The following adverse reactions have been reported in clinical studies and post marketing experience. The incidence identified below reflects exposure to 500 mg tablet of levofloxacin in total of 1,930 patients in pooled Phase 3 and Phase 4 clinical trials (e.g., 1,582 patients from Phase 3 clinical trials conducted in Japan (337 patients) and China (1,245 patients) and 348 patients from Phase 4 clinical trials) or 29,880 patients in a post marketing studies conducted in Japan. If the incidence category of an adverse reaction is different between each source (i.e., the incidence from the pooled clinical trials and the incidence from the post marketing study), the higher frequency is represented.
The following CIOMS frequency rating is used: Very common: 10% ≤ incidence; Common: 1% ≤ incidence < 10%; Uncommon: 0.1% ≤ incidence < 1%; Rare: 0.01% ≤ incidence < 0.1%; Very rare: incidence <0.01%.
*: see SERIOUS ADVERSE REACTIONS in the following text, each incidence is based on serious reactions.
Blood and lymphatic system disorders: Common: anemia.
Very rare: thrombocytopenia*.
Incidence unknown: pancytopenia*, agranulocytosis*, hemolytic anemia with hemoglobinuria*.
Immune system disorder: Incidence unknown: anaphylactoid reaction*.
Metabolism and nutrition disorder: Uncommon: anorexia.
Incidence unknown: hypoglycemia (hypoglycemic coma may occur)*, hyperglycemia*.
Psychiatric disorders: Common: sleep loss.
Rare: hallucination.
Incidence unknown: psychiatric symptoms such as confusion*, delirium*, depression*.
Nervous system disorders: Common: dizziness /vertigo, headache.
Uncommon: somnolence, numbness, tremor, mental dullness, dysgeusia.
Rare: consciousness disturbed.
Very rare: convulsion*, ageusia.
Incidence unknown: peripheral nerve disorder, extrapyramidal disorder, anosmia, parosmia.
Eye disorders: Rare: abnormal vision.
Ear and labyrinth disorders: Uncommon: tinnitus.
Incidence unknown: hearing losses.
Cardiac disorders: Uncommon: palpitations.
Incidence unknown: ventricular tachycardia (including Torsades de pointes)*, QT prolonged*, tachycardia.
Vascular disorders: Very rare: shock*.
Incidence unknown: hypotension.
Respiratory, thoracic and mediastinal disorders: Uncommon: dry throat.
Incidence unknown: interstitial pneumonia*, eosinophilic pneumonia*.
Gastrointestinal disorders: Common: nausea, vomiting, diarrhea, abdominal discomfort, constipation.
Uncommon: abdominal pain, dyspepsia, abdominal distension, constipation.
Rare: stomatitis.
Very rare: glossitis.
Incidence unknown: colitis with bloody stool, such as pseudomembranous colitis*.
Hepatobiliary disorders: Uncommon: hepatic function abnormal (severe hepatic function disorder* may rarely occur).
Incidence unknown: hepatitis fulminant*, jaundice*.
Skin and subcutaneous tissue disorders: Uncommon: pruritus, rash.
Rare: hyperhidrosis, urticaria.
Very rare: photosensitivity.
Incidence unknown: toxic epidermal necrolysis (TEN)*, oculomucocutaneous syndrome (Stevens-Johnson syndrome) *, hypersensitivity vasculitis*.
Musculoskeletal and connective tissue disorders: Uncommon: arthralgia, pain in extremity, back pain, weakness.
Rare: arthropathy, myalgia.
Incidence unknown: rhabdomyolysis*, tendon disorders such as Achilles tendonitis or tendon rupture*, exacerbation of myasthenia gravis *, muscle rupture.
Renal and urinary disorders: Uncommon: hematuria, urinary retention.
Rare: pollakiuria, oliguria, acute renal failure*.
Incidence unknown: interstitial nephritis*, anuria, dysuria.
General disorders and administration site conditions: Very common
#:
infusion site reaction (erythema, pruritus, swelling, pain, induration, warmth, discomfort, phlebitis, vasculitis, angiopathy, puncture site pain).
#: The incidence of the relevant event is based on data from Japan clinical studies in 586 patients intravenously treated with levofloxacin.
Uncommon: thirst, chest discomfort, malaise, feeling hot, edema.
Very rare:
#pyrexia.
