Each capsule contains Celecoxcib 400 mg.
Celecoxib is chemically designated as 4-[5-(4-methylphenyl)-3-(trifluoromethyl)-1H-pyrazol-1-yl] benzenesulfonamide and is a diaryl-substituted pyrazole. The empirical formula is C17H14F3N3O2S, and the molecular weight is 381.38.
Excipients/Inactive Ingredients: croscarmellose sodium, edible inks, gelatin, lactose monohydrate, magnesium stearate, povidone and sodium lauryl sulfate.
Pharmacology: Pharmacodynamics: Mechanism of Action: Celecoxib is a nonsteroidal anti-inflammatory drug that exhibits anti-inflammatory, analgesic, and antipyretic activities in animal models. The mechanism of action of Celecoxib is believed to be due to inhibition of prostaglandin synthesis, primarily via inhibition of cyclooxygenase-2 (COX-2), and at therapeutic concentrations in humans, Celecoxib does not inhibit the cyclooxygenase-1 (COX-1) isoenzyme.
Pharmacokinetics: Absorption: Peak plasma levels of celecoxib occur approximately 3 hrs after an oral dose. Under fasting conditions, both peak plasma levels (Cmax) and area under the curve (AUC) are roughly dose-proportional up to 200 mg BID; at higher doses there are less than proportional increases in Cmax and AUC. Absolute bioavailability studies have not been conducted. With multiple dosing, steady-state conditions are reached on or before Day 5.
Food Effects: When Celecoxib capsules were taken with a high fat meal, peak plasma levels were delayed for about 1 to 2 hours with an increase in total absorption (AUC) of 10% to 20%. Under fasting conditions, at doses above 200 mg, there is less than a proportional increase in Cmax and AUC, which is thought to be due to the low solubility of the drug in aqueous media.
Coadministration of Celecoxib with an aluminum- and magnesium-containing antacids resulted in a reduction in plasma celecoxib concentrations with a decrease of 37% in Cmax and 10% in AUC. Celecoxib, at doses up to 200 mg twice daily, can be administered without regard to timing of meals. Higher doses (400 mg twice daily) should be administered with food to improve absorption. In healthy adult volunteers, the overall systemic exposure (AUC) of celecoxib was equivalent when celecoxib was administered as intact capsule or capsule contents sprinkled on applesauce. There were no significant alterations in Cmax, Tmax or t½ after administration of capsule contents on applesauce.
Distribution: In healthy subjects, celecoxib is highly protein bound (˜97%) within the clinical dose range. In vitro studies indicate that celecoxib binds primarily to albumin and, to a lesser extent, ἀ1-acid glycoprotein. The apparent volume of distribution at steady state (Vss/F) is approximately 400 L, suggesting extensive distribution into the tissues. Celecoxib is not preferentially bound to red blood cells.
Metabolism: Celecoxib metabolism is primarily mediated via CYP2C9. Three metabolites, a primary alcohol, the corresponding carboxylic acid and its glucuronide conjugate, have been identified in human plasma. These metabolites are inactive as COX-1 or COX-2 inhibitors.
Excretion: Celecoxib is eliminated predominantly by hepatic metabolism with little (<3%) unchanged dreg recovered in the urine and feces. Following a single oral dose of radiolabeled drug, approximately 57% of the dose was excreted in the feces and 27% was excreted into the urine. The primary metabolite in both urine and feces was the carboxylic acid metabolite (73% of dose) with low amounts of the glucuronide also appearing in the urine. It appears that the low solubility of the drug prolongs the absorption process making terminal half-life (t½) determinations more variable. The effective half-life is approximately 11 hours under fasted conditions. The apparent plasma clearance (CL/F) is about 500 mL/min.
Carefully consider the potential benefits and risks of Celecoxib and other treatment options before deciding to use Celecoxib. Use the lowest effective dose for the shortest duration consistent with individual patient treatment goals.
Osteoarthritis (OA): Celecoxib is indicated for relief of the signs and symptoms of OA.
Rheumatoid Arthritis (RA): Celecoxib is indicated for relief of the signs and symptoms of RA.
Juvenile Rheumatoid Arthritis (JRA): Celecoxib is indicated for relief of the signs and symptoms of JRA in patients 2 years and older.
Ankylosing Spondylitis (AS): Celecoxib is indicated for the relief of signs and symptoms of AS.
Colorectal Polyps: Celecoxib is used to reduce the number of adenomatous colorectal polys in adults with familial adenomatous polyposis (FAP).
