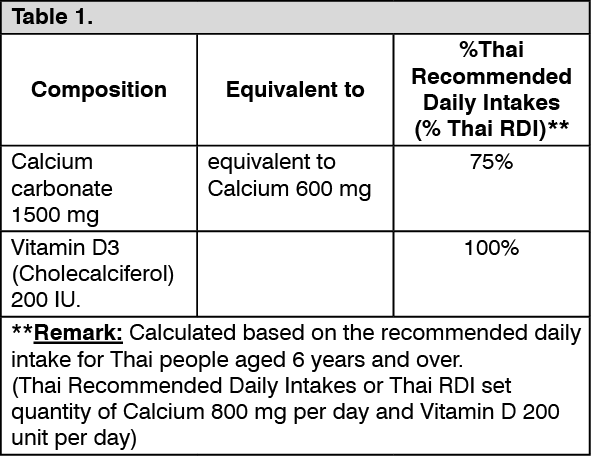
Cal-Os Plus D: Each tablet contains: See Table 1.
 Click on icon to see table/diagram/image
Cal-Os Chew:
Click on icon to see table/diagram/image
Cal-Os Chew: Each tablet contains Calcium carbonate 500 mg equivalent to calcium 200 mg. (See Table 2.)
Click on icon to see table/diagram/image
Pharmacology: Pharmacodynamics: Calcium functions as a regulator in the release and storage of neurotransmitters and hormones, in the uptake and binding of amino acids, and in vitamin B12 absorption and gastrin secretion. Calcium is required to maintain the function of the nervous, muscular, and skeletal systems and cell membrane and capillary permeability. It is an activator in many enzyme reactions and is essential in the transmission of nerve impulses; contraction of cardiac, smooth, and skeletal muscles; respiration; blood coagulation; and renal function.
Calcium more than 99% of total body calcium is found in bone and teeth.
Cal-Os Plus D: Vitamin D3 (Cholecalciferol) maintains serum calcium and phosphate concentrations within normal range by enhancing the efficiency. The small intestine to absorb these minerals from diet.
Pharmacokinetics: Cal-Os Plus D: Absorption and Metabolism: Calcium is absorbed from the GI tract by active transport and passive diffusion. For absorption to occur, calcium must be in a soluble, ionized form. Mean absorption of calcium intake is approximately 25% in adults. Calcium absorption from calcium carbonate is enhanced 10% to 30% by ingestion with a meal. Vitamin D3 (Cholecalciferol), in its activated forms, is required for calcium absorption and increases the capability of the absorptive mechanisms. Vitamin D3 (Cholecalciferol), fat soluble vitamin, is absorbed from small intestine and bile is essential for the absorption process. Vitamin D3 (Cholecalciferol) is incorporated into chylomicrons and reaches the systemic circulation through the lymphatic pathway.
Vitamin D3 (Cholecalciferol) is hydroxylated by the hepatic microsomal enzymes to 25-hydroxy-vitamin D3 (25-[OH]-D3). Further hydroxylation occurs in the kidney to biologically active 1α,25-dihydroxy-vitamin D3 (Calcitriol). Calcitriol stimulate resorption of bone, promote calcium reabsorption by the kidneys and enhances the efficiency of intestinal calcium absorption along the entire small intestine.
Distribution: Normal total serum calcium concentrations range from 9-10.4 mg/dL (4.5 - 5.2 mEq/L). Approximately 45% of the serum calcium is bound to plasma proteins. Cholecalciferol extensively bounds to vitamin D-binding protein (an a-globulin) and is stored in fat and muscles for prolonged periods.
Excretion: Calcium is excreted mainly in the feces and consists of unabsorbed calcium and that secreted via bile and pancreatic juice into the lumen of the GI tract. Only small amount of calcium ion are excreted in urine. Most dose of Cholecalciferol is excreted in the bile and feces. Only a small percentage of a dose of Cholecalciferol is excreted in the urine.
Cal-Os Chew: Calcium carbonate is converted to calcium chloride by gastric acid. Some of the calcium is absorbed from the intestines. Calcium is excreted by the kidneys. Unabsorbed calcium is eliminated with feces.
Calcium carbonate used as a daily source of calcium for prevention of calcium deficiency; treatment of calcium deficiency.
Prevention of calcium deficiency or calcium supplement when calcium intake may be inadequate such as pregnancy, lactation, postmenopause, hypoparathyroidism, vitamin D deficiency person which needs calcium supplement.
