


 Sign Out
Sign Out
Pharmacology: Pharmacodynamics: Mechanism of action: As a fluoroquinolone antibacterial agent, the bactericidal action of ciprofloxacin results from the inhibition of both type II topoisomerase (DNA-gyrase) and topoisomerase IV, required for bacterial DNA replication, transcription, repair and recombination.
Pharmacokinetic/pharmacodynamic relationship: Efficacy mainly depends on the relation between the maximum concentration in serum (Cmax) and the minimum inhibitory concentration (MIC) of ciprofloxacin for a bacterial pathogen and the relation between the area under the curve (AUC) and the MIC.
Mechanism of resistance: In-vitro resistance to ciprofloxacin can be acquired through a stepwise process by target site mutations in both DNA gyrase and topoisomerase IV. The degree of cross-resistance between ciprofloxacin and other fluoroquinolones that results is variable. Single mutations may not result in clinical resistance, but multiple mutations generally result in clinical resistance to many or all active substances within the class. Impermeability and/or active substance efflux pump mechanisms of resistance may have a variable effect on susceptibility to fluoroquinolones, which depends on the physiochemical properties of the various active substances within the class and the affinity of transport systems for each active substance. All in-vitro mechanisms of resistance are commonly observed in clinical isolates. Resistance mechanisms that inactivate other antibiotics such as permeation barriers (common in Pseudomonas aeruginosa) and efflux mechanisms may affect susceptibility to ciprofloxacin.
Plasmid-mediated resistance encoded by qnr-genes has been reported.
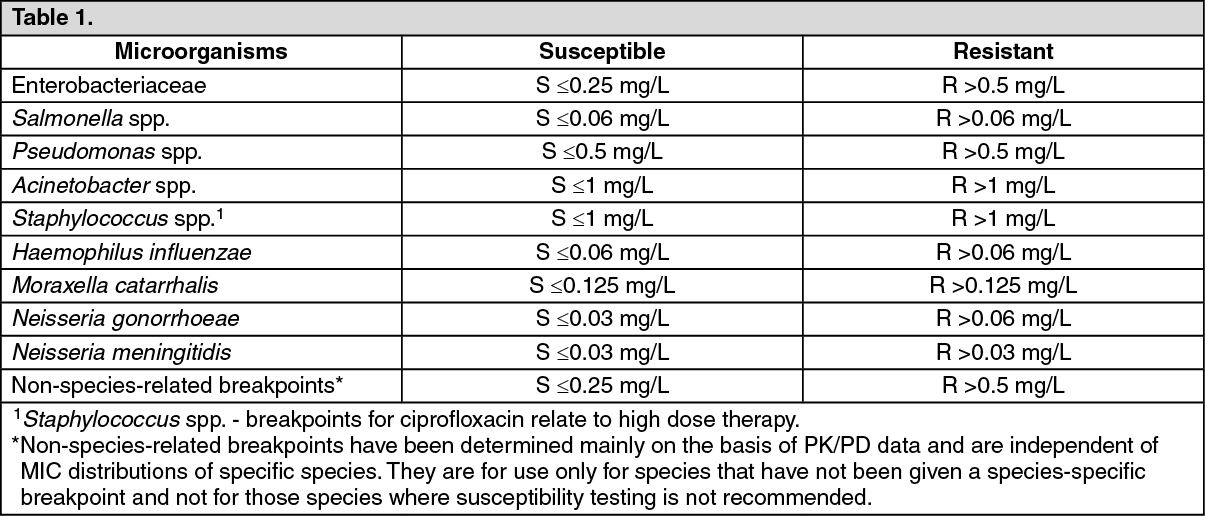
Spectrum of antibacterial activity: Breakpoints separate susceptible strains from strains with intermediate susceptibility and the latter from resistant strains: EUCAST Recommendations: See Table 1.
