


 Sign Out
Sign Out




The most common adverse reactions in adult patients in clinical trials (≥ 10%) were nausea, vomiting, constipation, headache, dizziness, akathisia, anxiety, insomnia, and restlessness.
The most common adverse reactions in the pediatric clinical trials (≥ 10%) were somnolence, headache, vomiting, extrapyramidal disorder, fatigue, increased appetite, insomnia, nausea, nasopharyngitis, and weight increased.
Aripiprazole has been evaluated for safety in 13,543 adult patients who participated in multiple-dose, clinical trials in schizophrenia, bipolar disorder, major depressive disorder, and Dementia of the Alzheimer's type, Parkinson's disease, and alcoholism, and who had approximately 7619 patient-years of exposure to oral aripiprazole and 749 patients with exposure to aripiprazole injection. A total of 3390 patients were treated with oral aripiprazole for at least 180 days and 1933 patients treated with oral aripiprazole had at least 1 year of exposure.
Aripiprazole has been evaluated for safety in 920 patients (6 to 17 years) who participated in multiple-dose, clinical trials in schizophrenia, bipolar mania, or autistic disorder and who had approximately 517 patient-years of exposure to oral aripiprazole. A total of 465 pediatric patients were treated with oral aripiprazole for at least 180 days and 117 pediatric patients treated with oral aripiprazole had at least 1 year of exposure.
The conditions and duration of treatment with aripiprazole (monotherapy and adjunctive therapy with antidepressants or mood stabilizers) included (in overlapping categories) double-blind, comparative and noncomparative open-label studies, inpatient and outpatient studies, fixed- and flexible-dose studies, and short- and longer-term exposure.
Adverse events during exposure were obtained by collecting volunteered adverse events, as well as results of physical examinations, vital signs, weights, laboratory analyses, and ECG. Adverse experiences were recorded by clinical investigators using terminology of their own choosing. In the tables and tabulations that follow, MedDRA dictionary terminology has been used to classify reported adverse events into a smaller number of standardized event categories, in order to provide a meaningful estimate of the proportion of individuals experiencing adverse events.
The stated frequencies of adverse reactions represent the proportion of individuals who experienced at least once, a treatment-emergent adverse event of the type listed. An event was considered treatment emergent if it occurred for the first time or worsened while receiving therapy following baseline evaluation. There was no attempt to use investigator causality assessments; ie, all events meeting the defined criteria, regardless of investigator causality are included.
Throughout this section, adverse reactions are reported. These are adverse events that were considered to be reasonably associated with the use of ABILIFY (adverse drug reactions) based on the comprehensive assessment of the available adverse event information. A causal association for ABILIFY often cannot be reliably established in individual cases.
The figures in the tables and tabulations cannot be used to predict the incidence of side effects in the course of usual medical practice where patient characteristics and other factors differ from those that prevailed in the clinical trials. Similarly, the cited frequencies cannot be compared with figures obtained from other clinical investigations involving different treatment, uses, and investigators. The cited figures, however, do provide the prescriber with some basis for estimating the relative contribution of drug and nondrug factors to the adverse reaction incidence in the population studied.
Clinical Studies Experience: Adult Patients with Schizophrenia: The following findings are based on a pool of five placebo-controlled trials (four 4-week and one 6-week) in which oral aripiprazole was administered in doses ranging from 2 mg/day to 30 mg/day.
Adverse Reactions Associated with Discontinuation of Treatment: Overall, there was little difference in the incidence of discontinuation due to adverse reactions between aripiprazole-treated (7%) and placebo-treated (9%) patients. The types of adverse reactions that led to discontinuation were similar for the aripiprazole- and placebo-treated patients.
Commonly Observed Adverse Reactions: The only commonly observed adverse reaction associated with the use of aripiprazole in patients with schizophrenia (incidence of 5% or greater and aripiprazole incidence at least twice that for placebo) was akathisia (aripiprazole 8%; placebo 4%).
Adult Patients with Bipolar Mania: Monotherapy: The following findings are based on a pool of 3-week, placebo-controlled, bipolar mania trials in which oral aripiprazole was administered at doses of 15 mg/day or 30 mg/day.
Adverse Reactions Associated with Discontinuation of Treatment: Overall, in patients with bipolar mania, there was little difference in the incidence of discontinuation due to adverse reactions between aripiprazole-treated (11%) and placebo-treated (10%) patients. The types of adverse reactions that led to discontinuation were similar between the aripiprazole-treated and placebo-treated patients.
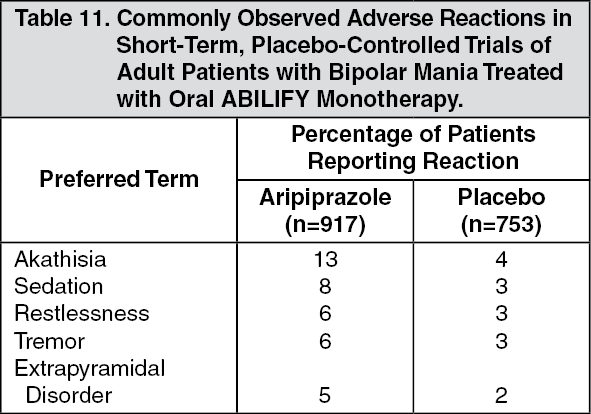
Commonly Observed Adverse Reactions: Commonly observed adverse reactions associated with the use of aripiprazole in patients with bipolar mania (incidence of 5% or greater and aripiprazole incidence at least twice that for placebo) are shown in Table 11. (See Table 11.)