Treatment of calcium deficiency such as: Osteoporosis, Osteomalacia, Hypocalcemic rickets.
Cal-Os Plus D: Prevention of calcium deficiency or calcium supplement when calcium intake may be inadequate in children (6 years of age and over), adult, elderly (50 years of age and over).
Treatment and prevention of osteoporosis.
Renal impairment: Patients with creatinine clearance less than 25 mL/minute dosage adjustments may be necessary depending on the serum calcium levels.
Hepatic impairment: The dosage adjustments in patients with hepatic impairment had not been studied.
Cal-Os: 350 mg capsule: 2 capsules 2-3 x daily.
835 mg capsule: 1 capsule 2-3 x daily.
1,000 & 1,250 mg film-coated tablet: 1 tablet twice daily.
1,500 mg film-coated tablet: 1 tablet once daily to twice daily.
Cal-Os Plus D: Cal-OS PLUS D TABLET is administered orally with food will optimized calcium absorption.
Administer 1-2 tablets daily. The doses should be divided so that the patient can take one in the morning and one at night or as directed by physician.
Cal-Os Chew: Mode of Administration: Recommend to chew tablets after meal to enhance absorption. Take with a large glass of water.
Do not use the maximum dosage of this product for more than 2 weeks except under the advice and supervision of a health care provider.
Recommended Dose: For prevention of calcium deficiency or calcium supplement: Thai Recommended Daily Intakes for Thais ages of 6 years and up (Thai RDI) of calcium is 800 mg/day.
Adolescences and Adults dosage: CAL-OS CHEW TABLET 2 tablets twice daily or to be used as directed by the physician.
Children 6-12 years dosage: CAL-OS CHEW TABLET 2 tablets twice daily or to be used as directed by the physician.
For treatment of calcium deficiency: CAL-OS CHEW TABLET 2-3 tablets 2-3 times per day or to be used as directed by the physician.
Cal-Os Plus D: Hypercalcemia may occur when large doses of calcium are administered to patients with chronic renal failure. Mild hypercalcemia may exhibit as nausea, vomiting, anorexia, or constipation, with mental changes such as stupor, delirium, coma, or confusion. Mild hypercalcemia is usually readily controlled by reducing calcium intake (e.g., decreasing the dose of or avoiding supplement Calcium); more severe hypercalcemia may require specific management (e.g., hemodialysis).
Acute or chronic administration of excessive doses of Cholecalciferol may lead to hypervitaminosis D manifested by hypercalcemia. Treatment of Vitamin D analog intoxication consists of withdrawal of both the drug and calcium supplements, maintenance of a low-calcium diet, administration of oral or IV fluids and, if needed, corticosteroids or other drugs, particularly calciuric diuretics (e.g., furosemide and ethacrynic acid) to decrease serum calcium concentration. Hemodialysis or peritoneal dialysis against a calcium free dialysate may also be used. If ingestion is recent, gastric lavage or emesis may prevent further absorption. If the drug has passed through the stomach, administration of mineral oil may promote fecal elimination.
Cal-Os Chew: Symptoms of hypercalcaemia include thirst, polyuria, anorexia, constipation, muscle weakness, fatigue, and confusion. In severe cases, there may be nausea and vomiting; cardiac arrhythmias may develop but are rare. Extreme hypercalcaemia may result in coma and death. Chronic hypercalcaemia can lead to interstitial nephritis and calcium renal calculi. Mild asymptomatic hypercalcemia is best corrected by increasing oral fluid intake. Patients with more severe hypercalcemia, and/or significant symptoms, need prompt treatment by physician.
Cal-Os Plus D: Hypersensitivity to calcium, vitamin D or any component of the formulation.
Patients with hypercalcemia which is caused by sarcoidosis, (sarcoidosis is a chronic multisystemic inflammatory disease related to immune system disorders.), hyperparathyroidism, hypervitaminosis D and certain types of cancer (cancer-induced hypercalcemia e.g. lung cancer, breast cancer and multiple myeloma).
Cal-Os Chew: Do not use in patients with hypercalcemia which is caused by sarcoidosis, (sarcoidosis is a chronic multisystemic inflammatory disease related to immune system disorders), hyperparathyroidism, hypervitaminosis D and certain types of cancer (cancer-induced hypercalcemia e.g. lung cancer, breast cancer and multiple myeloma).
