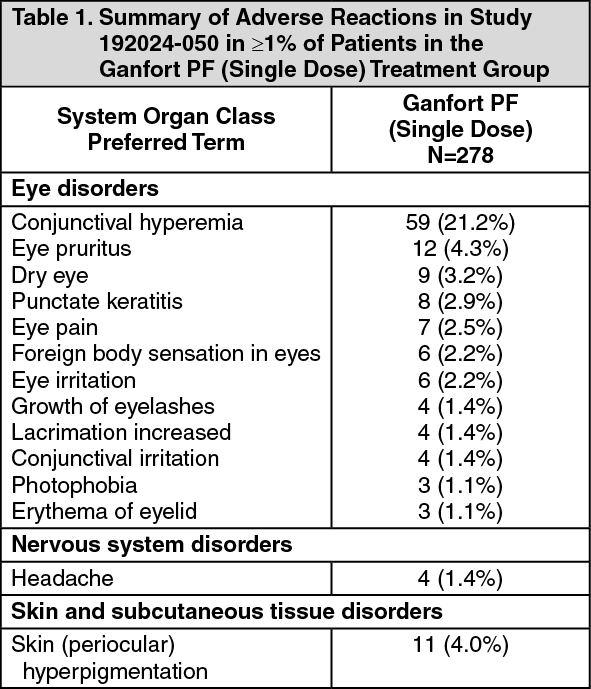
Clinical Study - Ganfort PF (Single Dose) - Study 192024-050: Study 192024-050 was a multicenter, double-masked, randomized, parallel study comparing the efficacy and safety of Ganfort PF (single dose) to Ganfort Eye Drops Solution (multidose) in patients with glaucoma or ocular hypertension and treated once daily for 3 months. A total of 278 and 283 patients were randomized to the Ganfort PF (single dose) and Ganfort Eye Drop Solution (multidose) treatment groups, respectively.
Table 1 presents the undesirable effects considered related to treatment that were reported in ≥1% of patients during treatment with Ganfort PF (single dose). Most were ocular, mild and none was serious. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Table 2 presents the adverse reactions with incidence rates <1%. (See Table 2.)
Click on icon to see table/diagram/image
Postmarketing Experience: The following adverse reactions have been identified during postmarketing use of Ganfort PF (single dose) in clinical practice. Because they are reported voluntarily from a population of unknown size, estimates of frequency cannot be made.
Cardiac Disorders: Bradycardia.
Eye Disorders: Eye swelling, ocular discomfort.
Immune System Disorders: Hypersensitivity reactions including sign or symptoms of allergic dermatitis, angioedema, eye allergy.
Respiratory, Thoracic and Mediastinal Disorders: Asthma, dyspnea.
Skin Disorders: Alopecia, skin discoloration (periocular).
Vascular disorders: Hypertension.
Additional Adverse Reactions: The additional adverse reactions listed as follows have been reported with the active substances bimatoprost and timolol and may potentially occur with Ganfort PF.
Bimatoprost 0.03% single dose (for ophthalmic use): Eye disorders: Hair growth abnormal, eye discharge, periorbital and lid changes associated with periorbital fat atrophy and skin tightness resulting in deepening of eyelid sulcus, eyelid ptosis, enophthalmos and eyelid retraction.
Timolol (ophthalmic use): Eye Disorders: Blepharitis, choroidal detachment following filtration surgery (see Precautions), decreased corneal sensitivity, diplopia, eye discharge, pseudopemphigoid, ptosis, refractive changes; signs and symptoms of ocular irritation including conjunctivitis and keratitis.
Cardiac Disorders: Arrhythmia, atrioventricular block, cardiac arrest, cardiac failure, chest pain, congestive heart failure, edema, heart block, palpitations, pulmonary edema, worsening of angina pectoris.
Ear and Labyrinth Disorders: Tinnitus.
Gastrointestinal Disorders: Abdominal pain, anorexia, diarrhea, dry mouth, dyspepsia, nausea, vomiting.
General Disorders and Administration Site Conditions: Asthenia.
Immune System Disorders: Systemic allergic reactions including anaphylaxis, systemic lupus erythematosus.
Metabolism and Nutrition Disorders: Hypoglycemia (in diabetic patients, see Precautions).
Musculoskeletal and Connective Tissue Disorders: Myalgia.
Nervous System Disorders: Cerebral ischemia, cerebrovascular accident, increase in signs and symptoms of myasthenia gravis, paresthesia, syncope.
Psychiatric Disorders: Behavioral changes and psychic disturbances including anxiety, confusion, depression, disorientation, hallucinations, nervousness, memory loss, somnolence.
Reproductive System and Breast Disorders: Decreased libido, Peyronie's disease, retroperitoneal fibrosis, sexual dysfunction.
Respiratory, Thoracic and Mediastinal Disorders: Bronchospasm (predominantly in patients with pre-existing bronchospastic disease) (see Precautions), cough, nasal congestion, respiratory failure, upper respiratory infection.
Skin and Subcutaneous Tissue Disorders: Exacerbation of psoriasis, psoriasiform rash, skin rash.
Vascular Disorders: Claudication, cold hands and feet, hypotension, Raynaud's phenomenon.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image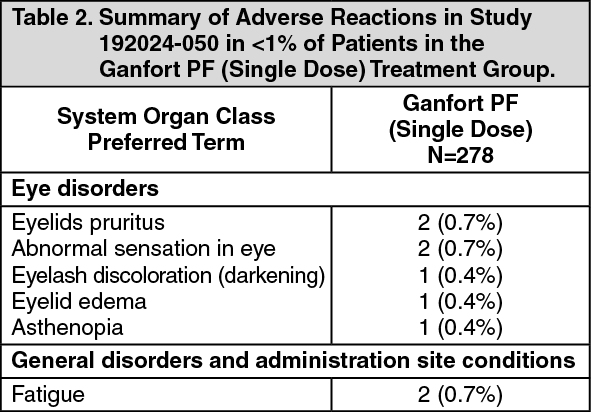 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