 Click on icon to see table/diagram/image
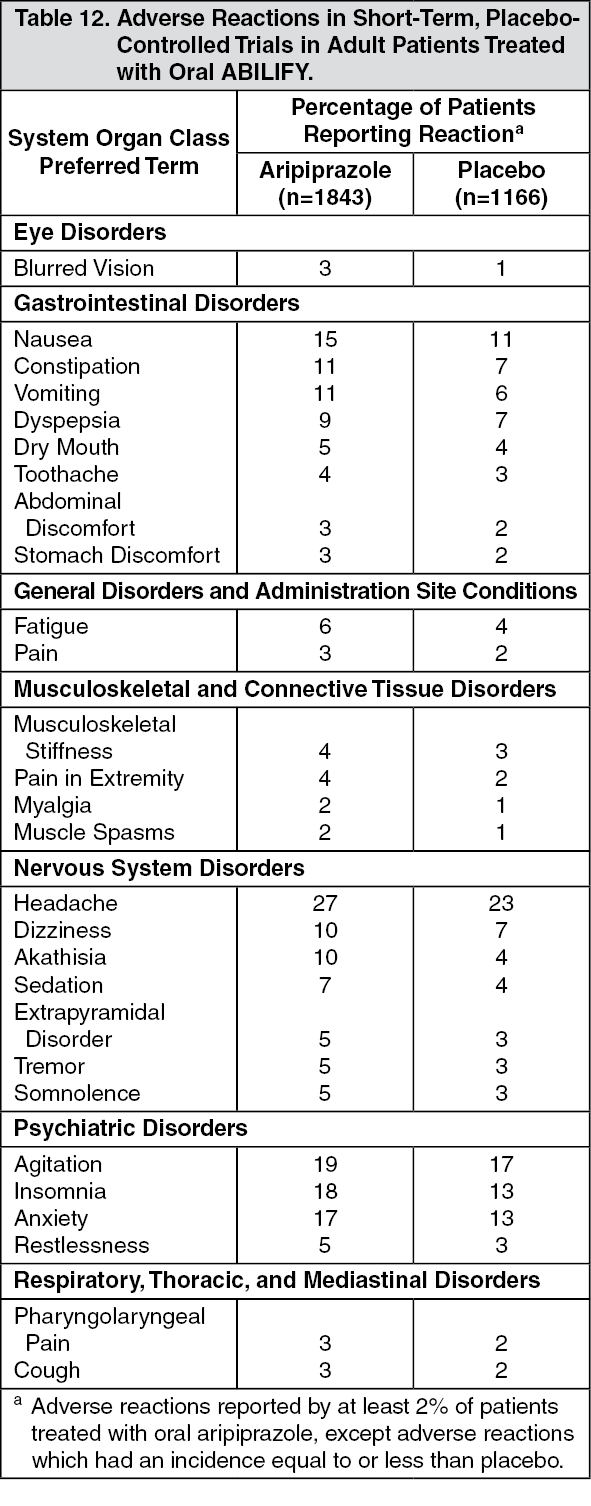
Click on icon to see table/diagram/imageLess Common Adverse Reactions in Adults: Table 12 enumerates the pooled incidence, rounded to the nearest percent, of adverse reactions that occurred during acute therapy (up to 6 weeks in Schizophrenia and up to 3 weeks in bipolar mania), including only those reactions that occurred in 2% or more of patients treated with aripiprazole (doses ≥ 2 mg/day) and for which the incidence in patients treated with aripiprazole was greater than the incidence in patients treated with placebo in the combined dataset. (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAn examination of population subgroups did not reveal any clear evidence of differential adverse reaction incidence on the basis of age, gender, or race.
Adults Patients with Adjunctive Therapy with Bipolar Mania: The following findings are based on a placebo-controlled trial of adult patients with bipolar disorder in which aripiprazole was administered at doses of 15 mg/day or 30 mg/day as adjunctive therapy with lithium or valproate.
Adverse Reactions Associated with Discontinuation of Treatment: In a study of patients who were already tolerating either lithium or valproate as monotherapy, discontinuation rates due to adverse reactions were 12% for patients treated with adjunctive aripiprazole compared to 6% for patients treated with adjunctive placebo. The most common adverse drug reactions associated with discontinuation in the adjunctive aripiprazole-treated compared to placebo-treated patients were akathisia (5% and 1%, respectively) and tremor (2% and 1%, respectively).
Commonly Observed Adverse Reactions: The commonly observed adverse reactions associated with adjunctive aripiprazole and lithium or valproate in patients with bipolar mania (incidence of 5% or greater and incidence at least twice that for adjunctive placebo) were: akathisia, insomnia, and extrapyramidal disorder.
