Curam FC tab/oral susp: Curam oral dosage recommendations for children below the age of 12 years are based on 25-50 mg/kg body weight/day [based on amoxicillin component], depending-on the severity of infection.
Dosage in adults and children over 12 years of age and weight over 40 kg: Mild - Moderate infections: One Curam 375 mg three times a day or every 8 hours or One Curam 625 mg two times a day or every 12 hours.
Severe infections: One Curam 625 mg three times a day or every 8 hours.
Where the 625 mg tablet is not available, a dose of two Curam 375 mg three times a day may be taken or One Curam 1000 mg two times a day or every 12 hours.
Curam 375 mg, 625 mg and 1000 mg are not recommended in children under 12 years of age and weight less than 40 kg.
Dosage in children 7-12 years: 10ml Curam 156.25 mg/5 ml suspension three times a day, or 5ml Curam forte 312.5 mg/5 ml suspension three times a day*.
Dosage in children 2-7 years: 5ml Curam 156.25 mg/5 ml suspension three times a day*.
Dosage in children 9 months-2 years: 2.5 ml Curam 156.25 mg/5 ml suspension three times a day*.
Dosage in children 0-9 months: no suitable oral presentation is currently available for this age group.
Treatment with Curam should not be extended beyond 14 days without review.
*these dosages may be doubled in severe infections.
Curam 457 mg/5 mL oral susp: The exact dose for children above 2 months of age should be based on their body weight. Depending upon severity of infection, the daily dose in children less than 40 kg body weight is 25-45 mg/kg body weight (based on the amoxicillin component), divided into two equal doses.
The measuring device is enclosed for the dosage and administration of suspension: 1 full measuring device provides 5ml,
3/
4 measuring device provides 3.75 ml,
1/
2 measuring device provides 2.5 ml,
1/
4 provides 1.25 ml of oral suspension.
The usual recommended daily dosage is: 25 mg/kg/day (based on the amoxicillin component) in mild to moderate infections (upper respiratory tract infections e.g. recurrent tonsillitis, lower respiratory infections and skin and soft tissue infections).
45 mg/kg/day (based on the amoxicillin component) for the treatment of more serious infections (upper respiratory tract infections e.g. otitis media and sinusitis, lower respiratory tract infections e.g. bronchopneumonia and urinary tract infections).
The tables as follows give guidance for children.
Children over 2 years: See Table 4.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Children aged 2 months to 2 years: Children under 2 years should be dosed according to body weight. (See Table 5.)
Click on icon to see table/diagram/image
There is insufficient experience with Curam suspension 457 mg/5ml to make dosage recommendations for children under 2 months old.
Shake the bottle well before each using.
Curam Solutab: Dosage in adults and children over 12 years of age: The tablets should be stirred in half a glass of water (minimum 30 ml), and mixed thoroughly before taking; or placed in the mouth to disperse, before being swallowed.
Dose should be taken at regular intervals throughout the day, ideally at 8 hour intervals for Curam Solutab 625 mg and 12 hour intervals for 1 g or as prescribed.
Dosage in renal impairment/insufficiency: With renal impairment the dose should be reduced in accordance with the severity of the dysfunction and the patient's weight (Curam FC tab/oral susp and Curam Solutab).
Curam FC tab/oral susp: Adults: No change in dosage for patients with mild renal insufficiency (creatinine clearance more than 30 ml/min).
In patients with moderate renal insufficiency (creatinine clearance 10 to 30 ml/min) the dose is 1 tablet 375 mg or 1 tablet 625 mg two times a day or every 12 hours.
In patients with severe renal insufficiency (creatinine clearance less than 10 ml/min) the dose is not more than 1 tablet 375 mg every 12 hours or not more than 1 tablet 625 mg every 24 hours.
Children: No change in dosage for patients with mild renal insufficiency (creatinine clearance more than 30 ml/min).
In patients with moderate renal insufficiency (creatinine clearance 10 to 30 ml/min) the dose is 18.75 mg/kg two times a day (maximum 625 mg two times a day).