Acute Pain (AP): Celecoxib is indicated for the management of AP in adults.
Primary Dysmenorrhea (PD): Celecoxib is indicated for the treatment of PD.
Use lowest effective dose for the shortest duration consistent with treatment goals for the individual patient. These doses can be given without regard to timing of meals.
Osteoarthritis: For relief of the signs and symptoms of OA the recommended oral dose is 200 mg per day administered as a single dose or as 100 mg twice daily.
Rheumatoid Arthritis: For relief of the signs and symptoms of RA the recommended oral dose is 100 to 200 mg twice daily.
Juvenile Rheumatoid Arthritis: For the relief of the signs and symptom of JRA the recommended oral dose for pediatric patients (age 2 years and older) is based on weight. For patients ≥ 25 kg the recommended dose is 100 mg twice daily.
Ankylosing Spondylitis: For the management of the signs and symptoms of AS, the recommended dose of Celecoxib is 200 mg daily in single (once per day) or divided (twice per day) doses. If on effect is observed after 6 weeks, a trial of 400 mg daily may be worthwhile. If no effect is observed after 6 weeks on 400 mg daily, a response is not likely and consideration should be given to alternate treatment options.
Colorectal Polyps: Celecoxib is used to reduce the number of adenomatous colorectal polys in adults with familial adenomatous polyposis (FAP) as an adjunct to usual care. Celecoxib should be given in a dosage of 400 mg twice daily.
Management of Acute Pain and Treatment of Primary Dysmenorrhea: The recommended dose of Celecoxib is 400 mg initially, followed by an additional 200 mg dose if needed on the first day. On subsequent days, the recommended dose is 200 mg twice daily as needed.
No overdoses of Celecoxib were reported during clinical trials. Doses up to 2400 mg/day for up to 10 days in 12 patients did not result in serious toxicity. Symptoms following acute NSAID overdoses are usually limited to lethargy, drowsiness, nausea, vomiting, and epigastric pain, which are generally reversible with supportive care. Gastrointestinal bleeding can occur. Hypertension, acute renal failure, respiratory depression and coma may occur, but are rare. Anaphylactoid reactions have been reported with therapeutic ingestion of NSAIDs, and may occur following an overdose. Patients should be managed by symptomatic and supportive care following and NSAID overdose. There are no specific antidotes. No information is available regarding the removal of celecoxib by hemodialysis, but based on its high degree of plasma protein binding (>97%) dialysis is unlikely to be useful in overdose. Emesis and/or activated charcoal (60 to 100 g in adults, 1 to 2 g/kg in children) and/or osmotic cathartic may be indicated in patients seen within 4 hours of ingestion with symptoms or following a large overdose. Forced diuresis, alkalinization of urine, hemodialysis, or hemoperfusion may not be useful due to high protein binding.
Celecoxib is contraindicated: In patients with known hypersensitivity to celecoxib, aspirin, or other NSAIDs.
In patients who have demonstrated allergic-type reactions to sulfonamides.
In patients who have experienced asthma, urticarial, or allergic-type reactions after taking aspirin or other NSAIDs. Severe anaphylactoid reactions to NSAIDs, some of them fatal, have been reported in such patients.
For the treatment of peri-operative pain in the setting of coronary artery bypass graft (CABG) surgery.
Cardiovascular Thrombotic Events: Chronic use of Celecoxib may cause an increased risk of serious adverse cardiovascular thrombotic events, myocardial infarction, and stroke, which can be fatal. All NSAIDs, both COX-2 selective and non-selective, may have a similar risk. Patients with known CV disease or risk factors for CV disease may be at greater risk. To minimize the potential risk for an adverse CV event in patients treated with Celecoxib, the lowest effective dose should be used for the shortest duration consistent with individual patient treatment goals. Physicians and patients should remain alert for the development of such events, even in the absence of previous CV symptoms. Patients should be informed about the signs and/or symptoms of serious CV toxicity and the steps to take if they occur. There is no consistent evidence that concurrent use of aspirin mitigates the increased risk of serious CV thrombotic events associated with NSAID use. The concurrent use of aspirin and Celecoxib dose increase the risk of serious GI.
Hypertension: As with all NSAIDs, Celecoxib can lead to the onset of new hypertension or worsening of preexisting hypertension, either of which may contribute to the increased incidence of CV events. Patients taking thiazides or loop diuretics may have impaired response to these therapies when taking NSAIDs. NSAIDs, including Celecoxib, should be used with caution in patients with hypertension. Blood pressure should be monitored closely during the initiation of therapy with Celecoxib and throughout the course of therapy.