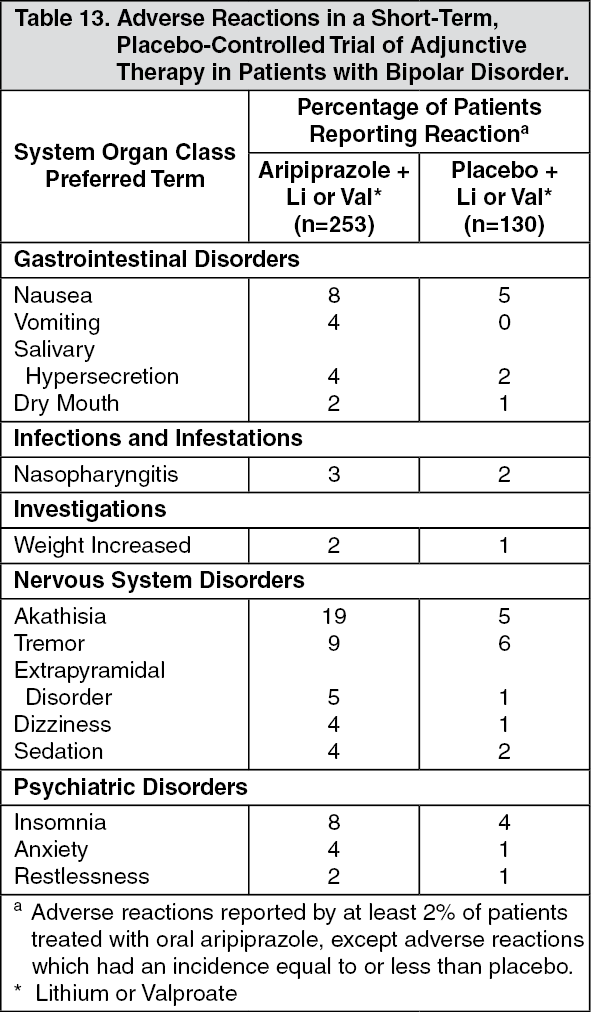
Less Common Adverse Reactions in Adult Patients with Adjunctive Therapy in Bipolar Mania: Table 13 enumerates the incidence, rounded to the nearest percent, of adverse reactions that occurred during acute treatment (up to 6 weeks), including only those reactions that occurred in 2% or more of patients treated with adjunctive aripiprazole (doses of 15 mg/day or 30 mg/day) and lithium or valproate and for which the incidence in patients treated with this combination was greater than the incidence in patients treated with placebo plus lithium or valproate. (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePediatric Patients (13 to 17 years) with Schizophrenia: The following findings are based on one 6-week placebo-controlled trial in which oral aripiprazole was administered in doses ranging from 2 mg/day to 30 mg/day.
Adverse Reactions Associated with Discontinuation of Treatment: The incidence of discontinuation due to adverse reactions between aripiprazole-treated and placebo-treated pediatric patients (13 to 17 years) was 5% and 2%, respectively.
Commonly Observed Adverse Reactions: Commonly observed adverse reactions associated with the use of aripiprazole in adolescent patients with schizophrenia (incidence of 5% or greater and aripiprazole incidence at least twice that for placebo) were extrapyramidal disorder, somnolence, and tremor.
Pediatric Patients (10 to 17 years) with Bipolar Mania: The following findings are based on one 4-week placebo-controlled trial in which oral aripiprazole was administered in doses of 10 mg/day or 30 mg/day.
Adverse Reactions Associated with Discontinuation of Treatment: The incidence of discontinuation due to adverse reactions between aripiprazole-treated and placebo-treated pediatric patients (10 to 17 years) was 7% and 2%, respectively.
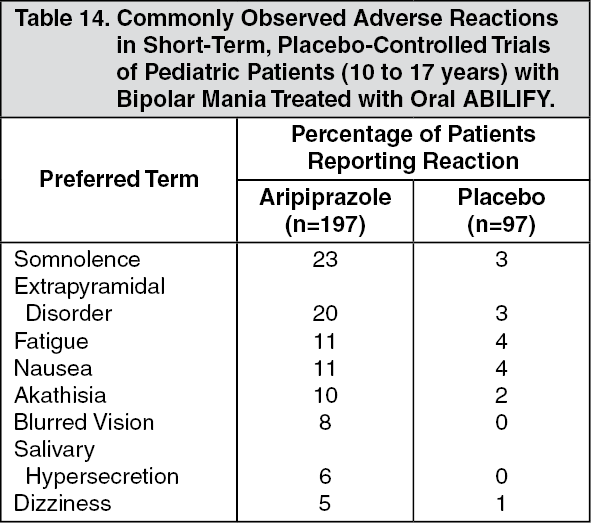
Commonly Observed Adverse Reactions: Commonly observed adverse reactions associated with the use of aripiprazole in pediatric patients with bipolar mania (incidence of 5% or greater and aripiprazole incidence at least twice that for placebo) are shown in Table 14. (See Table 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePediatric Patients (6 to 17 years) with Autistic Disorder: The following findings are based on two 8-week, placebo-controlled trials in which oral aripiprazole was administered in doses of 2 mg/day to 15 mg/day.
