


 Sign Out
Sign Out



Before treatment initiation, patients' left ventricular ejection fraction (LVEF) should be assessed by echocardiography (see Precautions). If LVEF is < 55%, treatment should not be initiated.
Before initiation of treatment, women of childbearing potential must have a negative pregnancy test (see Precautions and Use in Pregnancy & Lactation).
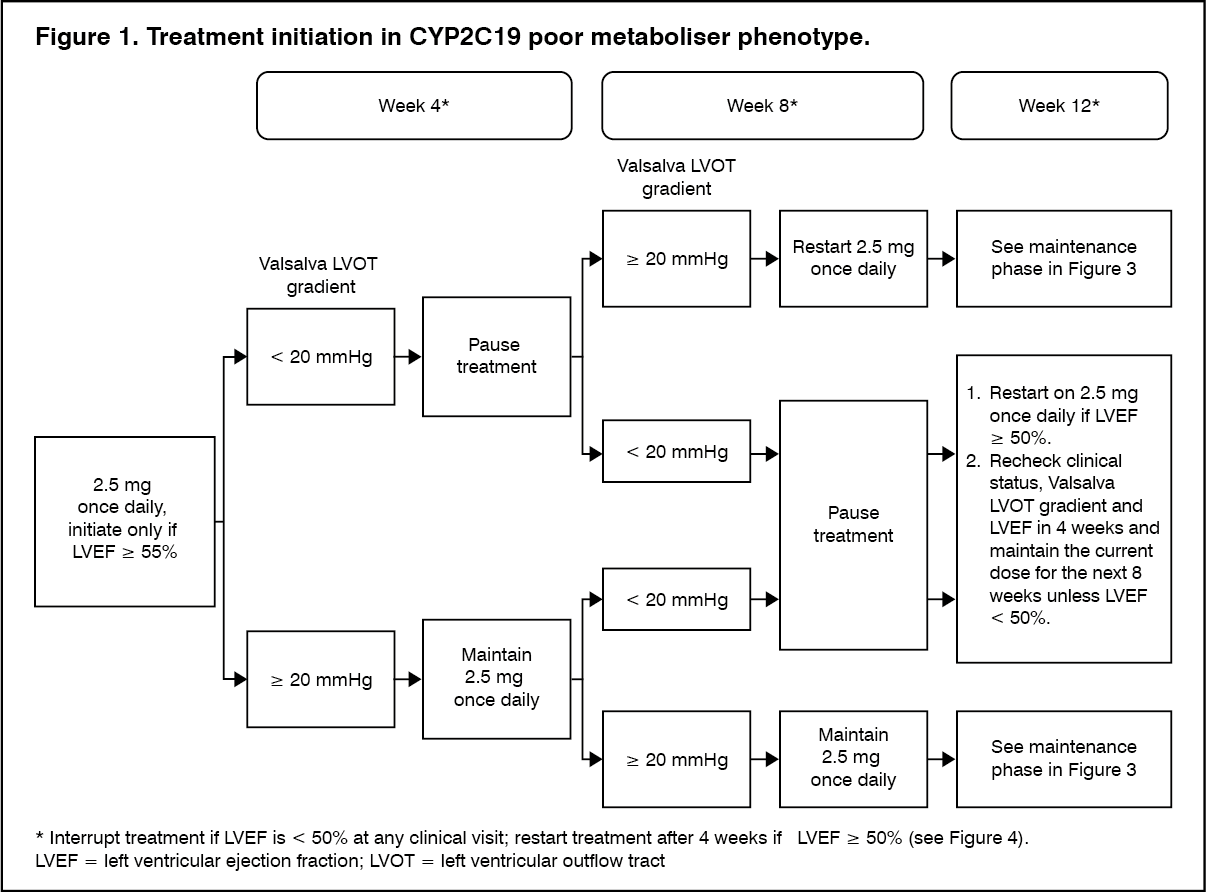
Patients should be genotyped for Cytochrome P450 (CYP) 2C19 (CYP2C19) in order to determine appropriate mavacamten dose. Patients with CYP2C19 poor metabolizer phenotype may have increased mavacamten exposures (up to 3 times) that can lead to increased risk of systolic dysfunction compared to normal metabolizers (see Precautions and Pharmacology: Pharmacokinetics under Actions). If treatment initiation occurs prior to determination of CYP2C19 phenotype, patients should follow dosing instructions for poor metabolisers (see Figure 1 and Table 4) until CYP2C19 phenotype is determined.