Congestive Heart Failure and Edema: Fluid retention and edema have been observed in some patients taking NSAIDs, including Celecoxib. Celecoxib should be used with caution in patients with fluid retention or heart failure.
Gastrointestinal (GI) Effects: Risk of GI Ulceration, Bleeding, and Perforation: NSAIDs, including Celecoxib, can cause serious gastrointestinal events including bleeding ulceration, and perforation of the stomach, small intestine or large intestine, which can be fatal. These serious adverse events can occur at any time, with or without warning symptoms, in patients treated with NSAIDs. With longer duration of use of NSAIDs, there is a trend for increasing the likelihood of developing a serious GI event at some time during the course of therapy. However, even short-term therapy is not without risk.
NSAIDs should be prescribed with extreme caution in patients with a prior history of ulcer disease or gastrointestinal bleeding. Patients with a prior history of peptic ulcer disease and /or gastrointestinal bleeding who use NSAIDs have a greater than 10-fold increased risk for developing a GI bleed compared to patients with neither of these risk factors. Other factors that increase the risk of GI bleeding in patients treated with NSAIDs include concomitant use of oral corticosteroids or anticoagulants, longer duration of NSAID therapy, smoking, use of alcohol, older age, and poor general health status. Most spontaneous reports of fatal GI events are in elderly or debilitated patients and therefore special care should be taken in treating this population.
To minimize the potential risk for an adverse GI event the lowest effective dose should be used for the shortest duration consistent with individual patient treatment goals. Physicians and patients should remain alert for signs and symptoms of GI ulceration and bleeding during Celecoxib therapy and promptly initiate additional evaluation and treatment if a serious GI adverse event is suspected. For high-risk patients, alternate therapies that do not involve NSAIDs should be considered.
Hepatic Effects: Borderline elevations of one or more liver-associated enzymes may occur in up to 15% of patients taking NSAIDs, and notable elevations of ALT or AST (approximately 3 or more times the upper limit of normal) have been reported in approximately 1% of patients in clinical trials with NSAIDs. These laboratory abnormalities may progress, may remain unchanged, or may be transient with continuing therapy. Rare cases of severe hepatic reactions, including jaundice and fatal fulminant hepatitis, liver necrosis and hepatic failure (some with fatal outcome) have been reported with NSAIDs, including Celecoxib. A patient with symptoms and/or signs suggesting liver dysfunction, or in whom an abnormal liver test has occurred, should be monitored carefully for evidence of the development of a more severe hepatic reaction while on therapy with Celecoxib. If clinical signs and symptoms consistent with liver disease develop, or if systemic manifestations occur (e.g., eosinophilia, rash, etc.), Celecoxib should be discontinued.
Anaphylactoid Reactions: As with NSAIDs in general, anaphylactoid reactions have occurred in patients without known prior exposure to Celecoxib. In post-marketing experience, rare cases of anaphylactic reactions and angioedema have been reported in patients receiving Celecoxib. Celecoxib should not be given to patients with the aspirin triad. This symptom complex typically occurs in asthmatic patients who experience rhinitis with or without nasal polyps, or who exhibit severe, potentially fatal bronchospasm after taking aspirin or other NSAIDs. Emergency help should be sought in cases where an anaphylactoid reaction occurs.
Skin Reactions: Celecoxib is a sulfonamide and can cause serious skin adverse events such as exfoliative dermatitis, Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN), which can be fatal. These serious events can occur without warning and in patients without prior known sulfa allergy. Patients should be informed about the signs and symptoms of serious skin manifestations and use of the drug should be discontinued at the first appearance of skin rash or any other sign of hypersensitivity.
Corticosteroid Treatment: Celecoxib cannot be expected to substitute for corticosteroids or to treat corticosteroid insufficiency. Abrupt discontinuation of corticosteroids may lead to exacerbation of corticosteroid-responsive illness. Patients on prolonged corticosteroid therapy should have their therapy tapered slowly if a decision is made to discontinue corticosteroids.
Hematological Effects: Anemia is sometimes seen in patients receiving Celecoxib. In controlled clinical trials the incidence of anemia was 0.6% with Celecoxib and 0.4% WITH PLACEBO. Patients on long-term treatment with Celecoxib should have their hemoglobin or hematocrit checked if they exhibit any signs or symptoms of anemia or blood loss. Celecoxib does not generally affect platelet counts, prothrombin time (PT), or partial thromboplastin time (PTT), and does not inhibit platelet aggregation at indicated dosages.