Cal-Os Plus D: The drug accumulation may occur which can be dangerous, avoid overdose or prolonged use, use as directed by the physician.
The total amount of calcium intake from dietary and supplement should not exceed 1,500 mg/day.
Calcium absorption is impaired in achlorhydria; administration of calcium carbonate is followed by increased gastric acid secretion within 2 hours of administration especially with high doses. Common in elderly patients; use an alternate salt (e.g. citrate) and administer with food.
Hypercalcemia may occur when large doses of calcium are administered to patients with chronic renal failure. Mild hypercalcemia may exhibit as nausea, vomiting, anorexia, or constipation, with mental changes such as stupor, delirium, coma, or confusion. By reducing calcium intake, mild hypercalcemia is usually readily controlled. Chronic hypercalcemia may result in vascular calcification and other soft-tissue calcification.
Reduced calcium absorption may occur with calcium carbonate administration without food.
Use caution when administering calcium to patients with a history of kidney stones.
The milk-alkali syndrome of hypercalcemia, alkalosis and renal impairment may occur in patients who take large amounts of calcium and absorbable alkali.
Hypercalcemia may increase risk of cardiac arrythmias and seizures.
Cal-Os Chew: The major limiting factor to the chronic use of Calcium carbonate is gastric hypersecretion and acid rebound. Calcium carbonate may cause the milk-alkaline syndrome. Patient with renal impairment or dehydration and electrolyte imbalance are predisposed to developing the milk-alkaline syndrome. Serum calcium concentrations should be monitored weekly in patients receiving large dosages of Calcium carbonate.
Cal-Os Plus D: Pregnancy: Calcium crosses the placenta. The amount of calcium reaching the fetus is determined by maternal physiological changes. Calcium requirements are the same in pregnant and nonpregnant females. Fetal harm is not expected if maternal calcium concentrations are monitored and maintained. Vitamin D crosses the placenta but the transfer to the fetus from the mother is low. Maternal supplementation has not been shown to affect pregnancy outcomes. Vitamin D requirements are the same in pregnant and nonpregnant females. The daily intake should not exceed 1,500 mg of calcium and 600 IU of Vitamin D in pregnancy.
Lactation: Calcium is excreted in breast milk. The amount of calcium in breast milk is not altered by maternal calcium intake. Calcium requirements are the same in lactating and nonlactating females. Maternal vitamin D requirements are the same for breast-feeding and non-breast feeding women. However, the amount of vitamin D in breast milk does not correlate with serum concentrations in the infant. This drug poses minimal risk to the infant when used during breastfeeding.
Cal-Os Chew: The dietary reference intakes for calcium carbonate chewable tablets in pregnant or lactating females are the same as in nonpregnant or nonlactating females.
Common: Gastrointestinal system: constipation, flatulence (from released carbon dioxide), swollen abdomen, nausea, loss of appetite.
High doses or prolonged use may lead to gastric hypersecretion and acid rebound.
May occur: Central nervous system: headache.
Cardiovascular system: myocardial infarction.
Endocrine and metabolic system: hypercalcaemia (particularly in patients with renal impairments or after high dose), hypervitaminosis D (signs and symptoms include hypercalcaemia, resulting in headache, nausea, vomiting, lethargy, confusion, sluggishness, abdominal pain, bone pain, polyuria, polydipsia, weakness, cardiac arrhythmias [e.g. QT shortening, sinus tachycardia], soft tissue calcification, calciuria, and nephrocalcinosis).
Gastrointestinal system: abdominal pain, gastric hypersecretion and acid rebound (high doses or prolonged use).
Genitourinary system: hypercalciuria, urolithiasis, prostate cancer.
Miscellaneous: milk-alkaline syndrome, alkalosis (may also occur as a result of the carbonate anion).
Calcium salts interact with many other drugs both by alterations in gastric pH and emptying, and by formation of complexes that are not absorbed. Interactions can be minimized by giving Calcium carbonate and any other medication 2 to 3 hours (for Cal-Os Plus D) or 4 hours (for Cal-Os Chew) apart.
Bisphosphonates: Concomitant administration of calcium salts with bisphosphonates (e.g., alendronate, etidronate, ibandronate, risedronate) may reduce absorption of the bisphosphonate from the GI tract. To minimize this effect, the drug should be administered at separate times (for Cal-Os Plus D) or at least 2 hours after bisphosphonates administration (for Cal-Os Chew).
