


 Sign Out
Sign Out
Pharmacology: Pharmacodynamics: Mechanism of action: Bicalutamide is a non-steroidal antiandrogen, devoid of other endocrine activity. It binds to the wild type or normal androgen receptor without activating gene expression, and thus inhibits the androgen stimulus. Regression of prostatic tumours results from this inhibition. Clinically, discontinuation of Casodex can result in antiandrogen withdrawal syndrome in a subset of patients.
Casodex is a racemate with its antiandrogenic activity being almost exclusively in the (R)-enantiomer.
150 mg: Clinical efficacy and safety: Casodex 150 mg was studied as a treatment for patients with localised (T1-T2, N0 or NX, M0) or locally advanced (T3-T4, any N, M0; T1-T2, N+, M0) non-metastatic prostate cancer in a combined analysis of three placebo controlled, double-blind studies in 8113 patients, where Casodex was given as immediate hormonal therapy or as adjuvant to radical prostatectomy or radiotherapy (primarily external beam radiation). At 9.7 years median follow up, 36.6% and 38.17% of all Casodex and placebo-treated patients, respectively, had experienced objective disease progression.
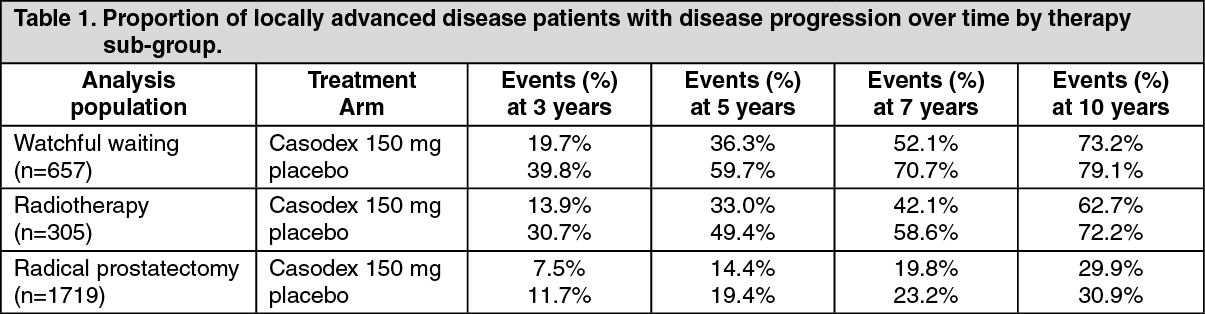
A reduction in risk of objective disease progression was seen across most patient groups but was most evident in those at highest risk of disease progression. Therefore, clinicians may decide that the optimum medical strategy for a patient at low risk of disease progression, particularly in the adjuvant setting following radical prostatectomy, may be to defer hormonal therapy until signs that the disease is progressing.
No overall survival difference was seen at 9.7 years median follow up with 31.4% mortality (HR= 1.01; 95% CI 0.94 to 1.09). However, some trends were apparent in exploratory subgroup analyses.
Data on progression-free survival and overall survival over time based on Kaplan-Meier estimates for patients with locally advanced disease are summarised in the following tables: See Tables 1 and 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image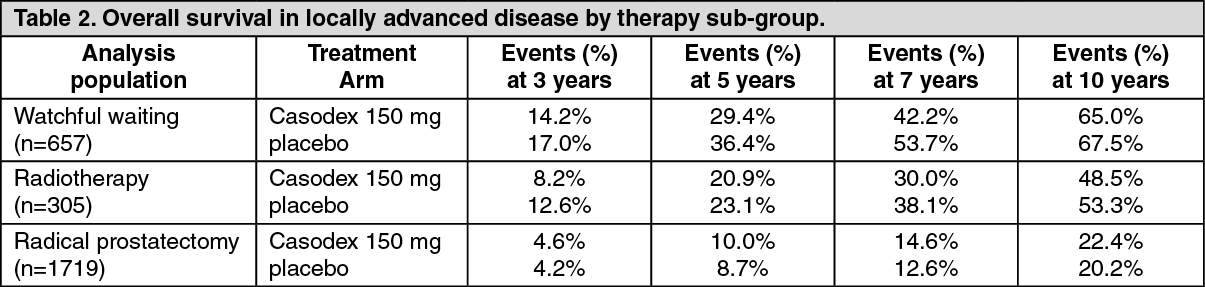 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor patients with localised disease receiving Casodex alone, there was no significant difference in progression free survival. There was no significant difference in overall survival in patients with localised disease who received Casodex as adjuvant therapy, following radiotherapy (HR=0.98; 95% CI 0.80 to 1.20) or radical prostatectomy (HR=1.03; 95% CI 0.85 to 1.25). In patients with localised disease, who would otherwise have been managed by watchful waiting, there was also a trend toward decreased survival compared with placebo patients (HR=1.15; 95% CI 1.00 to 1.32). In view of this, the benefit-risk profile for the use of Casodex is not considered favourable in patients with localised disease.