Disseminated Intravascular Coagulation (DIC): Celecoxib should be used only with caution in pediatric patients with systemic onset JRA due to the risk of disseminated intravascular coagulation.
Preexisting Asthma: Patients with asthma may have aspirin-sensitive asthma. The use of aspirin in patients with aspirin-sensitive asthma has been associated with severe bronchospasm, which can be fatal. Since cross reactivity, including bronchospasm, between aspirin and other nonsteroidal anti-inflammatory drugs has been reported in such aspirin-sensitive patients, Celecoxib should be used with caution in patients with preexisting asthma.
Laboratory Tests: Because serious GI tract ulcerations and bleeding can occur without warning symptoms, physicians should monitor for signs or symptoms of GI bleeding. Patients on long-term treatment with NSAIDs should have a CBC and a chemistry profile checked periodically. If abnormal liver tests or renal tests persist or worsen, Celecoxib should be discontinued.
In controlled clinical trials, elevated BUN occurred more frequently in patients receiving Celecoxib compared with patients on placebo. This laboratory abnormality was also seen in patients who received comparator NSAIDs in these studies. The clinical significance of this abnormality has not been established.
Inflammation: The pharmacological activity of Celecoxib in reducing inflammation, and possibly fever, may diminish the utility of these diagnostic signs in detecting infections complications of presumed noninfectious, painful conditions.
Concomitant NSAID Use: The concomitant use of Celecoxib with any dose of non-aspirin NSAID should be avoided due to the potential for increased risk of adverse reactions.
Hepatic insufficiency: The daily recommended dose of celecoxib capsules in patients with moderate hepatic impairment (Child-Pugh Class B) should be reduced by 50%. The use of celecoxib in patients with severe hepatic impairment is not recommended.
Poor Metabolizers of CYP2C9 Substrates: Patients who are known or suspected to be poor CYP2C9 metabolizers based on genotype or previous history/experience with other CYP2C9 substrates (such as warfarin, phenytoin) should be administered celecoxib with caution. Consider starting treatment at half the lowest recommended dose in poor metabolizers (i.e. CYP2C9*3/*3). Consider using alternative management in JRA patients who are poor metabolizers.
Use in Pregnancy: In late pregnancy, starting at 30 weeks gestation, Celecoxib should be avoided because it may cause premature closure of the ductus arteriosus.
Pregnancy: Pregnancy Category C. Pregnancy category D from 30 weeks of gestation onward.
Teratogenic effects: Celecoxib at oral doses ≥150 mg/kg/day (approximately 2-fold human exposure at 200 mg twice daily as measured by AUC0-24 ), caused an increased incidence of ventricular septal defects, a rare event, and fetal alterations, such as ribs fused, sternebral fused and sternebrae misshapen when rabbits were treated throughout organogenesis. A dose-dependent increase in diaphragmatic hernias was observed when rats were given celecoxib at oral doses ≥ 30 mg/kg/day approximately 6-fold human exposure based on the AUC0-24 at 200 mg twice daily) throughout organogenesis. There are no studies in pregnant women. Celecoxib should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Nonteratogenic effects: Celecoxib produced pre-implantation and post-implantation losses and reduced embryo/fetal survival in rats at oral dosages ≥50 mg/kg/day (approximately 6-fold human exposure based on the AUC0-24 at 200 mg twice daily). These changes are expected with inhibition of prostaglandin synthesis and are not the result of permanent alteration of female reproductive function, nor are they expected at clinical exposures. No studies have been conducted to evaluate the effect of celecoxib on the closure of the ductus arteriosus in humans. Therefore, use of Celecoxib during the third trimester of pregnancy should be avoided.
Labor and Delivery: Celecoxib produced no evidence of delayed labor or parturition at oral doses up to 100 mg/kg in rats (approximately 7-fold human exposure as measured by the AUC 0-24 at 200 mg BID). The effects of Celecoxib on labor and delivery in pregnant women are unknown.
Nursing Mothers: Limited data from 3 published reports that included a total of 12 breastfeeding women showed low levels of Celecoxib in breast milk. The calculated average daily infant dose was 10-40 mcg/kg/day, less than 1% of the weight-based therapeutic dose for a two-year old-child. A report of two breastfed infants 17 and 22 months of age did not show any adverse events. Caution should be exercised when Celecoxib is administered to a nursing woman.