Cardiac Glycosides: The inotropic and toxic effect of cardiac glycosides and calcium are synergistic and arrhythmias may occur if these drugs are given together.
Iron preparations: Concomitant administration of calcium salts and oral iron preparations may result in reduced absorption of iron. Patients should be advised to take the drugs at different times, whenever possible.
Levothyroxine: Calcium carbonate may form an insoluble chelate with levothyroxine, resulting in decreased levothyroxine absorption and increased serum thyrotropin (thyroid stimulating hormone) concentrations. To minimize or prevent this interaction, oral levothyroxine sodium should be administered at least 4 hours apart from Calcium carbonate.
Quinolones: Concomitant administration of calcium salts and some fluoroquinolones (e.g., ciprofloxacin) may reduce oral bioavailability of the fluoroquinolone.
Tetracyclines: Calcium complexes tetracycline antibiotics rendering them inactive; the two drugs should not be given at the same time orally.
Cal-Os Plus D: Cholestyramine or colestipol hydrochloride: Cholestyramine or colestipol hydrochloride administration may result in decreased intestinal absorption of vitamin D analogs; patients taking cholestyramine or colestipol hydrochloride should be instructed to allow as long a time interval as possible between the ingestion of vitamin D analogs and the resin.
Orlistat: Orlistat may result in decreased GI absorption of vitamin D analogs. At least 2 hours should elapse between (before or after) any orlistat dose and vitamin D analog administration.
Mineral oil: Mineral oil may interfere with intestinal absorption of vitamin D analogs. Patients taking mineral oil should be instructed to allow as long a time interval as possible between the ingestion of vitamin D analogs and mineral oil.
Drugs that inhibit cytochrome P-450 enzymes: Drugs that inhibit CYP enzymes (e.g., atazanavir, clarithromycin, indinavir, itraconazole, ketoconazole, nefazodone, nelfinavir, ritonavir, saquinavir, telithromycin, voriconazole) may inhibit CYP27B1, which metabolizes calcifediol to its activated form (1,25-dihydroxycholecalciferol [calcitriol]), and CYP24A1, which metabolizes both calcifediol and 1,25-dihydroxycholecalciferol to inactive metabolites, thereby altering serum calcifediol concentrations.
Drugs that induce hepatic microsomal enzymes: Administration of anticonvulsants ( e.g., carbamazepine, phenobarbital, phenytoin) and other drugs that induce hepatic microsomal hydroxylation may decrease plasma concentrations of 25-hydroxylated ergocalciferol and 25- hydroxylated cholecalciferol (calcifediol) and increase metabolism of the vitamins to inactive metabolites. Dosage adjustment of vitamin D analogs may be required. Serum concentrations of total 25-hydroxyvitamin D, iPTH, and calcium should be monitored in patients receiving calcifediol when concomitant therapy with anticonvulsants or other drugs that stimulate microsomal hydroxylation is initiated or discontinued.
Thiazide diuretics: Concurrent administration of thiazide diuretics and pharmacologic doses of vitamin D analogs in patients with hypoparathyroidism may result in hypercalcemia which may be transient and self-limited or may require discontinuance of vitamin D analogs. Thiazide-induced hypercalcemia in hypoparathyroid patients is probably caused by increased release of calcium from bone. Thiazide diuretics also can induce hypercalcemia by decreasing renal calcium excretion. More frequent monitoring of serum calcium concentrations may be required in patients with secondary hyperparathyroidism and chronic kidney disease receiving such concomitant therapy.
Corticosteroids: Corticosteroids counteract the effects of vitamin D analogs.
Cardiac glycosides: Concurrent use of vitamin D analogs and cardiac glycosides may result in cardiac arrhythmias.
A12AA04 - calcium carbonate ; Belongs to the class of calcium-containing preparations. Used as dietary supplements.
A12AX - Calcium, combinations with vitamin D and/or other drugs ; Used as dietary supplements.
Cal-Os cap 350 mg
10 × 10's
Cal-Os cap 835 mg
10 × 10's
Cal-Os Chew chewable tab 500 mg
14's;30's;60's
Cal-Os FC tab 1,000 mg
10 × 10's
Cal-Os FC tab 1,250 mg
10 × 10's
Cal-Os FC tab 1,500 mg
10 × 10's
Cal-Os Plus D FC tab
10 × 10's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image







 Sign Out
Sign Out