In a separate programme, the efficacy of Casodex 150 mg for the treatment of patients with locally advanced non-metastatic prostate cancer for whom immediate castration was indicated, was demonstrated in a combined analysis of 2 studies with 480 previously untreated patients with non-metastatic (M0) prostate cancer. At 56% mortality and a median follow-up of 6.3 years, there was no significant difference between Casodex and castration in survival (hazard ratio = 1.05 [CI 0.81 to 1.36]); however, equivalence of the two treatments could not be concluded statistically.
In a combined analysis of 2 studies with 805 previously untreated patients with metastatic (M1) disease at 43% mortality, Casodex 150 mg was demonstrated to be less effective than castration in survival time (hazard ratio = 1.30 [CI 1.04 to 1.65]), with a numerical difference in estimated time to death of 42 days (6 weeks) over a median survival time of 2 years.
Paediatric population: No studies have been conducted in paediatric patients (see Contraindications and Use in Pregnancy & Lactation).
Pharmacokinetics: Absorption: Bicalutamide is well absorbed following oral administration. There is no evidence of any clinically relevant effect of food on bioavailability.
Distribution: Bicalutamide is highly protein bound (racemate 96%, (R)-enantiomer >99%) and extensively metabolised (via oxidation and glucuronidation). Its metabolites are eliminated via the kidneys and bile in approximately equal proportions.
Biotransformation: The (S)-enantiomer is rapidly cleared relative to the (R)-enantiomer, the latter having a plasma elimination half-life of about 1 week.
On daily administration of Casodex, the (R)-enantiomer accumulates about 10-fold in plasma as a consequence of its long half-life.
Steady state plasma concentrations of the (R)-enantiomer of approximately 9 and 22 microgram/ml are observed during daily administration of Casodex 50 and 150 mg, respectively. At steady state, the predominantly active (R)-enantiomer accounts for 99% of the total circulating enantiomers.
Elimination: In a clinical study, the mean concentration of R-bicalutamide in semen of men receiving Casodex 150 mg was 4.9 microgram/ml. The amount of bicalutamide potentially delivered to a female partner during intercourse is low and by extrapolation possibly equates to approximately 0.3 microgram/kg. This is below that required to induce changes in offspring of laboratory animals.
Special Populations: The pharmacokinetics of the (R)-enantiomer are unaffected by age, renal impairment or mild to moderate hepatic impairment. There is evidence that for subjects with severe hepatic impairment, the (R)-enantiomer is more slowly eliminated from plasma.
Toxicology: Preclinical safety data: Bicalutamide is a potent antiandrogen and a mixed function oxidase enzyme inducer in animals. Target organ changes, including tumour induction (Leydig cells, thyroid, liver) in animals are related to these activities.
Atrophy of seminiferous tubules is a predicted class effect with antiandrogens and has been observed for all species examined. Reversal of testicular atrophy occurred 4 months after the completion of dosing in a 6-month rat study (at doses of approximately 1.5 and 0.6 times human therapeutic concentrations at the recommended doses of 50 and 150 mg, respectively). No recovery was observed at 24 weeks after the completion of dosing in a 12-month rat study (at doses of approximately 2 and 0.9 times human therapeutic concentrations at the recommended human doses of 50 and 150 mg, respectively). Following 12 months of repeated dosing in dogs (at doses of approximately 7 and 3 times human therapeutic concentrations at the recommended human doses of 50 and 150 mg, respectively), the incidence of testicular atrophy was the same in dosed and control dogs after a 6-month recovery period. In a fertility study (at doses of approximately 1.5 and 0.6 times human therapeutic concentrations at the recommended human doses of 50 and 150 mg, respectively), male rats had an increased time to successful mating immediately after 11 weeks of dosing; reversal was observed after 7 weeks off-dose.
150 mg: Enzyme induction has not been observed in man.