Each 5 mL contains Paracetamol 120 mg or 250 mg, respectively.
Excipients/Inactive Ingredients: 250 mg/5 mL: Sucrose, Methylparaben, Propylparaben, Carboxymethylcellulose sodium, Microcrystalline cellulose, Polysorbate 80, Sorbitol solution, Glycerin, Titanium dioxide, Sweet orange essence, Kingcol sunset yellow, Propylene glycol, Purified water qs to.
Pharmacology: Pharmacodynamics: 120 mg/5 mL: Although not fully elucidated, believed to inhibit the synthesis of prostaglandins in the central nervous system and work peripherally to block pain impulse generation; produces antipyresis from inhibition of hypothalamic heat-regulating center.
250 mg/5 mL: Paracetamol (Acetaminophen) is the active metabolite of phenacetin and has antipyretic and analgesic activities.
Pharmacokinetics: 120 mg/5 mL: Onset of action: Oral: <1 hour.
Duration: Oral: Analgesia: 4-6 hours.
Absorption: Primarily absorbed in small intestine (rate of absorption dependent upon gastric emptying); minimal absorption from stomach; varies by dosage form.
Distribution: ~1 L/kg at therapeutic doses.
Protein binding: 10% to 25% at therapeutic concentrations; 8% to 43% at toxic concentrations.
Metabolism: At normal therapeutic dosages, primarily hepatic metabolism to sulfate and glucuronide conjugates, while a small amount is metabolized by CYP2E1 to a highly reactive intermediate, N-acetyl-p-benzoquinone imine (NAPQI), which is conjugated rapidly with glutathione and inactivated to nontoxic cysteine and mercapturic acid conjugates. At toxic doses (as little as 4 g daily) glutathione conjugation becomes insufficient to meet the metabolic demand causing an increase in NAPQI concentrations, which may cause hepatic cell necrosis. Oral administration is subject to first pass metabolism.
Half-life elimination: Prolonged following toxic doses.
Neonate: 7 hours (range: 4-10 hours).
Infants: ~4 hours (range: 1-7 hours).
Children: 3 hours (range: 2-5 hours).
Adolescents: ~3 hours (range: 2-4 hours).
Adults: ~2 hours (range: 2-3 hours); may be slightly prolonged in severe renal insufficiency.
(Clcr < 30 mL/minute ): 2-5.3 hours.
Time to peak, serum: Oral: Immediate release: 10-60 minutes (may be delayed in acute overdoses).
Excretion: Urine (<5% unchanged; 60% to 80% as glucuronide metabolites; 20% to 30% as sulphate metabolites; ~8% cysteine and mercapturic acid metabolites).
250 mg/5 mL: Paracetamol is absorbed rapidly, and peak plasma levels are reached in 30 to 60 minutes. Approximately 90% of paracetamol usually undergoes hepatic conjugation with glucuronide (40% to 67%) and sulfate (20% to 46%) to form inactive metabolites that area excreted in the urine.
Toxicology: Preclinical safety data: 250 mg/5 mL: Not applicable.
For relief of fever and pains.
Recommended dose: 120 mg/5 mL: Children 4-6 months of age: 2 droppers (2.4 mL).
Children 2-3 months of age: 1 ½ droppers (18 mL).
Children 1 month of age: 1 dropper (1.2 mL).
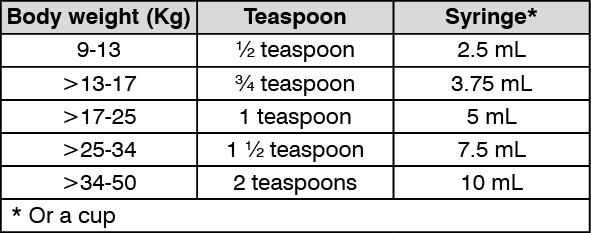
250 mg/5 mL: If there is pain or fever, take this medicine not more than 5 times a day, every 4 hours, given according to the dose in the table. (See table.)
 Click on icon to see table/diagram/image
Mode of administration: 120 mg/5 mL:
Click on icon to see table/diagram/image
Mode of administration: 120 mg/5 mL: Oral.
120 mg/5 mL: Overdose and treatment: Symptoms include hepatic necrosis, transient azotemia, renal tubular necrosis with acute toxicity, anemia, and GI disturbances with chronic toxicity. Acetylcysteine 140 mg/kg orally (loading) followed by 70 mg/kg every 4 hours for 17 doses. Therapy should be initiated based upon laboratory analysis suggesting high probability of hepatotoxic potential. Activated charcoal is very effective at binding acetaminophen.
250 mg/5 mL: Symptoms: Paracetamol toxicity may result from a single toxic dose, from repeated ingestion of large doses of paracetamol (e.g. 7.5-10 g daily for 1-2 days), or from chronic ingestion of the drug.
Nausea, vomiting, and abdominal pain usually occur within 2-3 hours after ingestion of toxic doses of the drug. Fulminant, fatal hepatic failure may occur in chronic alcoholics following overdosage of paracetamol. P-Aminophenol derivatives may elevate serum bilirubin concentrations, and jaundice may develop within 2-6 days. Young children appear to be less likely to develop hepatotoxic effects than adults.
