Special precautions for disposal and other handling: For reconstitution to a final concentration of 1 mg alteplase per ml the full volume of solvent provided should be transferred to the vial containing the Actilyse powder. To this purpose a transfer cannula is included with the 50 mg pack size, which is to be used.
For reconstitution to a final concentration of 2 mg alteplase per ml only half of the solvent provided should be used (as per the following table). In these cases always a syringe should be used to transfer the required amount of solvent to the vial containing the Actilyse powder.
Under aseptic conditions the content of an injection vial of Actilyse (50 mg) is dissolved with water for injections according to the following table to obtain either a final concentration of 1 mg alteplase/ml or 2 mg alteplase/ml: See Table 9.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The reconstituted solution should then be administered intravenously. The 1 mg/mL reconstituted solution may be diluted further with sterile sodium chloride 9 mg/ml (0.9 %) solution for injection up to a minimal concentration of 0.2 mg/ml since the occurrence of turbidity of the reconstituted solution cannot be excluded. A further dilution of the 1 mg/mL reconstituted solution with sterilised water for injections or in general, the use of carbohydrate infusion solutions, e.g. dextrose is not recommended due to increasing formation of turbidity of the reconstituted solution. Actilyse should not be mixed with other medicinal products in the same infusion-vial (not even with heparin).
For incompatibilities, see Incompatibilities as follows.
The reconstituted solution is for single use only. Any unused solution or waste material should be disposed in accordance with the local requirements.
Instructions for reconstituting Actilyse: 1. Reconstitute immediately before administration.
2. Remove the protective cap on the two vials containing the sterile water and Actilyse dry substance by flipping them up with a thumb.
3. Swab the rubber top of each vial with an alcohol wipe.
4. Remove the transfer cannula* from its cover. Do not disinfect or sterilize the transfer cannula; it is sterile. Take one cap off.
(*if a transfer cannula is included in the kit. The reconstitution can also be performed with a syringe and a needle.)
5. Stand the sterile water vial upright on a stable surface. From directly above, puncture the rubber stopper vertically in the stopper center with the transfer cannula, by pressing gently but firmly, without twisting.
6. Hold the sterile water vial and the transfer cannula steady with one hand using the two side flaps.
Remove the remaining cap on top of the transfer cannula.
7. Hold the sterile water vial and the transfer cannula steady with one hand using the two side flaps.
Hold the vial with Actilyse dry substance above the transfer cannula and position the tip of the transfer cannula right in the center of the stopper.
Push down the vial with the dry substance onto the transfer cannula from directly above, puncturing the rubber stopper vertically and gently but firmly without twisting.
8. Invert the two vials and allow the water to drain completely into the dry substance.
9. Remove the empty water vial together with the transfer cannula.
They can be disposed of.
10. Take the vial with reconstituted Actilyse and swirl gently to dissolve any remaining powder, but do not shake, as this will produce foam.
If there are bubbles, let the solution stand undisturbed for a few minutes to allow them to disappear.
11. The solution consists of 1mg/mL Actilyse. It should be clear and colourless to pale yellow and it should not contain any particles.
12. Remove the amount required using a needle and a syringe.
Do not use the puncture location from the transfer cannula to avoid leakage.
13. Use immediately.
Dispose of any unused solution.
Incompatibilities: The reconstituted solution may be diluted with sterile sodium chloride 9 mg/ml (0.9 %) solution for injection up to a minimal concentration of 0.2 mg alteplase per ml.
Further dilution, the use of water for injections for dilution or in general the use of carbohydrate infusion solutions, e.g. dextrose, is not recommended due to increasing formation of turbidity of the reconstituted solution.
Actilyse should not be mixed with other medicinal products neither in the same infusion vial nor the same catheter (not even with heparin).


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image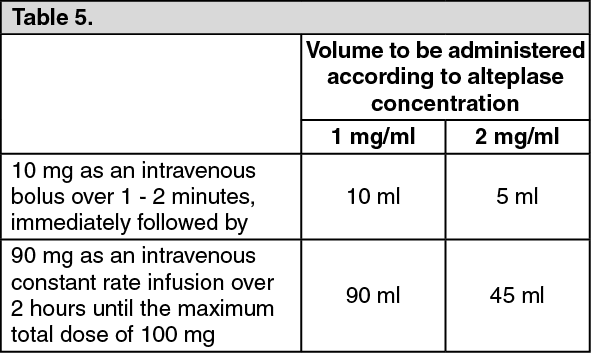 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image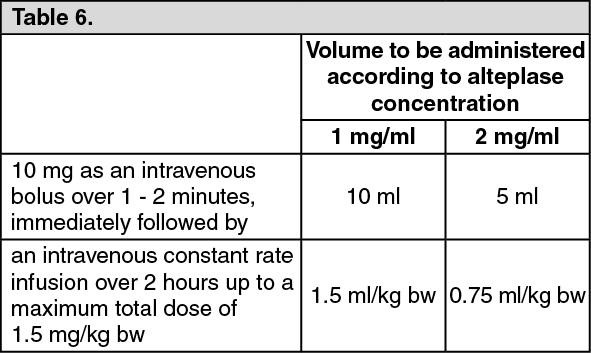 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image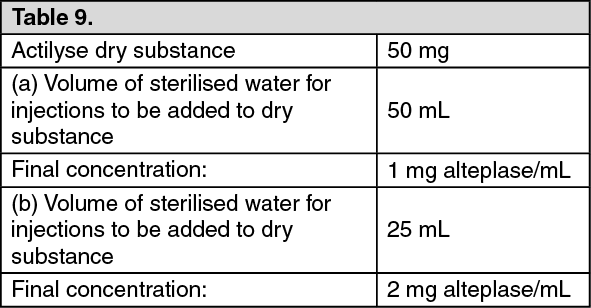 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