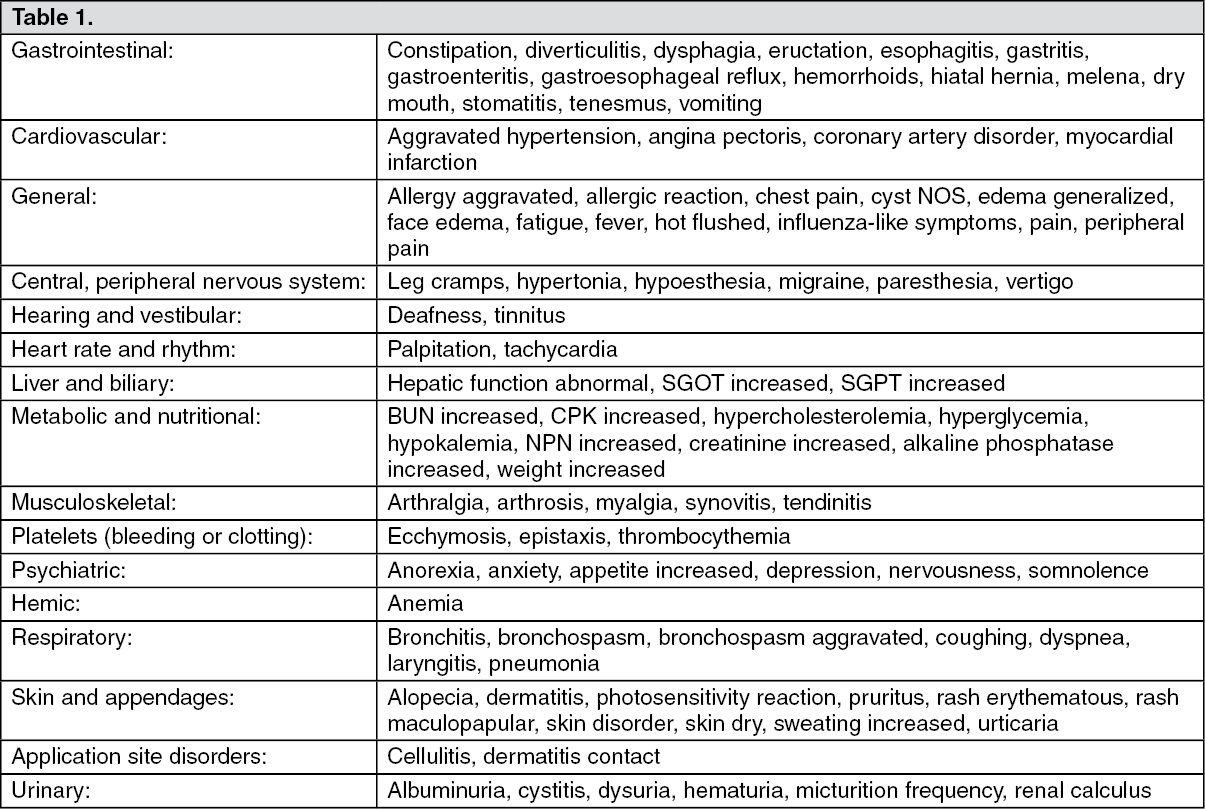
The following adverse reactions occurred in 0.1-1.9% of patients treated with Celecoxib (100-200 mg twice daily or 200 mg once daily). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The following serious adverse events (causality not evaluated) occurred in <0.1% of patients (cases reported only in post-marketing experience are indicated in italics). (See Table 2.)
Click on icon to see table/diagram/image
General: Celecoxib metabolism is predominantly mediated via cytochrome P450 (CYP)2C9 in the liver. Co-administration of celecoxib with drugs that are known to inhibit CYP2C9 should be done with caution. Significant interactions may occur when celecoxib is administered together with drugs that inhibit CYP2C9.
Warfarin: Anticoagulant activity should be monitored, particularly in the first few days, after initiating or changing Celecoxib therapy in patients receiving warfarin or similar agents, since these patients are at an increased risk of bleeding complications. The effect of celecoxib on anticoagulant effect of warfarin was studied in a group of healthy subjects receiving daily 2-5 mg doses of warfarin. In these subjects, celecoxib did not alter the anticoagulant effect of warfarin as determined by prothrombin time. However, in post-marketing experience, serious bleeding events, some of which were fatal, have been reported, predominantly in the elderly, in association with increases in prothrombin time tin patients receiving Celecoxib concurrently with warfarin.