Treatment: If paracetamol has been recently ingested, activated charcoal may reduce paracetamol absorption and should be administered as soon as possible (preferably within 1 hour of ingestion). Acetylcysteine therapy is initiated within 8-16 hours of ingestion, but acetylcysteine is effective when given more than 24 hours after ingestion.
Acetylcysteine 20% i.v.: Administer intravenously, 20% acetylcysteine immediately without waiting for positive urine test or plasma level results: initial dose of 150 mg/kg over 15 minutes, followed by continuous infusion of 50 mg/kg in 500 ml 5% glucose/dextrose over 4 hours and 100mg/kg in 1 L 5% glucose/dextrose over 16 hours; or.
Oral Methionine: 2.5 g immediately followed by three further doses of 2.5 g at four hourly intervals. For a 3-year-old child, 1 g methionine every four hours for four doses has been used; or.
Oral Acetylcysteine 5%: 140 mg/kg as a loading dose, then 70 mg/kg every 4 hours for a total of 17 maintenance doses. If more than ten hours have elapsed since the overdosage was taken, the antidote may be ineffective.
Hypersensitivity to acetaminophen/paracetamol or any component of the formulation; severe hepatic impairment or severe active liver disease. Not use continuous over 5 days.
120 mg/5 mL: Limit acetaminophen dose from all sources (prescription and OTC) to < 4 g/day. May cause severe hepatotoxicity on acute overdose; in addition, chronic daily dosing in adults has resulted in liver damage in some patients; hepatotoxicity is usually associated with excessive acetaminophen intake (> 4 g/day). Use with caution in patients with alcoholic liver disease; consuming ≥ 3 alcoholic drinks/day may increase the risk of liver damage. Use caution in patients with hepatic impairment or active liver disease. Use caution in patients with known G6PD deficiency; rare reports of hemolysis have occurred. Use caution in patients with severe renal impairment; consider dosing adjustments. Hypersensitivity and anaphylactic reactions have been reported; discontinue immediately if symptoms of allergic or hypersensitivity reactions occur.
250 mg/5 mL: Do not take paracetamol more than the recommended dose as described in the label or leaflet because paracetamol can cause hepatotoxicity and do not take more than 5 days.
Do not take other paracetamol containing products whilst taking this medicine because it may cause overdose.
Consult with the doctor or pharmacist before taking this medicine if patient has alcoholism and liver or kidney disease.
If there is swelling of the face, eyes and lips, urticaria, fainting, skin rash, skin peeling, stop taking this medicine and consult the doctor immediately.
Effects on ability to drive and use machine: No effects on ability to drive and use machine.
120 mg/5 mL: Pregnancy risk factor C.
250 mg/5 mL: The use of paracetamol in normal doses during pregnancy is not associated with an increased risk of miscarriage or still birth. Frequent maternal use of paracetamol during pregnancy may be associated with wheezing and asthma in early childhood.
Lactation: Enters breast milk/use caution.
120 mg/5 mL: Dermatologic: Rash.
Endocrine & metabolic: May increase chloride, uric acid, glucose; may decrease sodium, bicarbonate, calcium.
Hematologic: Anemia; blood dyscrasias (neutropenia, pancytopenia, leukopenia).
Hepatic: May increase bilirubin, alkaline phosphatase.
Renal: May increase ammonia, nephrotoxicity with chronic overdose, analgesic nephropathy.
Miscellaneous: Hypersensitivity reactions (rare).
250 mg/5 mL: Adverse effects of paracetamol are rare and usually mild, although hematological reactions have been reported. Cutaneous hypersensitivity reactions including skin rashes, angioedema, Stevens-Johnson Syndrome/Toxic epidermal Necrolysis have been reported.
Increased Effect/Toxicity: Acetaminophen/paracetamol may increase the levels/effects of: ARI-Piprazole; Busulfan; Dasatinib; Imatinib; Lomitapide; Pimozide; Prilocaines; SORAfenib; Vitamin K Antagonists.
Decreased Effect: The levels/effects of Acetaminophen/paracetamol may be decreased by: Anticonvulsants (Hydantoin); Barbiturates; Carbamazepine; Cholestyramine Resin; Peginterferon Alfa-2b.
Ethanol/Nutrition/Herb Interactions: Ethanol: Excessive intake of ethanol may increase the risk of acetaminophen-induced hepatotoxicity. (Avoid ethanol or limit to < 3 drinks/day - for 120 mg/5 mL only).
120 mg/5 mL: The levels/effects of Acetaminophen may be increased by: Dasatinib; Imatinib; Isoniazid; Metyrapone; Probenecid; SORAfenib.
Food: Rate of absorption may be decreased when given with food.
Herb/Nutraceutical: St John's wort may decrease acetaminophen levels.
Incompatibilities: 250 mg/5 mL: Not applicable.
Store below 30°C and protected from light.
Shelf-life: 250 mg/5 mL: 24 months.
N02BE01 - paracetamol ; Belongs to the class of anilide preparations. Used to relieve pain and fever.
Paracap Suspension oral susp 120 mg/5 mL
60 mL x 1's
Paracap Suspension oral susp 250 mg/5 mL
60 mL x 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out