


 Sign Out
Sign Out
A dose-response relationship has been observed for the following adverse events: Sweating increased, dry mouth, insomnia, somnolence, diarrhoea, nausea and fatigue. The table as follows shows the adverse events in percentage associated with SSRIs and/or citalopram seen in either ≥1% of the patients in double-blind, placebo-controlled studies or seen as post-marketing events. (See table.)
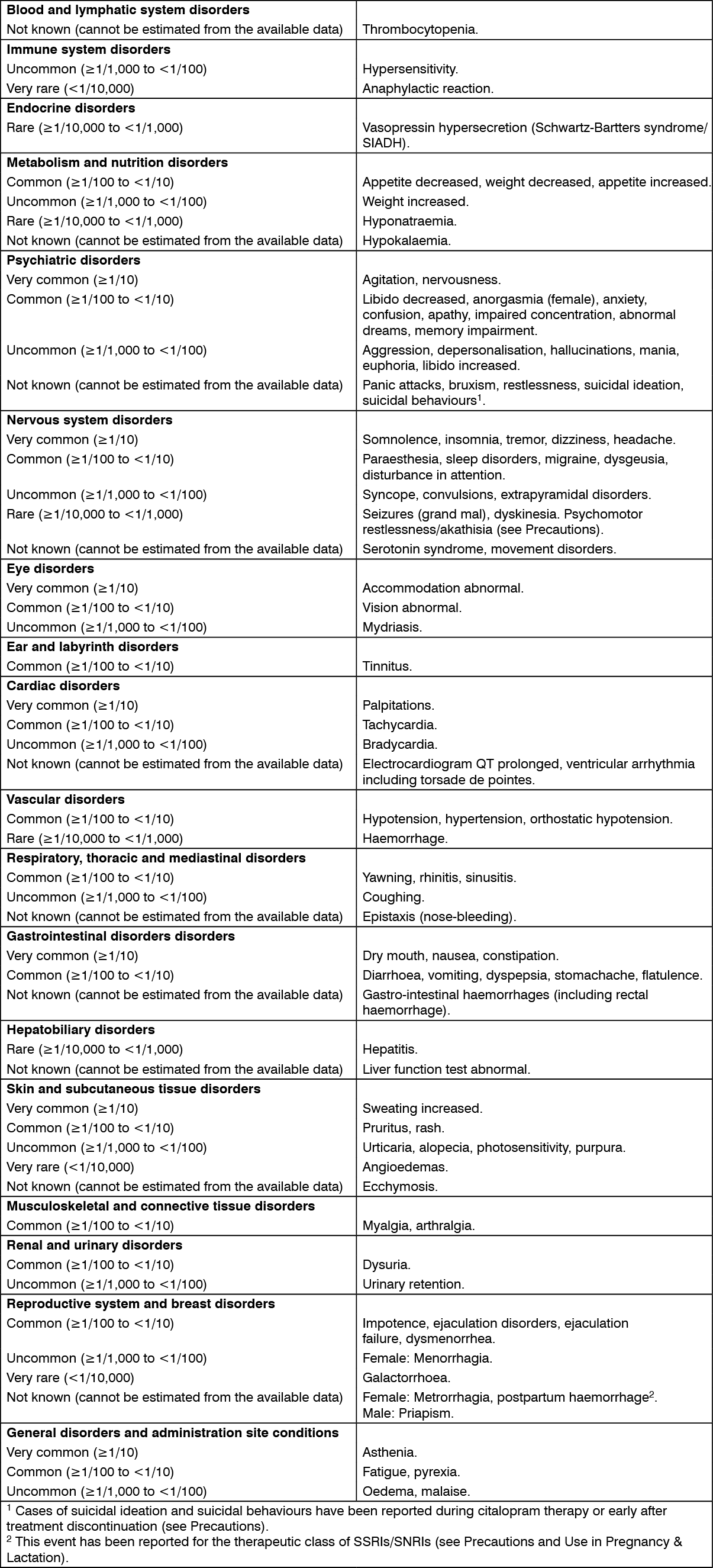 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageQT prolongation: Cases of QT prolongation and ventricular arrhythmia including torsade de pointes have been reported during the post-marketing period, predominantly in patients of female gender, with hypokalemia, or with pre-existing QT prolongation or other cardiac diseases (see Contraindications, Precautions, Interactions, Overdosage and Pharmacology: Pharmacodynamics under Actions).
Class effect - bone fractures: Epidemiological studies, mainly conducted in patients 50 years of age and older, show an increased risk of bone fractures in patients receiving SSRIs or tricyclic antidepressants. The mechanism leading to this risk is unknown.
Discontinuation symptoms seen when stopping SSRI treatment: Discontinuation of citalopram (particularly when abrupt) often leads to discontinuation symptoms. Dizziness, sensory disturbances (including paraesthesia), sleep disturbances (including insomnia and intense dreams), agitation or anxiety, nausea and/or vomiting, tremor, confusion, sweating, headache, diarrhoea, palpitations, emotional instability, irritability, and visual disturbances are the most commonly reported reactions. Generally, these events are mild to moderate and are self-limiting, however, in some patients they may be severe and/or prolonged. It is therefore advised that when citalopram treatment is no longer required, gradual discontinuation by dose tapering should be carried out (see Dosage & Administration and Precautions).
View ADR Monitoring Form