 Click on icon to see table/diagram/image
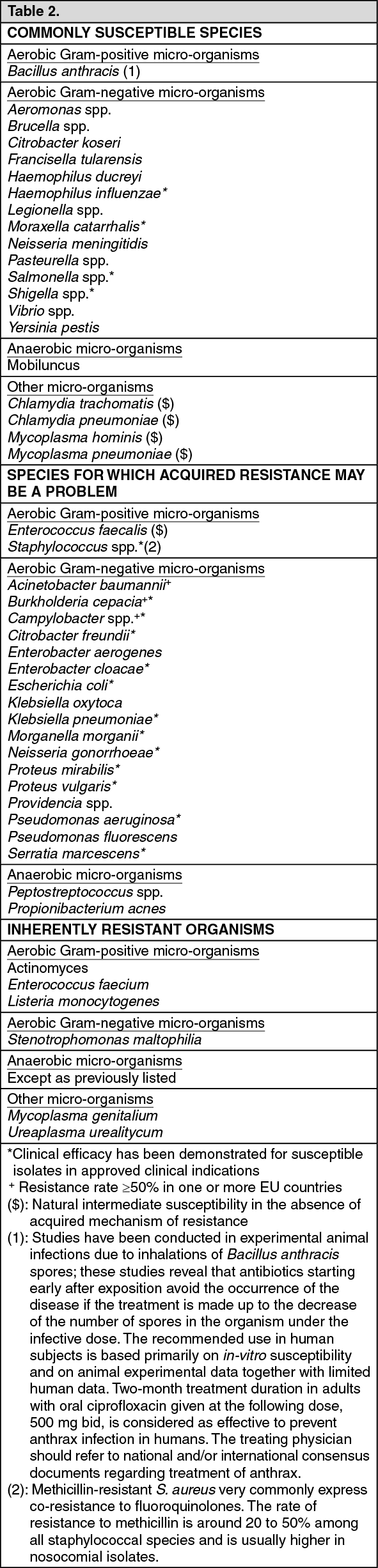
Click on icon to see table/diagram/imageThe prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent in at least some types of infections is questionable.
Groupings of relevant species according to ciprofloxacin susceptibility (for Streptococcus species see Precautions). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Absorption: Film-coated tablet: Following oral administration of single doses of 250 mg, 500 mg, and 750 mg of ciprofloxacin tablets, ciprofloxacin is absorbed rapidly and extensively, mainly from the small intestine, reaching maximum serum concentrations 1-2 hours later.
Single doses of 100-750 mg produced dose-dependent maximum serum concentrations (Cmax) between 0.56 and 3.7 mg/L. Serum concentrations increase proportionately with doses up to 1000 mg.
The absolute bioavailability is approximately 70-80%.
A 500 mg oral dose given every 12 hours has been shown to produce an area under the serum concentration-time curve (AUC) equivalent to that produced by an intravenous infusion of 400 mg ciprofloxacin given over 60 minutes every 12 hours.
Infusion: Following an intravenous infusion of ciprofloxacin the mean maximum serum concentrations were achieved at the end of infusion. Pharmacokinetics of ciprofloxacin were linear over the dose range up to 400 mg administered intravenously.
Comparison of the pharmacokinetic parameters for a twice a day and three times a day intravenous dose regimen indicated no evidence of drug accumulation for ciprofloxacin and its metabolites.
A 60-minute intravenous infusion of 200 mg ciprofloxacin or the oral administration of 250 mg ciprofloxacin, both given every 12 hours, produced an equivalent area under the serum concentration time curve (AUC).
A 60-minute intravenous infusion of 400 mg ciprofloxacin every 12 hours was bioequivalent to a 500 mg oral dose every 12 hours with regard to AUC.
The 400 mg intravenous dose administered over 60 minutes every 12 hours resulted in a Cmax similar to that observed with a 750 mg oral dose.
A 60-minute infusion of 400 mg ciprofloxacin every 8 hours is equivalent with respect to AUC to 750 mg oral regimen given every 12 hours.
Distribution: Protein binding of ciprofloxacin is low (20-30%). Ciprofloxacin is present in plasma largely in a non-ionised form and has a large steady state distribution volume of 2-3 L/kg body weight. Ciprofloxacin reaches high concentrations in a variety of tissues such as lung (epithelial fluid, alveolar macrophages, biopsy tissue), sinuses, inflamed lesions (cantharides blister fluid), and the urogenital tract (urine, prostate, endometrium) where total concentrations exceeding those of plasma concentrations are reached.
