Pharmacotherapeutic group: Cytokines, Interferons.
ATC Code: L03AB08.
Pharmacology: Pharmacodynamics: Mechanism of action: Interferons belong to the family of cytokines, which are naturally occurring proteins. Interferons have molecular weights ranging from 15,000 to 21,000 Daltons. Three major classes of interferons have been identified: alpha, beta, and gamma. Interferon alpha, interferon beta, and interferon gamma have overlapping yet distinct biologic activities. The activities of interferon beta-1b are species-restricted and therefore, the most pertinent pharmacological information on interferon beta-1b is derived from studies of human cells in culture or in human
in vivo studies.
Interferon beta-1b has been shown to possess both antiviral and immunoregulatory activities. The mechanisms by which interferon beta-1b exerts its actions in multiple sclerosis are not clearly understood. However, it is known that the biologic response-modifying properties of interferon beta-1b are mediated through its interactions with specific cell receptors found on the surface of human cells. The binding of interferon beta-1b to these receptors induces the expression of a number of gene products that are believed to be the mediators of the biological actions of interferon beta-1b. A number of these products have been measured in the serum and cellular fractions of blood collected from patients treated with interferon beta-1b. Interferon beta-1b both decreases the binding affinity and enhances the internalization and degradation of the interferon-gamma receptor. Interferon beta-1b also enhances the suppressor activity of peripheral blood mononuclear cells.
No separate investigations were performed regarding the influence of Betaferon on the cardiovascular system, respiratory system and the function of endocrine organs.
Clinical efficacy and safety: RR-MS: One controlled clinical trial with Betaferon in patients with relapsing-remitting multiple sclerosis and able to walk unaided (baseline EDSS 0 to 5.5) was performed. Patients receiving Betaferon showed a reduction in frequency (30%) and severity of clinical relapses, as well as the number of hospitalisations due to disease. Furthermore, there was a prolongation of the relapse-free interval. There is no evidence of an effect of Betaferon on the duration of relapses or on symptoms in between relapses, and no significant effect was seen on the progression of the disease in relapsing-remitting multiple sclerosis.
SP-MS: Two controlled clinical trials with Betaferon involving a total of 1,657 patients with secondary progressive multiple sclerosis (baseline EDSS 3 to 6.5, i.e. patients were able to walk) were performed. Patients with mild disease and those unable to walk were not studied. The two studies showed inconsistent results for the primary endpoint time to confirmed progression, representing delay of disability progression: One of the two studies demonstrated a statistically significant delay in the time to disability progression (Hazard Ratio = 0.69, 95% confidence interval (0.55, 0.86), p=0.0010, corresponding to a 31% risk reduction due to Betaferon) and in the time to becoming wheelchair bound (Hazard Ratio = 0.61, 95% confidence interval (0.44, 0.85), p=0.0036, corresponding to a 39% risk reduction due to Betaferon) in patients who received Betaferon. This effect continued over the observation period of up to 33 months. The treatment effect occurred in patients at all levels of disability investigated and independent of relapse activity.
In the second trial of Betaferon in secondary progressive multiple sclerosis, no delay in the time to disability progression was observed. There is evidence that the patients included in this study had overall less active disease than in the other study in secondary progressive multiple sclerosis.
In retrospective meta-analyses including the data of both studies, an overall treatment effect was found which was statistically significant (p=0.0076; 8.0 million IU Betaferon versus all placebo patients).
Retrospective analyses in subgroups showed that a treatment effect on disability progression is most likely in patients with active disease before treatment commences (Hazard Ratio 0.72, 95% confidence interval (0.59, 0.88), p=0.0011, corresponding to a 28 % risk reduction due to Betaferon in patients with relapses or pronounced EDSS progression, 8.0 million IU Betaferon versus all placebo patients).
From these retrospective subgroup analyses there was evidence to suggest that relapses as well as pronounced EDSS progression (EDSS >1 point or >0.5 point for EDSS ≥6 in the previous two years) can help to identify patients with active disease.
In both trials secondary progressive multiple sclerosis patients receiving Betaferon showed a reduction in frequency (30%) of clinical relapses. There is no evidence of Betaferon having an effect on the duration of relapses.