Adverse Reactions Associated with Discontinuation of Treatment: The incidence of discontinuation due to adverse reactions between aripiprazole-treated and placebo-treated pediatric patients (6 to 17 years) was 10% and 8%, respectively.
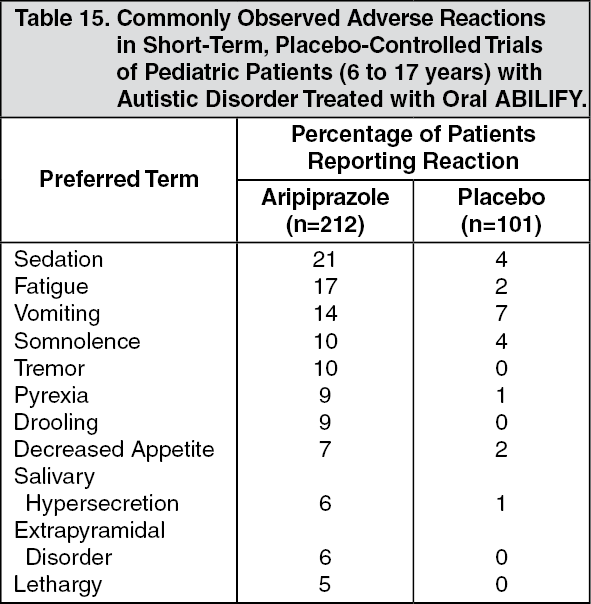
Commonly Observed Adverse Reactions: Commonly observed adverse reactions associated with the use of aripiprazole in pediatric patients with autistic disorder (incidence of 5% or greater and aripiprazole incidence at least twice that for placebo) are shown in Table 15. (See Table 15.)
 Click on icon to see table/diagram/image
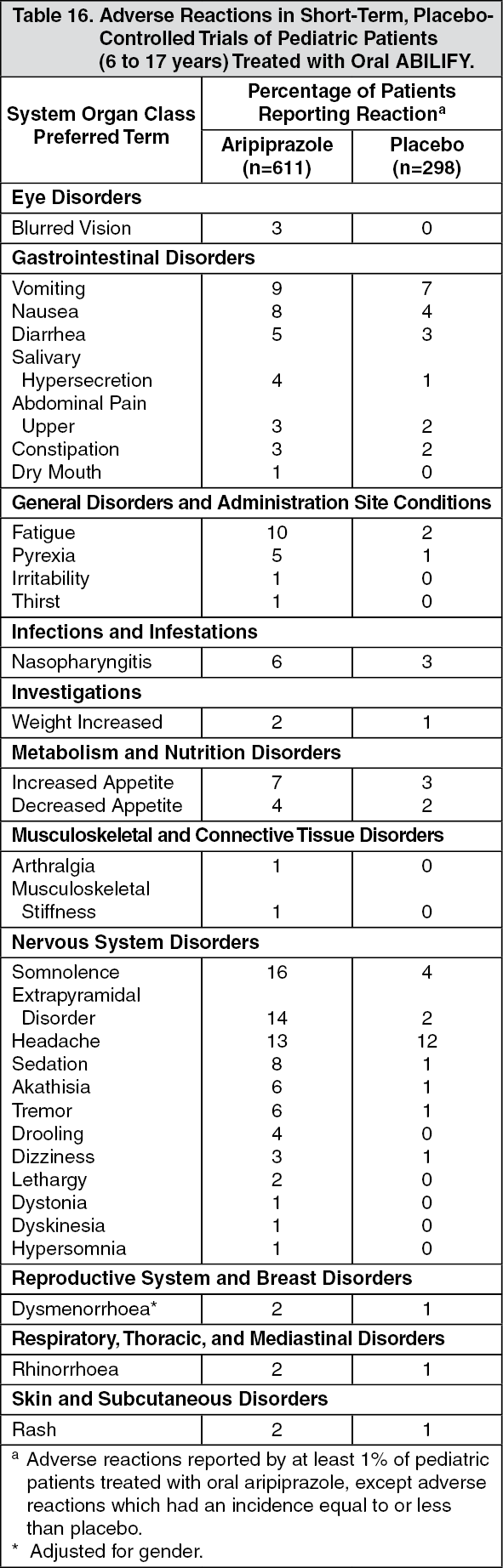
Click on icon to see table/diagram/imageLess Common Adverse Reactions in Pediatric Patients (6 to 17 years) with Schizophrenia, Bipolar Mania or Autistic Disorder: Table 16 enumerates the pooled incidence, rounded to the nearest percent, of adverse reactions that occurred during acute therapy (up to 6 weeks in schizophrenia, up to 4 weeks in bipolar mania, and up to 8 weeks in autistic disorder), including only those reactions that occurred in 1% or more of pediatric patients treated with aripiprazole (doses ≥ 2 mg/day) and for which the incidence in patients treated with aripiprazole was greater than the incidence in patients treated with placebo. (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdult Patients Receiving ABILIFY as Adjunctive Treatment of Major Depressive Disorder: The following findings are based on a pool of two placebo-controlled trials of patients with major depressive disorder in which aripiprazole was administered at doses of 2 mg to 20 mg as adjunctive treatment to continued antidepressant therapy.