Lithium: In a study conducted in healthy subjects, mean steady-state lithium plasma levels increased approximately 17% in subjects receiving lithium 450 mg twice daily with Celecoxib 200 mg twice daily as compared to subjects receiving lithium alone. Patients on lithium treatment should be closely monitored when Celecoxib is introduced or withdrawn.
Aspirin: Celecoxib can be used with low-dose aspirin. However, concomitant administration of aspirin with Celecoxib increases the rate of GI ulceration or other complications, compared to use of Celecoxib alone. Because of its lack of platelet effects, Celecoxib is not a substitute for aspirin for cardiovascular prophylaxis.
ACE-inhibitors and Angiotensin II Antagonists: Reports suggest that NSAIDs may diminish the antihypertensive effect of Angiotensin Converting Enzyme (ACE) inhibitors and angiotensin II antagonists. This interaction should be given consideration in patients taking Celecoxib concomitantly with ACE-inhibitors and angiotensin II antagonists.
In patients who are elderly, volume-depleted (including those on diuretic therapy), or with compromised renal function, co-administration of NSAIDs, including selective COX-2 inhibitors, may result in deterioration of renal function, including possible acute renal failure. Discontinuation of NSAID therapy is usually followed by recovery to the pretreatment state.
Fluconazole: Concomitant administration of fluconazole at 200 mg once daily resulted in a two-fold increase in celecoxib plasma concentration. This increase is due to the inhibition of celecoxib metabolism via P450 2C9 by fluconazole. Celecoxib should be introduced at the lowest recommended dose in patients receiving fluconazole.
Furosemide: Clinical studies, as well as post-marketing observations, have shown that NSAIDs can reduce the natriuretic effect of furosemide and thiazides in some patients. This response has been attributed to inhibition of renal prostaglandin synthesis.
Methotrexate: In an interaction study of rheumatoid arthritis patients taking methotrexate, Celecoxib did not have an effect on the pharmacokinetics of methotrexate.
Concomitant NSAID Use: The concomitant use of Celecoxib with any dose of a non-aspirin NSAID should be avoided due to the potential for increased risk of adverse reactions.
Protect from light and moisture.
Store below 30°C in a dry place.
M01AH01 - celecoxib ; Belongs to the class of non-steroidal antiinflammatory and antirheumatic products, coxibs.
Cecoxza 400 cap 400 mg
6 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image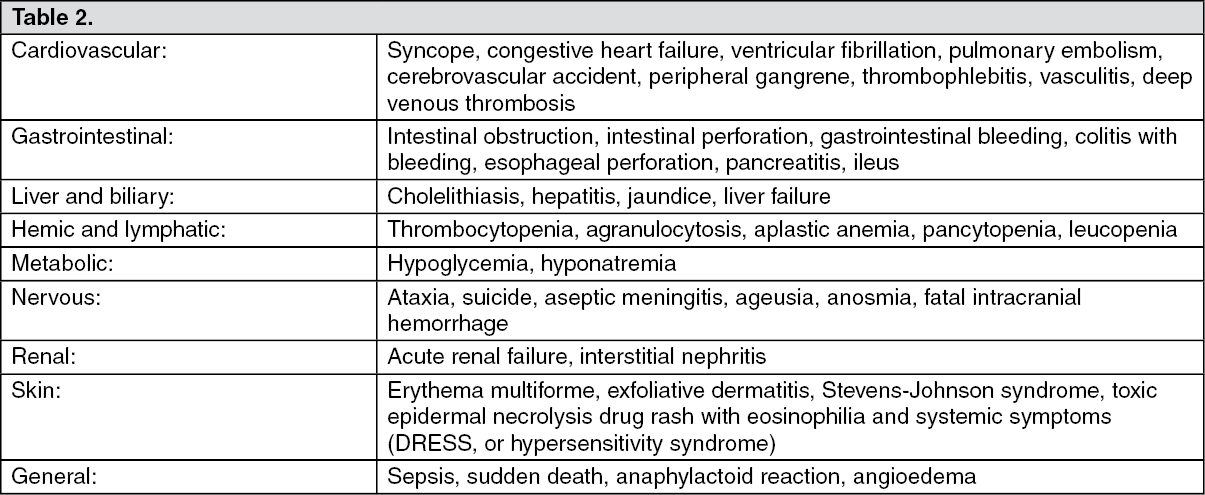 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out