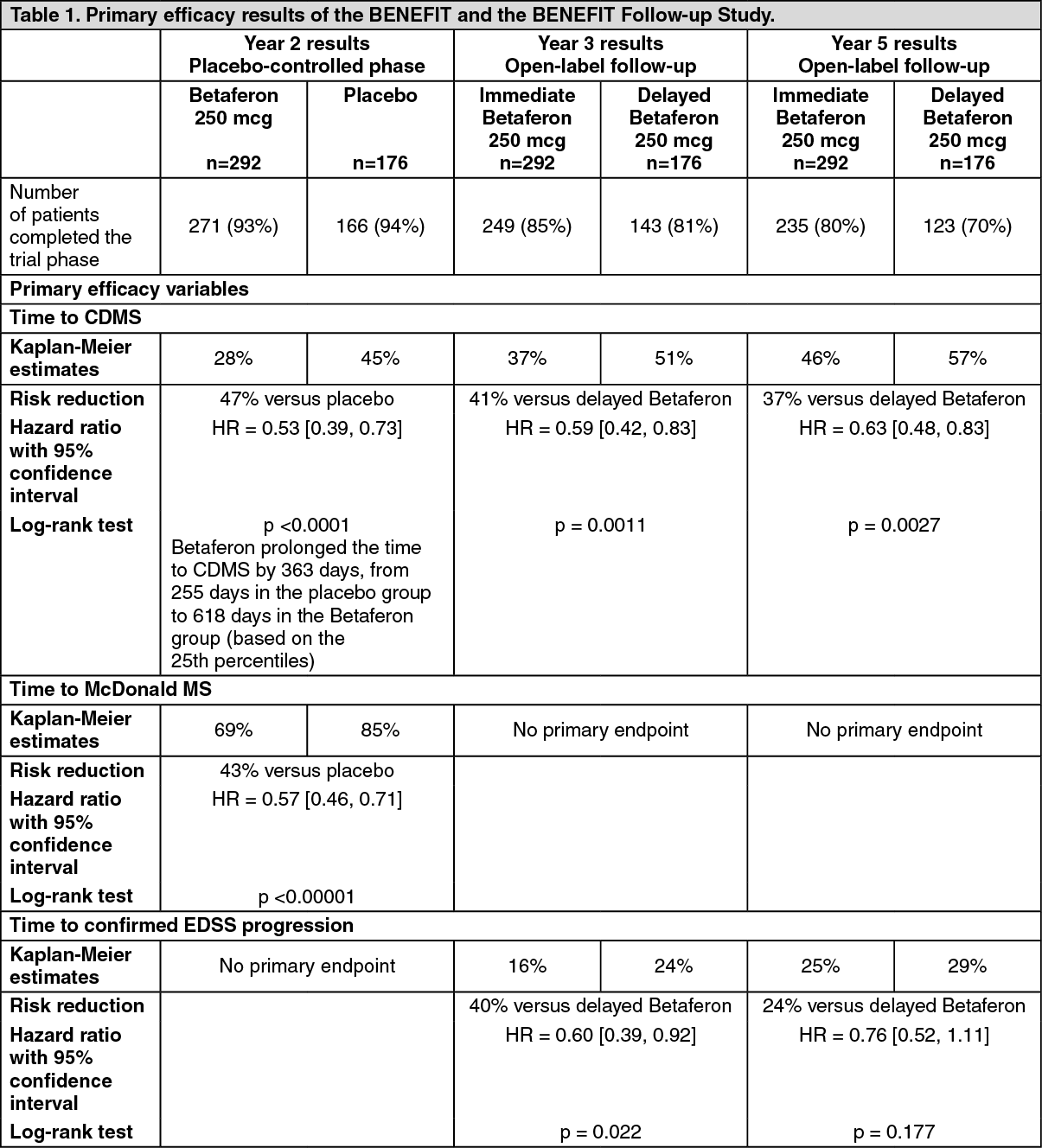
Single clinical event suggestive of MS: One controlled clinical trial with Betaferon was performed in patients with a single clinical event and MRI features suggestive of multiple sclerosis (at least two clinically silent lesions on the T2-weighted MRI). Patients with monofocal or multifocal onset of the disease were included (i.e. patients with clinical evidence for a single or at least two lesions, respectively, of the central nervous system). Any disease other than multiple sclerosis that could better explain signs and symptoms of the patient had to be excluded. This study consisted of two phases, a placebo-controlled phase followed by a pre-planned follow-up phase. The placebo-controlled phase lasted for 2 years or until the patient developed clinically definite multiple sclerosis (CDMS), whichever came first. After the placebo-controlled phase, patients entered a pre-planned follow-up phase with Betaferon to evaluate the effects of immediate versus delayed start of Betaferon-treatment, comparing patients initially randomized to Betaferon ("immediate treatment group") or to placebo ("delayed treatment group"). Patients and investigators remained blinded to the initial treatment allocation. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In the placebo-controlled phase, Betaferon delayed the progression from the first clinical event to CDMS in a statistically significant and clinically meaningful manner. The robustness of the treatment effect was also shown by the delay of progression to multiple sclerosis according to McDonald criteria (Table 1).