Adverse Reactions Associated with Discontinuation of Treatment: The incidence of discontinuation due to adverse reactions was 6% for adjunctive aripiprazole-treated patients and 2% for adjunctive placebo-treated patients.
Commonly Observed Adverse Reactions: The commonly observed adverse reactions associated with the use of adjunctive aripiprazole in patients with major depressive disorder (incidence of 5% or greater and aripiprazole incidence at least twice that for placebo) were: akathisia, restlessness, insomnia, constipation, fatigue, and blurred vision.
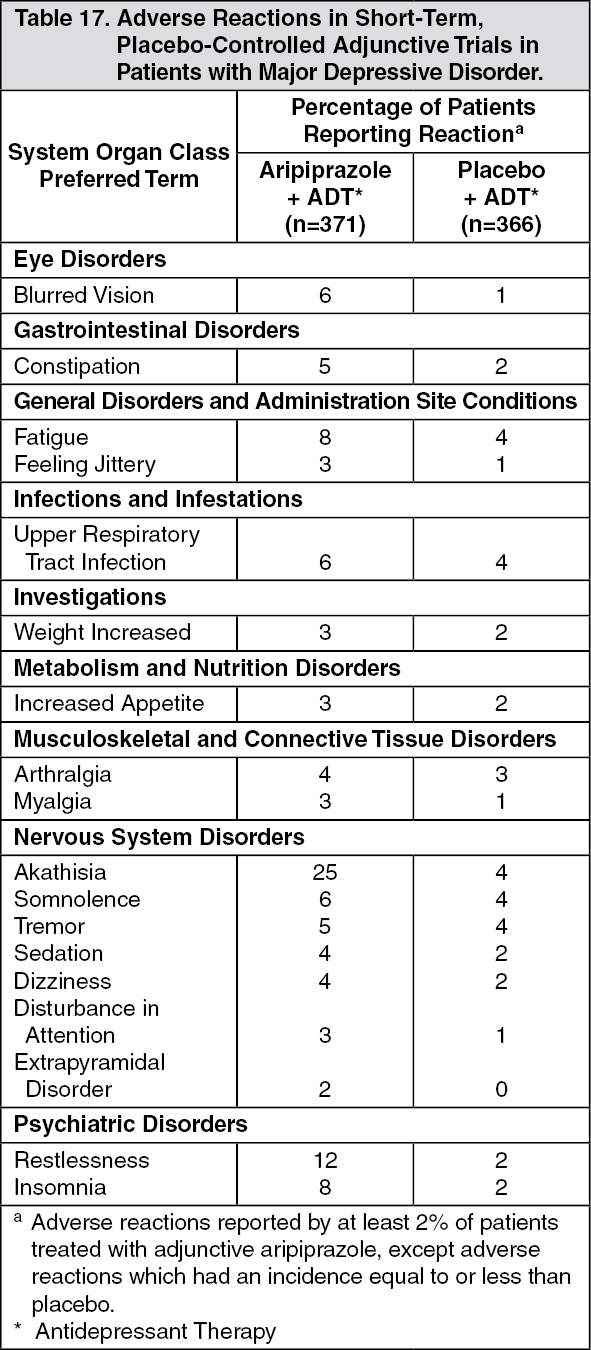
Less Common Adverse Reactions in Adult Patients with Major Depressive Disorder: Table 20 enumerates the pooled incidence, rounded to the nearest percent, of adverse reactions that occurred during acute therapy (up to 6 weeks), including only those adverse reactions that occurred in 2% or more of patients treated with adjunctive aripiprazole (doses ≥2 mg/day) and for which the incidence in patients treated with adjunctive aripiprazole was greater than the incidence in patients treated with adjunctive placebo in the combined dataset. (See Table 17.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDose-Related Adverse Reactions: Schizophrenia: Dose response relationships for the incidence of treatment-emergent adverse events were evaluated from four trials in adult patients with schizophrenia comparing various fixed doses (2 mg/day, 5 mg/day, 10 mg/day, 15 mg/day, 20 mg/day, and 30 mg/day) of oral aripiprazole to placebo. This analysis, stratified by study, indicated that the only adverse reaction to have a possible dose response relationship, and then most prominent only with 30 mg, was somnolence [including sedation]; (incidences were placebo, 7.1%; 10 mg, 8.5%; 15 mg, 8.7%; 20 mg, 7.5%; 30 mg, 12.6%).
In the study of pediatric patients (13 to 17 years of age) with schizophrenia, three common adverse reactions appeared to have a possible dose response relationship: extrapyramidal disorder (incidences were placebo, 5.0%; 10 mg, 13.0%; 30 mg, 21.6%); somnolence (incidences were placebo, 6.0%; 10 mg, 11.0%; 30 mg, 21.6%); and tremor (incidences were placebo, 2.0%; 10 mg, 2.0%; 30 mg, 11.8%).