Incidence unknown: chest pain.
Investigations: Common: AST increased, ALT increased, LDH increased, white blood cell count decreased, eosinophil count increased.
Uncommon: creatinine increased, urinary protein positive, alkaline phosphatase increased, γ-GTP increased, blood bilirubin increased, lymphocyte count decreased, neutrophil count decreased, CPK increased, glucose urine present, blood glucose decreased, platelet count decreased.
Rare: BUN increased, urine output decreased.
Very rare: blood glucose increased.
The events of which frequency category observed in Japanese clinical studies in 586 patients and post-marketing study in 1138 patients intravenously treated with levofloxacin is higher than the rating shown in this section is listed as follows.
Psychiatric disorders: Uncommon: hallucination.
Respiratory, thoracic and mediastinal disorders: Uncommon: interstitial pneumonia*.
Gastrointestinal disorders: Common: constipation; Uncommon: glossitis.
Hepatobiliary disorders: Common: hepatic function abnormal (severe hepatic function disorder* may uncommon occur).
Musculoskeletal and connective tissue disorders: Uncommon: myalgia.
General disorders and administration site conditions: Uncommon: pyrexia.
Investigations: Common: γ-GTP increased, alkaline phosphatase increased.
Serious Adverse Reaction: The following serious adverse reactions have been reported in patients receiving therapy with levofloxacin. If the following reactions are suspected, treatment with levofloxacin should be discontinued immediately and appropriate therapeutic measure should be taken: Shock or anaphylactoid reaction (initial symptoms: erythema, rigor, dyspnea, etc.).
Toxic epidermal necrolysis (TEN) or oculomucocutaneous syndrome (Stevens-Johnson syndrome).
Convulsion.
QT prolonged and ventricular tarchycardia (including Torsades de pointes): During post-marketing surveillance, prolonged QT which may sometimes lead to the occurrence of ventricular tachycardia including torsades de pointes have been reported spontaneously in patients taking levofloxacin. The risk of the events may be increased in patients with serious heart diseases (e.g. arrhythmia and ischemic heart disease), patients with uncorrected hypokalemia, patients receiving Class IA (quinidine sulfate, procainamide hydrochloride) and Class III (amiodarone hydrochloride, sotalol hydrochloride) antiarrhythmic agents and in geriatric patients.
Acute renal failure or interstitial nephritis.
Hepatitis fulminant, hepatic function disorder or jaundice (initial symptoms: nausea, vomiting, anorexia, malaise, pruritus, etc.)
Pancytopenia, agranulocytosis (initial symptoms: pyrexia, pharynx pain, malaise, etc.), hemolytic anemia with hemoglobinuria or thrombocytopenia;
Interstitial pneumonia or eosinophilic pneumonia accompanied with pyrexia, cough, dyspnea, abnormal chest X-ray, or eosinophilia, etc.
Serious colitis with bloody stool, such as pseudomembranous colitis: If such symptoms as abdominal pain and frequent diarrhea are noted, treatment with levofloxacin should be discontinued immediately and appropriate therapeutic measures taken.
Rhabdomyolysis characterized by myalgia, weakness, elevated CK (CPK) and increased myoglobin in plasma and urine, etc., and accompanied with acute exacerbation of renal function.
Dysglycemia: During post-marketing surveillance, hypoglycemia and hyperglycemia have been reported in patients taking levofloxacin. Serious symptoms such as hypoglycemic coma have been reported in patients receiving levofloxacin. Hypoglycemia may be prone to develop in patients with diabetes mellitus (especially, those receiving sulfonylureas or insulin preparations), patients with impaired renal function and geriatric patients.
Tendon disorders such as Achilles tendonitis or tendon rupture: If symptoms such as pain and edema in the peritendinous region are observed, treatment with levofloxacin should be discontinued immediately and appropriate therapeutic measures taken. The risk of tendonitis and tendon rupture is increased in those over age 60, in those on concomitant corticosteroid therapy, and transplant recipients.
Psychiatric symptoms such as confusion, delirium and depression.
Hypersensitivity vasculitis: If symptoms such as pyrexia, abdominal pain, arthralgia, purpura or maculopapules, and skin biopsy evidence of leukocytoclastic vasculitis are observed, treatment with levofloxacin should be discontinued immediately and appropriate therapeutic measures taken.
Exacerbation of myasthenia gravis.