Subgroup analyses according to baseline factors demonstrated evidence of efficacy on progression to CDMS in all subgroups evaluated. The risk for progression to CDMS within 2 years was higher in monofocal patients with at least 9 T2-lesions or Gd-enhancement on brain MRI at baseline. In multifocal patients, the risk for CDMS was independent from MRI findings at baseline, indicating a high risk for CDMS because of the dissemination of the disease based on clinical findings. For the time being there is no well established definition of a high risk patient, although a more conservative approach is to accept at least nine T2 hyperintense lesions on the initial scan and at least one new T2 or one new Gd-enhancing lesion on a follow-up scan taken at least 1 month after the initial scan. In any case, treatment should only be considered for patients classified as high risk.
Therapy with Betaferon was well accepted as indicated by a high rate of trial completion (93% in the Betaferon group). To increase tolerability of Betaferon, a dose titration was applied and non-steroidal anti-inflammatory drugs were administered at start of therapy. Moreover, an autoinjector was used by the majority of patients throughout the study.
In the open label follow-up phase, the treatment effect on CDMS was still evident after 3 and 5 years (Table 1), even though the majority of patients from the placebo-group was treated with Betaferon at least from the second year onwards. EDSS progression (confirmed increase in EDSS of at least one point compared to baseline) was lower in the immediate treatment group (Table 1, significant effect after 3 years, no significant effect after 5 years). The majority of patients in both treatment groups had no disability progression over the 5-year period. Robust evidence for benefit on this outcome parameter could not be demonstrated for 'immediate' treatment. No benefit, attributable to immediate Betaferon treatment, in quality of life (as measured by FAMS - Functional Assessment of MS: Treatment Outcomes Index) was seen.
RR-MS, SP-MS and single clinical event suggestive of MS: Betaferon was effective in all multiple sclerosis studies to reduce disease activity (acute inflammation in the central nervous system and permanent tissue alterations) as measured by magnetic resonance imaging (MRI). The relation of multiple sclerosis disease activity as measured by MRI and clinical outcome is currently not fully understood.
Pharmacokinetics: Betaferon serum levels were followed in patients and volunteers by means of a not completely specific bioassay. Maximum serum levels of about 40 IU/ml were found 1-8 hours after subcutaneous injection of 500 microgram (16.0 million IU) interferon beta-1b. From various studies mean clearance rates and half-lives of disposition phases from serum were estimated to be at most 30 ml·min
-1·kg
-1 and 5 hours, respectively.
Betaferon injections given every other day do not lead to serum level increases, and the pharmacokinetics do not seem to change during therapy.
The absolute bioavailability of subcutaneously administered interferon beta-1b was approximately 50%.
Toxicology: Preclinical safety data: No acute toxicity studies have been carried out. As rodents do not react to human interferon beta, repeated dose studies were carried out with rhesus monkeys. Transitory hyperthermia was observed, as well as a significant rise in lymphocytes and a significant decrease in thrombocytes and segmented neutrophils.
No long-term studies have been conducted. Reproduction studies with rhesus monkeys revealed maternal toxicity and an increased rate of abortions, resulting in prenatal mortality. No malformations have been observed in the surviving animals.
No investigations on fertility have been conducted. No influence on the monkey oestrous cycle has been observed. Experience with other interferons suggest a potential for impairment of male and female fertility.
In one single genotoxicity study (Ames test), no mutagenic effect has been observed. Carcinogenicity studies have not been performed. An
in vitro cell transformation test gave no indication of tumorigenic potential.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image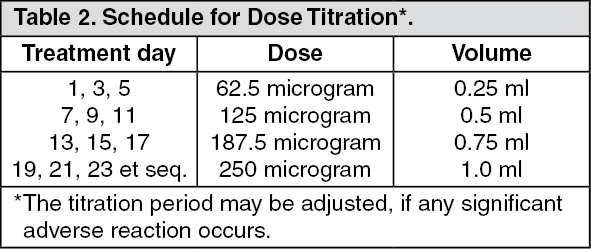 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out