Biotransformation: Low concentrations of four metabolites have been reported, which were identified as: desethyleneciprofloxacin (M 1), sulphociprofloxacin (M 2), oxociprofloxacin (M 3) and formylciprofloxacin (M 4). The metabolites display in-vitro antimicrobial activity but to a lower degree than the parent compound.
Ciprofloxacin is known to be a moderate inhibitor of the CYP 450 1A2 iso-enzyme.
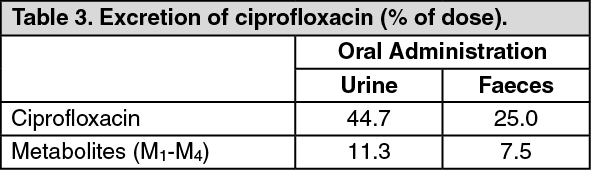
Elimination: Film-coated tablet: Ciprofloxacin is largely excreted unchanged both renally and, to a smaller extent, faecally. The serum elimination half-life in subjects with normal renal function is approximately 4-7 hours. (See Table 3.)
 Click on icon to see table/diagram/image
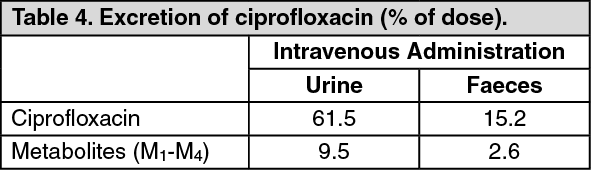
Click on icon to see table/diagram/imageInfusion: Ciprofloxacin is largely excreted unchanged both renally and, to a smaller extent, faecally. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRenal clearance is between 180-300 mL/kg/h and the total body clearance is between 480-600 mL/kg/h. Ciprofloxacin undergoes both glomerular filtration and tubular secretion. Severely impaired renal function leads to increased half lives of ciprofloxacin of up to 12 h.
Non-renal clearance of ciprofloxacin is mainly due to active trans-intestinal secretion and metabolism. 1% of the dose is excreted via the biliary route. Ciprofloxacin is present in the bile in high concentrations.
Paediatric patients: The pharmacokinetic data in paediatric patients are limited.
In a study in children Cmax and AUC were not age-dependent (above one year of age). No notable increase in Cmax and AUC upon multiple dosing (10 mg/kg three times daily) was observed.
In 10 children with severe sepsis Cmax was 6.1 mg/L (range 4.6-8.3 mg/L) after a 1-hour intravenous infusion of 10 mg/kg in children aged less than 1 year compared to 7.2 mg/L (range 4.7-11.8 mg/L) for children between 1 and 5 years of age. The AUC values were 17.4 mg*h/L (range 11.8-32.0 mg*h/L) and 16.5 mg*h/L (range 11.0-23.8 mg*h/L) in the respective age groups.
These values are within the range reported for adults at therapeutic doses. Based on population pharmacokinetic analysis of paediatric patients with various infections, the predicted mean half-life in children is approx. 4-5 hours and the bioavailability of the oral suspension ranges from 50 to 80%.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazards for humans based on conventional studies of single dose toxicity, repeated dose toxicity, carcinogenic potential, or toxicity to reproduction.
Like a number of other quinolones, ciprofloxacin is phototoxic in animals at clinically relevant exposure levels. Data on photomutagenicity/ photocarcinogenicity show a weak photomutagenic or phototumorigenic effect of ciprofloxacin in-vitro and in animal experiments. This effect was comparable to that of other gyrase inhibitors.
Articular tolerability: As reported for other gyrase inhibitors, ciprofloxacin causes damage to the large weight-bearing joints in immature animals. The extent of the cartilage damage varies according to age, species and dose; the damage can be reduced by taking the weight off the joints. Studies with mature animals (rat, dog) revealed no evidence of cartilage lesions. In a study in young beagle dogs, ciprofloxacin caused severe articular changes at therapeutic doses after two weeks of treatment, which were still observed after 5 months.