Aortic aneurysm, aortic dissection (incidence unknown): Aortic aneurysm or aortic dissection may occur. If any abnormalities are observed, appropriate medical treatment should be taken. (see Precautions).


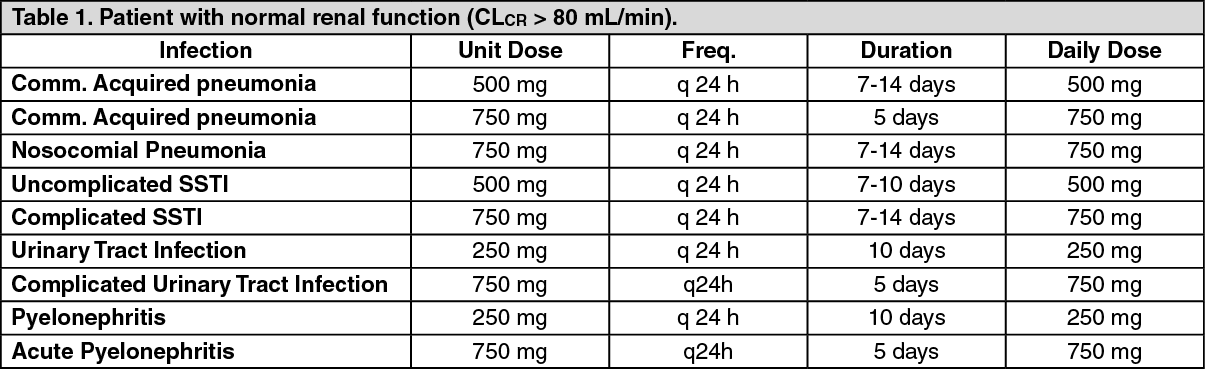 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image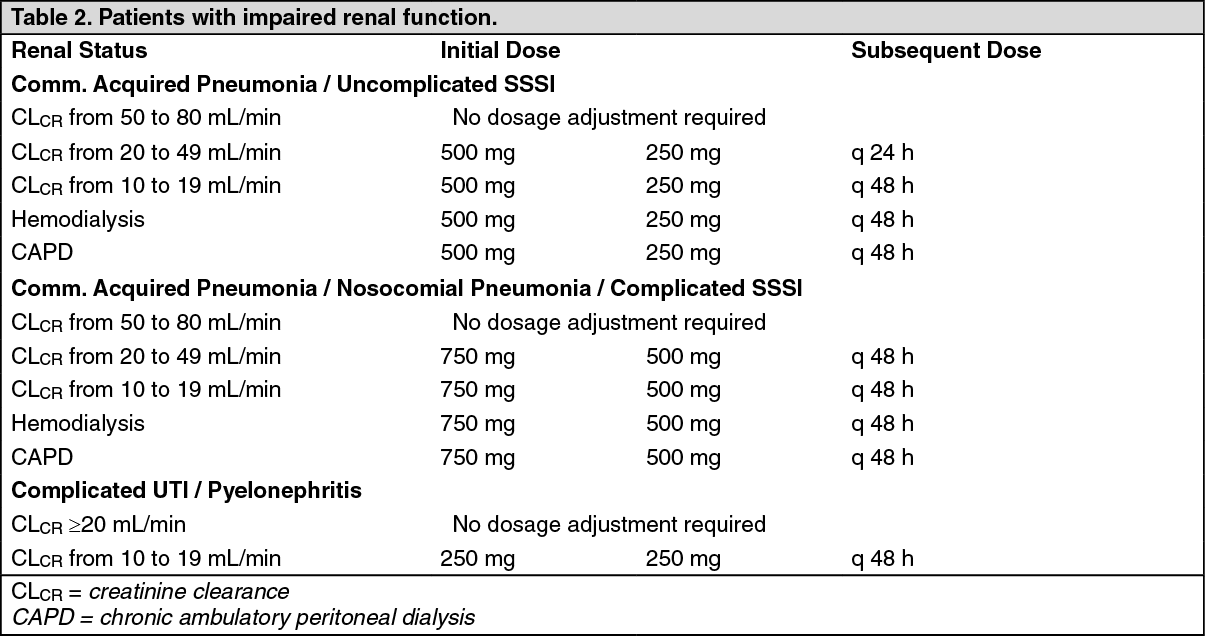 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