Posology: The dose range is 2.5 mg to 15 mg (either 2.5 mg, 5 mg, 10 mg or 15 mg). The bioequivalence between strengths has not been confirmed in a bioequivalence study in humans; therefore, the use of multiple capsules to achieve a prescribed dose is prohibited and one capsule of the appropriate dose strength should be used.
CYP2C19 poor metaboliser phenotype: The recommended starting dose is 2.5 mg orally once daily. The maximum dose is 5 mg once daily. The patient should be assessed for early clinical response by left ventricular outflow tract (LVOT) gradient with Valsalva manoeuvre 4 and 8 weeks after treatment initiation (see Figure 1).
CYP2C19 intermediate, normal, rapid and ultra-rapid metaboliser phenotype: The recommended starting dose is 5 mg orally once daily. The maximum dose is 15 mg once daily. The patient should be assessed for early clinical response by LVOT gradient with Valsalva manoeuvre 4 and 8 weeks after treatment initiation (see Figure 2).
Once an individualised maintenance dose is achieved, patients should be assessed every 12 weeks (see Figure 3). If at any visit the patient's LVEF is < 50%, the treatment should be interrupted for 4 weeks and until LVEF returns to ≥ 50% (see Figure 4).
In patients experiencing an intercurrent illness such as serious infection or arrhythmia (including atrial fibrillation or other uncontrolled tachyarrhythmia) which may impair systolic function, LVEF assessment is recommended, and dose increases are not recommended until intercurrent illness is resolved (see Precautions).
Consideration should be given to discontinue treatment in patients who have shown no response (e.g., no improvement in symptoms, quality of life, exercise capacity, LVOT gradient) after 4-6 months on the maximum tolerated dose.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image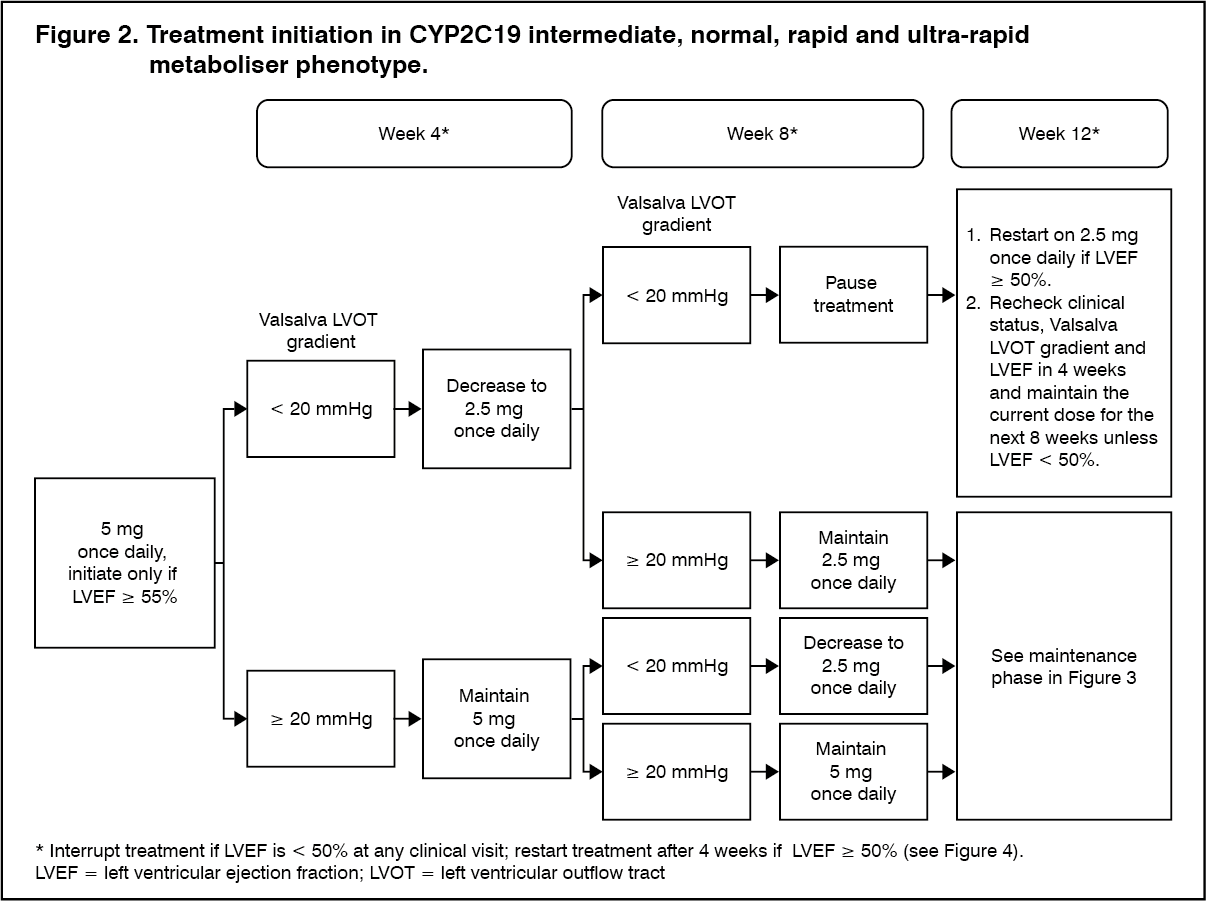 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image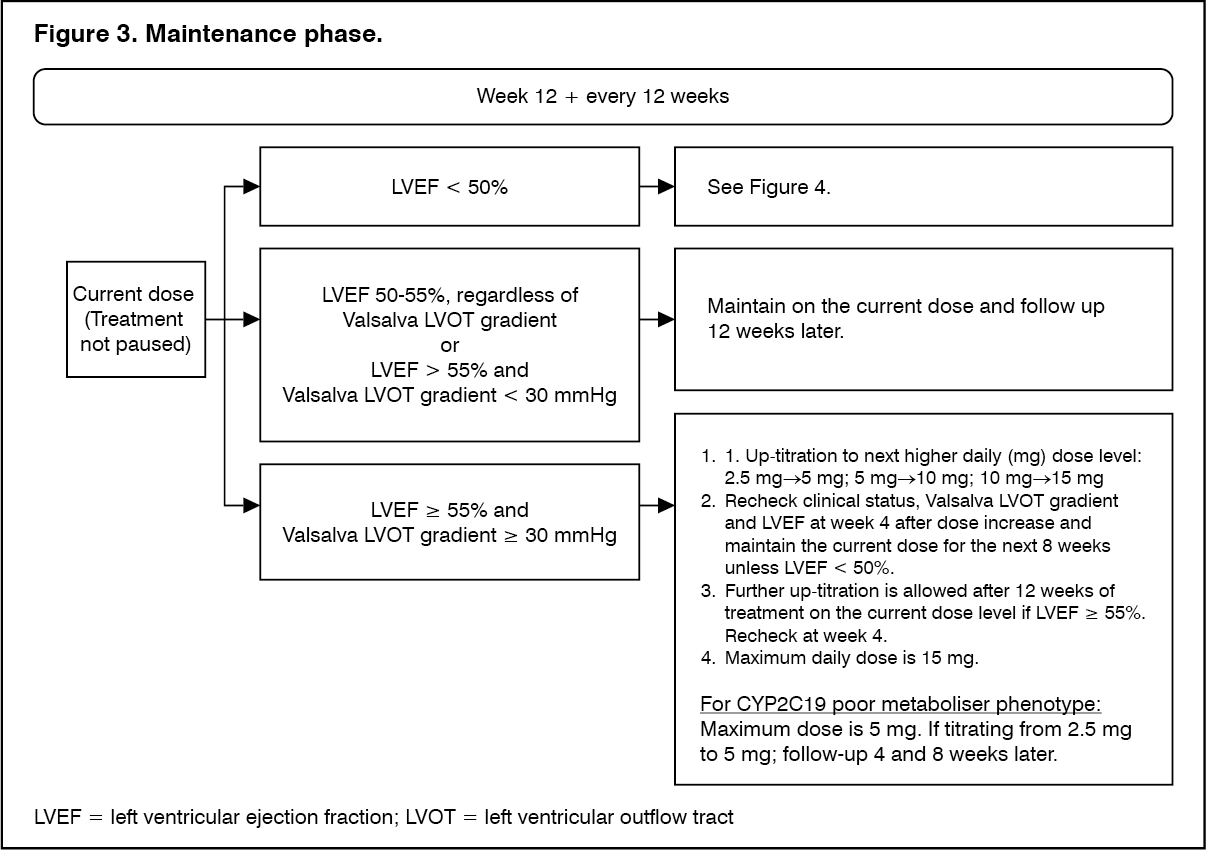 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image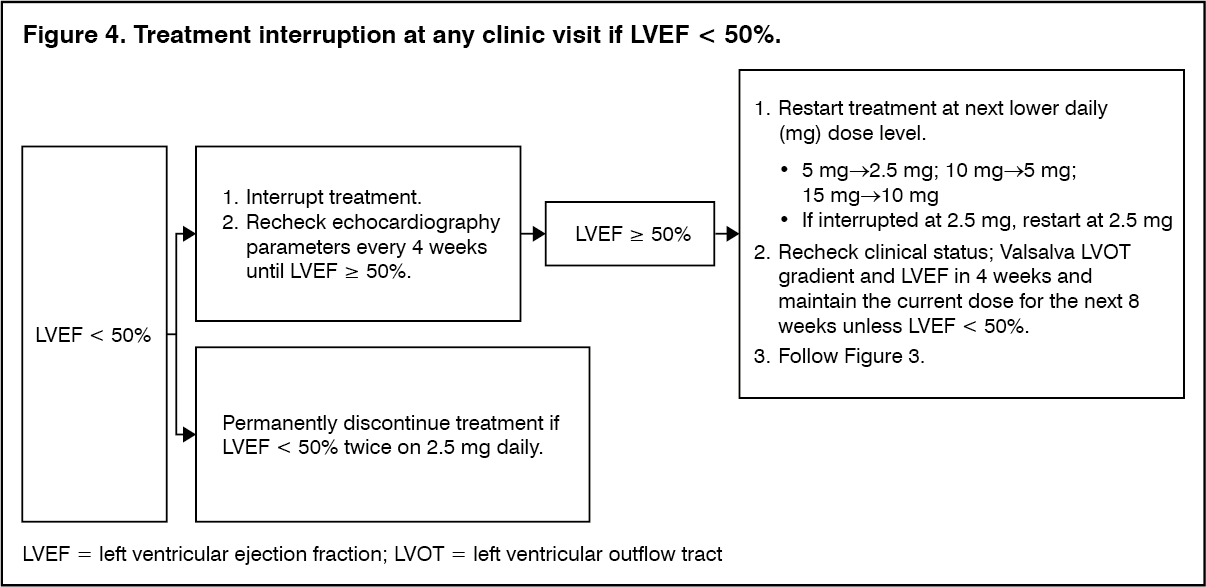 Click on icon to see table/diagram/image
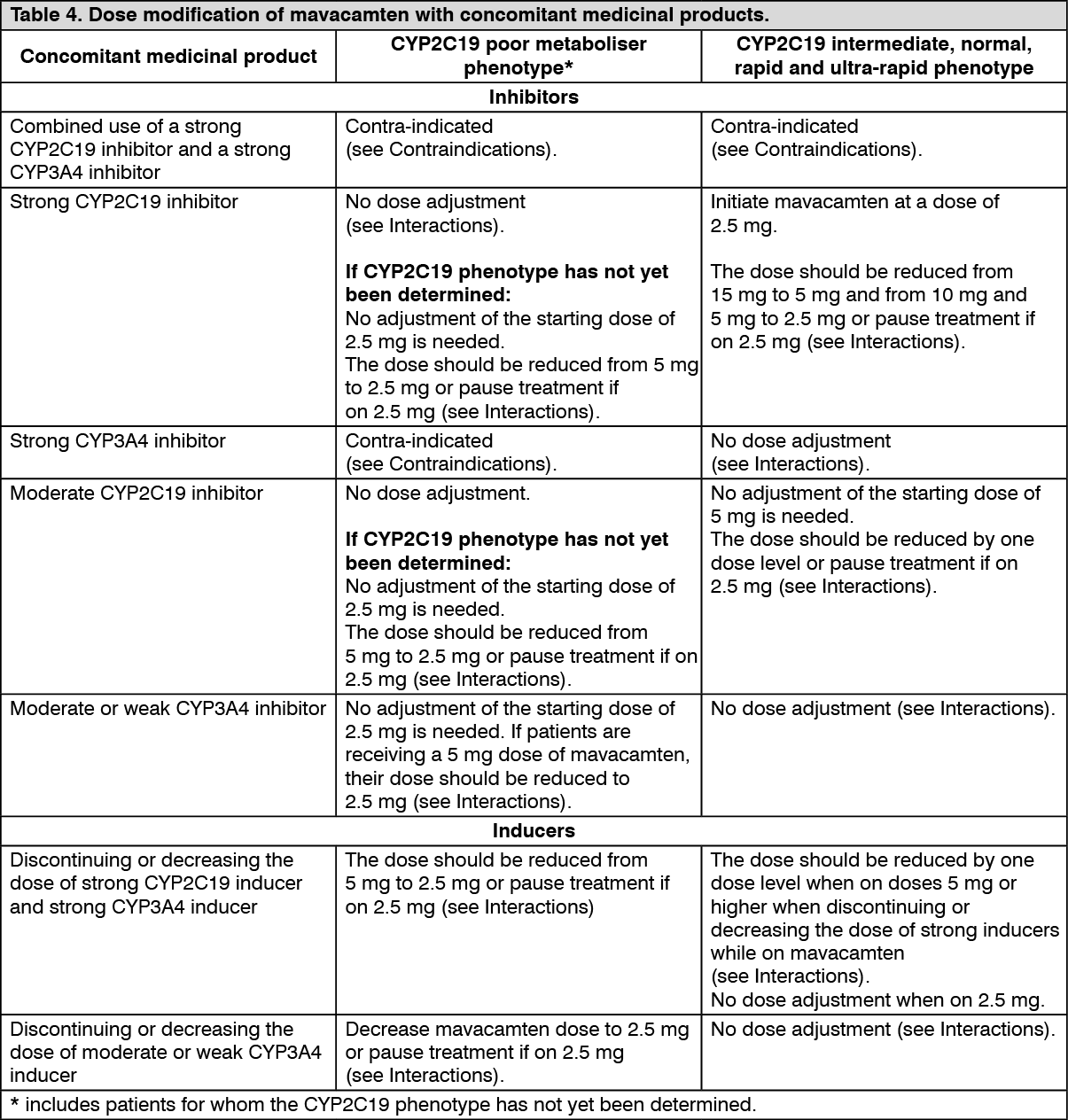