Bipolar Mania: In the study of pediatric patients (10 to 17 years of age) with bipolar mania, four common adverse reactions had a possible dose response relationship at 4 weeks; extrapyramidal disorder (incidences were placebo, 3.1%; 10 mg, 12.2%; 30 mg, 27.3%); somnolence (incidences were placebo, 3.1%; 10 mg, 19.4%; 30 mg, 26.3%); akathisia (incidences were placebo, 2.1%, 10 mg, 8.2%; 30 mg, 11.1%); and salivary hypersecretion (incidences were placebo, 0%; 10 mg, 3.1%; 30 mg, 8.1%).
Autistic Disorder: In a study of pediatric patients (6 to 17 years of age) with autistic disorder, one common adverse reaction had a possible dose response relationship: fatigue (incidences were placebo, 0%; 5 mg, 3.8%; 10 mg, 22.0%; 15 mg, 18.5%).
Extrapyramidal Symptoms: Schizophrenia: In short-term, placebo-controlled trials in schizophrenia in adults, the incidence of reported EPS-related events, excluding events related to akathisia, for aripiprazole-treated patients was 13% vs. 12% for placebo; and the incidence of akathisia-related events for aripiprazole-treated patients was 8% vs. 4% for placebo. In the short-term, placebo-controlled trial of schizophrenia in pediatric patients (13 to 17 years), the incidence of reported EPS-related events, excluding events related to akathisia, for aripiprazole-treated patients was 25% vs. 7% for placebo; and the incidence of akathisia-related events for aripiprazole-treated patients was 9% vs. 6% for placebo.
Objectively collected data from those trials was collected on the Simpson Angus Rating Scale (for EPS), the Barnes Akathisia Scale (for akathisia), and the Assessments of Involuntary Movement Scales (for dyskinesias). In the adult schizophrenia trials, the objectively collected data did not show a difference between aripiprazole and placebo, with the exception of the Barnes Akathisia Scale (aripiprazole, 0.08; placebo, -0.05). In the pediatric (13 to 17 years) schizophrenia trial, the objectively collected data did not show a difference between aripiprazole and placebo, with the exception of the Simpson Angus Rating Scale (aripiprazole, 0.24; placebo, -0.29).
Similarly, in a long-term (26-week), placebo-controlled trial of schizophrenia in adults, objectively collected data on the Simpson Angus Rating Scale (for EPS), the Barnes Akathisia Scale (for akathisia), and the Assessments of Involuntary Movement Scales (for dyskinesias) did not show a difference between aripiprazole and placebo.
Bipolar Mania: In the short-term, placebo-controlled trials in bipolar mania in adults, the incidence of reported EPS-related events, excluding events related to akathisia, for monotherapy aripiprazole-treated patients was 16% vs. 8% for placebo and the incidence of akathisia-related events for monotherapy aripiprazole-treated patients was 13% vs. 4% for placebo. In the 6-week, placebo-controlled trial in bipolar mania for adjunctive therapy with lithium or valproate, the incidence of reported EPS-related events, excluding events related to akathisia for adjunctive aripiprazole-treated patients was 15% vs. 8% for adjunctive placebo and the incidence of akathisia-related events for adjunctive aripiprazole-treated patients was 19% vs. 5% for adjunctive placebo. In the short-term, placebo-controlled trial in Bipolar Mania in pediatric (10 to 17 years) patients, the incidence of reported EPS-related events, excluding events related to akathisia, for aripiprazole-treated patients was 26% vs. 5% for placebo and the incidence of akathisia-related events for aripiprazole-treated patients was 10% vs. 2% for placebo.
In the adult bipolar mania trials with monotherapy aripiprazole, the Simpson Angus Rating Scale and the Barnes Akathisia Scale showed a significant difference between aripiprazole and placebo (aripiprazole, 0.50; placebo, -0.01 and aripiprazole, 0.21; placebo, -0.05). Changes in the Assessments of Involuntary Movement Scales were similar for the aripiprazole and placebo groups. In the bipolar mania trials with aripiprazole as adjunctive therapy with either lithium or valproate, the Simpson Angus Rating Scale and the Barnes Akathisia Scale showed a significant difference between adjunctive aripiprazole and adjunctive placebo (aripiprazole, 0.73; placebo, 0.07 and aripiprazole, 0.30; placebo, 0.11). Changes in the Assessments of Involuntary Movement Scales were similar for adjunctive aripiprazole and adjunctive placebo. In the pediatric (10 to 17 years) short-term bipolar mania trial, the Simpson Angus Rating Scale showed a significant difference between aripiprazole and placebo (aripiprazole, 0.90; placebo, -0.05). Changes in the Barnes Akathisia Scale and the Assessments of Involuntary Movement Scales were similar for the aripiprazole and placebo groups.
Major Depressive Disorder: In the short-term, placebo-controlled trials in major depressive disorder, the incidence of reported EPS-related events, excluding events related to akathisia, for adjunctive aripiprazole-treated patients was 8% vs. 5% for adjunctive placebo-treated patients; and the incidence of akathisia-related events for adjunctive aripiprazole-treated patients was 25% vs. 4% for adjunctive placebo-treated patients.
In the major depressive disorder trials, the Simpson Angus Rating Scale and the Barnes Akathisia Scale showed a significant difference between adjunctive aripiprazole and adjunctive placebo (aripiprazole, 0.31; placebo, 0.03 and aripiprazole, 0.22; placebo, 0.02). Changes in the Assessments of Involuntary Movement Scales were similar for the adjunctive aripiprazole and adjunctive placebo groups.