In patients with severe renal insufficiency (creatinine clearance less than 10 ml/min) the dose is 18.75 mg/kg given as a single daily dose (maximum 625 mg).
Curam 457 mg/5 mL oral susp: For children with a GFR of > 30ml/min no adjustment in dosage is required. For children with a GFR of < 30ml/min Curam 457 mg/5 ml is not recommended.
Dosage in infants with immature kidney function: For infants with immature renal function Curam 457 mg/5 ml is not recommended.
Curam Solutab: Dose in renal impairment in relation to patient weighing 70 kg: See Table 6.
Click on icon to see table/diagram/image
Dosage in hepatic functional impairment: Administer with caution. The liver function should be monitored at regular intervals. The experience in the use of the product in hepatic insufficiency is not adequate in order to give dose recommendations.
Curam Solutab: Curam Solutab must not be used in patients with severe hepatic functional impairment and in patients in whom hepatic functional impairment had occurred on previous therapy with Curam Solutab. Liver function parameters should be checked at regular intervals in patients with signs of hepatic lesions and a change of therapy should be given consideration if these parameters exacerbate on treatment.
Method of administration: Amoxicillin/clavulanic acid is recommended to be taken with meals to reduce any possible gastrointestinal discomfort.
Duration of administration/therapy:
Curam FC tab/oral susp: The length of treatment will be decided by the physician. Do not discontinue therapy of the patient's own accord, even if patient feels better. Normally treatment with this medicine should be continued for three to four days after recovery from the illness or disappearance of the symptoms.
Treatment should not be extended beyond 14 days without review by the physician.
As a precaution, therapy over at least 10 days is indicated in the treatment of infections with β-haemolytic streptococci in order to guard against late complications (e.g. rheumatic fever, glomerulonephritis).
Curam 457 mg/5 mL oral susp: Curam 457mg/5ml should be administered for a further 3 to 4 days after improvement/regression of the symptoms and should be continued, however, for a least the generally recommended minimum period of treatment. Treatment should not be extended beyond 14 days without review by the physician.
As a precaution, over at least 10 days is indicated in the treatment of infections with beta-haemolytic streptococci in order to guard against late complications (e.g. rheumatic fever, glomerulonephritis).
If the medicinal product is forgotten to be given, give the forgotten dose as soon as remembered. But do not give the next dose too soon, it must be at minimum 4 hours between two doses. Try to carry on as before (after 12 hours give the next dose). Do not double the dose.
Curam Solutab: The duration of therapy should be determined by the response of the patient. Some infections (e.g. osteomyelitis) require longer periods of treatment. Treatment should not be extended beyond 14 days without review by the physician.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image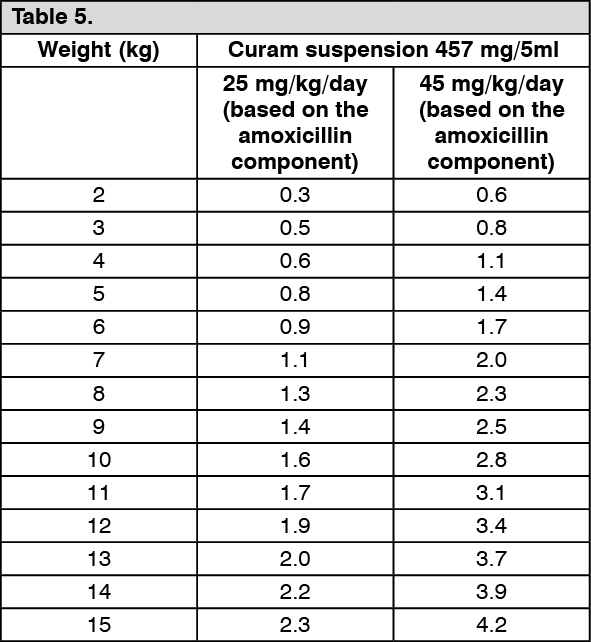 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image







 Sign Out
Sign Out