Click on icon to see table/diagram/imageDose modification with concomitant medicinal products: For concomitant treatment with inhibitors and inducers of CYP2C19 or CYP3A4, follow the steps shown in Table 4 (see also Interactions).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMissed or delayed doses: If a dose is missed, it should be taken as soon as possible, and the next scheduled dose should be taken at the usual time the following day. Two doses should not be taken on the same day.
Special populations: Elderly: No dose adjustment to the standard dose and titration scheme is required for patients aged 65 years and older (see Pharmacology: Pharmacokinetics under Actions).
Renal impairment: No dose adjustment to the standard dose and titration scheme is required for patients with mild (estimated glomerular filtration rate [eGFR] 60-89 mL/min/1.73m2) to moderate (eGFR 30-59 mL/min/1.73m2) renal impairment. No dose recommendation can be made for patients with severe (eGFR < 30 mL/min/1.73m2) renal impairment because mavacamten has not been studied in patients with severe renal impairment (see Pharmacology: Pharmacokinetics under Actions).
Hepatic impairment: The mavacamten starting dose should be 2.5 mg in all patients with mild (Child-Pugh class A) and moderate (Child-Pugh class B) hepatic impairment since mavacamten exposure is likely to be increased (see Pharmacology: Pharmacokinetics under Actions). No dose recommendation can be made for patients with severe hepatic impairment (Child-Pugh class C) because mavacamten has not been studied in patients with severe hepatic impairment (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Paediatric population: The safety and efficacy of mavacamten in children and adolescents below 18 years have not been established. No data are available.
Mavacamten should not be used in children less than 12 years because of potential safety concerns.
Method of administration: For oral use.
Treatment should be taken once daily with or without meals at about the same time each day. Use a single capsule for a prescribed dose. The capsule should be swallowed whole with water.