Autistic Disorder: In the short-term, placebo-controlled trials in autistic disorder in pediatric patients (6 to 17 years), the incidence of reported EPS-related events, excluding events related to akathisia, for aripiprazole-treated patients was 18% vs. 2% for placebo and the incidence of akathisia-related events for aripiprazole-treated patients was 3% vs. 9% for placebo.
In the pediatric (6 to 17 years) short-term autistic disorder trials, the Simpson Angus Rating Scale showed a significant difference between aripiprazole and placebo (aripiprazole, 0.1; placebo, -0.4). Changes in the Barnes Akathisia Scale and the Assessments of Involuntary Movement Scales were similar for the aripiprazole and placebo groups.
Agitation Associated with Schizophrenia or Bipolar Mania: In the placebo-controlled trials in patients with agitation associated with schizophrenia or bipolar mania, the incidence of reported EPS-related events excluding events related to akathisia for aripiprazole-treated patients was 2% vs. 2% for placebo and the incidence of akathisia-related events for aripiprazole-treated patients was 2% vs. 0% for placebo. Objectively collected data on the Simpson Angus Rating Scale (for EPS) and the Barnes Akathisia Scale (for akathisia) for all treatment groups did not show a difference between aripiprazole and placebo.
Dystonia: Class Effect: Symptoms of dystonia, prolonged abnormal contractions of muscle groups, may occur in susceptible individuals during the first few days of treatment. Dystonic symptoms include: spasm of the neck muscles, sometimes progressing to tightness of the throat, swallowing difficulty, difficulty breathing, and/or protrusion of the tongue. While these symptoms can occur at low doses, they occur more frequently and with greater severity with high potency and at higher doses of first generation antipsychotic drugs. An elevated risk of acute dystonia is observed in males and younger age groups.
Laboratory Test Abnormalities: A between group comparison for 3-week to 6-week, placebo-controlled trials in adults or 4-week to 8-week, placebo-controlled trials in pediatric patients (6 to 17 years) revealed no medically important differences between the aripiprazole and placebo groups in the proportions of patients experiencing potentially clinically significant changes in routine serum chemistry, hematology, or urinalysis parameters. Similarly, there were no aripiprazole/placebo differences in the incidence of discontinuations for changes in serum chemistry, hematology, or urinalysis in adult or pediatric patients.
ECG Changes: Between group comparisons for a pooled analysis of placebo-controlled trials in patients with schizophrenia, bipolar mania, or major depressive disorder revealed no significant differences between oral aripiprazole and placebo in the proportion of patients experiencing potentially important changes in ECG parameters. Aripiprazole was associated with a median increase in heart rate of 2 beats per minute compared to no increase among placebo patients.
In the pooled, placebo-controlled trials in patients with agitation associated with schizophrenia or bipolar mania, there were no significant differences between aripiprazole injection and placebo in the proportion of patients experiencing potentially important changes in ECG parameters, as measured by standard 12-lead ECGs.
Additional Findings Observed in Clinical Trials: Adverse Reactions in Long-Term, Double-Blind, Placebo-Controlled Trials: The adverse reactions reported in a 26-week, double-blind trial comparing oral ABILIFY and placebo in patients with schizophrenia were generally consistent with those reported in the short-term, placebo-controlled trials, except for a higher incidence of tremor [8% (12/153) for ABILIFY vs. 2% (3/153) for placebo]. In this study, the majority of the cases of tremor were of mild intensity (8/12 mild and 4/12 moderate), occurred early in therapy (9/12 <49 days), and were of limited duration (7/12 <10 days). Tremor infrequently led to discontinuation (<1%) of ABILIFY. In addition, in a long-term (52-week), active-controlled study, the incidence of tremor was 5% (40/859) for ABILIFY. A similar profile was observed in a long-term monotherapy study and a long-term adjunctive study with lithium and valproate in bipolar disorder.
Other Adverse Reactions Observed During the Premarketing Evaluation of Aripiprazole: Following is a list of MedDRA terms that reflect adverse reactions as defined previously in Overall Adverse Reactions Profile reported by patients treated with oral aripiprazole at multiple doses > 2 mg/day during any phase of a trial within the database of 13,543 adult patients. All events assessed as possible adverse drug reactions have been included with the exception of more commonly occurring events. In addition, medically/clinically meaningful adverse reactions, particularly those that are likely to be useful to the prescriber or that have pharmacologic plausibility, have been included. Events already listed in other parts of Adverse Reactions, or those considered in Precautions or Overdosage have been excluded. Although the reactions reported occurred during treatment with aripiprazole, they were not necessarily caused by it.
Events are further categorized by MedDRA system organ class and listed in order of decreasing frequency according to the following definitions: those occurring in at least 1/100 patients (only those not already listed in the tabulated results from placebo-controlled trials appear in this listing); those occurring in 1/100 to 1/1000 patients; and those occurring in fewer than 1/1000 patients.
Adults - Oral Administration: Blood and Lymphatic System Disorders: ≥1/1000 patients and <1/100 patients - leukopenia, neutropenia, thrombocytopenia.
Cardiac Disorders: ≥1/1000 patients and <1/100 patients - bradycardia, palpitations, cardiopulmonary failure, myocardial infarction, cardio-respiratory arrest, atrioventricular block, extrasystoles, sinus tachycardia, atrial fibrillation, angina pectoris, myocardial ischemia; <1/1000 patients - atrial flutter, supraventricular tachycardia, ventricular tachycardia.
Eye Disorders: ≥1/1000 patients and <1/100 patients - photophobia, diplopia, eyelid edema, photopsia.
Gastrointestinal Disorders: ≥1/1000 patients and <1/100 patients - gastroesophageal reflux disease, swollen tongue, esophagitis; <1/1000 patients - pancreatitis.
General Disorders and Administration Site Conditions: ≥1/100 patients - asthenia, peripheral edema, chest pain; ≥1/1000 patients and <1/100 patients - face edema, angioedema; <1/1000 patients -hypothermia.
Hepatobiliary Disorders: <1/1000 patients - hepatitis, jaundice.
Immune System Disorders: ≥1/1000 patients and <1/100 patients - hypersensitivity.
Injury, Poisoning, and Procedural Complications: ≥1/100 patients - fall; ≥1/1000 patients and <1/100 patients - self mutilation; <1/1000 patients - heat stroke.
Investigations: ≥1/100 patients - weight decreased, creatine phosphokinase increased; ≥1/1000 patients and <1/100 patients - hepatic enzyme increased, blood glucose increased, blood prolactin increased, blood urea increased, electrocardiogram QT prolonged, blood creatinine increased, blood bilirubin increased; <1/1000 patients - blood lactate dehydrogenase increased, glycosylated hemoglobin increased, gamma-glutamyltransferase increased.
Metabolism and Nutrition Disorders: ≥1/1000 patients and <1/100 patients - hyperlipidemia, anorexia, diabetes mellitus (including blood insulin increased, carbohydrate tolerance decreased, diabetes mellitus non-insulin-dependent, glucose tolerance impaired, glycosuria, glucose urine, glucose urine present), hyperglycemia, hypokalemia, hyponatremia, hypoglycemia, polydipsia; <1/1000 patients - diabetic ketoacidosis.
Musculoskeletal and Connective Tissue Disorders: ≥1/1000 patients and <1/100 patients - muscle rigidity, muscular weakness, muscle tightness, mobility decreased; <1/1000 patients - rhabdomyolysis.
Nervous System Disorders: ≥1/100 patients - coordination abnormal; ≥1/1000 patients and <1/100 patients - speech disorder, parkinsonism, memory impairment, cogwheel rigidity, cerebrovascular accident, hypokinesia, tardive dyskinesia, hypotonia, myoclonus, hypertonia, akinesia, bradykinesia; <1/1000 patients - Grand Mal convulsion, choreoathetosis.
Psychiatric Disorders: ≥1/100 patients - suicidal ideation; ≥1/1000 patients and <1/100 patients - aggression, loss of libido, suicide attempt, hostility, libido increased, anger, anorgasmia, delirium, intentional self injury, completed suicide, tic, homicidal ideation; <1/1000 patients - catatonia, sleep walking.
Renal and Urinary Disorders: ≥1/1000 patients and <1/100 patients - urinary retention, polyuria, nocturia.
Reproductive System and Breast Disorders: ≥1/1000 patients and <1/100 patients - menstruation irregular, erectile dysfunction, amenorrhea, breast pain; <1/1000 patients - gynaecomastia, priapism.
Respiratory, Thoracic, and Mediastinal Disorders: ≥1/100 patients - nasal congestion, dyspnea, pneumonia aspiration.
Skin and Subcutaneous Tissue Disorders: ≥1/100 patients - rash (including erythematous, exfoliative, generalized, macular, maculopapular, papular rash; acneiform, allergic, contact, exfoliative, seborrheic dermatitis, neurodermatitis, and drug eruption), hyperhydrosis; ≥1/1000 patients and <1/100 patients - pruritus, photosensitivity reaction, alopecia, urticaria.
Vascular Disorders: ≥1/100 patients - hypertension; ≥1/1000 patients and <1/100 patients - hypotension.
Pediatric Patients - Oral Administration: Most adverse events observed in the pooled database of 920 pediatric patients aged 6 to 17 years were also observed in the adult population. Additional adverse reactions observed in the pediatric population are listed as follows.
Gastrointestinal Disorders: ≥ 1/1000 patients and < 1/100 patients - tongue dry, tongue spasm.
Investigations: ≥ 1/100 patients - blood insulin increased.
Nervous System Disorders: ≥ 1/1000 patients and < 1/100 patients - sleep talking.
Skin and Subcutaneous Tissue Disorders: ≥ 1/1000 patients and < 1/100 patients - hirsutism.
Postmarketing Experience: The following adverse reactions have been identified during postapproval use of ABILIFY. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to establish a causal relationship to drug exposure: occurrences of allergic reaction (anaphylactic reaction, angioedema, laryngospasm, pruritus/urticaria, or oropharyngeal spasm), pathological gambling, hiccups and blood glucose fluctuation.
View ADR Monitoring Form