Clinical Trial Data: The safety profile presented as follows is based on data from more than 3500 subjects.
As has been observed for DTPa and DTPa-containing combinations, an increase in local reactogenicity and fever was reported after booster vaccination with Infanrix-IPV+Hib with respect to the primary course.
Adverse reactions reported are listed according to the following frequency: Very common ≥1/10; Common ≥1/100 and <1/10; Uncommon ≥1/1000 and <1/100; Rare ≥1/10000 and <1/1000; Very rare <1/10000.
Infections and infestations: Uncommon: Upper respiratory tract infection.
Blood and lymphatic system disorders: Uncommon: lymphadenopathy.
Metabolism and nutrition disorders: Very common: appetite lost.
Psychiatric disorders: Very common: irritability, crying abnormal, restlessness.
Nervous system disorders: Very common: somnolence.
Respiratory, thoracic and mediastinal disorders: Uncommon: cough, bronchitis, rhinorrhoea.
Gastrointestinal disorders: Common: diarrhoea, vomiting.
Skin and subcutaneous tissue disorders: Uncommon: rash, urticaria.
Rare: pruritus, dermatitis.
General disorders and administration site conditions: Very common: injection site reactions such as pain and redness, local swelling at the injection site (≤50 mm), fever (≥38.0°C).
Common: injection site reactions including induration, local swelling at the injection site (>50 mm)
1.
Uncommon: fever >39.5°C
2, fatigue, diffuse swelling of the injected limb, sometimes involving the adjacent joint
1.
Post-marketing data: Respiratory, thoracic and mediastinal disorders: Apnoea
3 [see Precautions for apnoea in very premature infants (≤28 weeks of gestation)].
Blood and lymphatic system disorders: Thrombocytopenia
4.
Immune system disorders: Allergic reactions (including anaphylactic
3 and anaphylactoid reactions).
Nervous system disorders: Convulsions (with or without fever), collapse or shock-like state (hypotonic-hyporesponsiveness episode).
Skin and subcutaneous tissue disorders: Angioneurotic oedema
3.
General disorders and administration site conditions: Swelling of the entire injected limb
1, injection site vesicles
3.
1 Children primed with acellular pertussis vaccines are more likely to experience swelling reactions after booster administration in comparison with children primed with whole cell vaccines. These reactions resolve over an average of 4 days.
2 common with booster vaccination.
3 reported with GSK's DTPa containing vaccines.
4 reported with D and T vaccines.


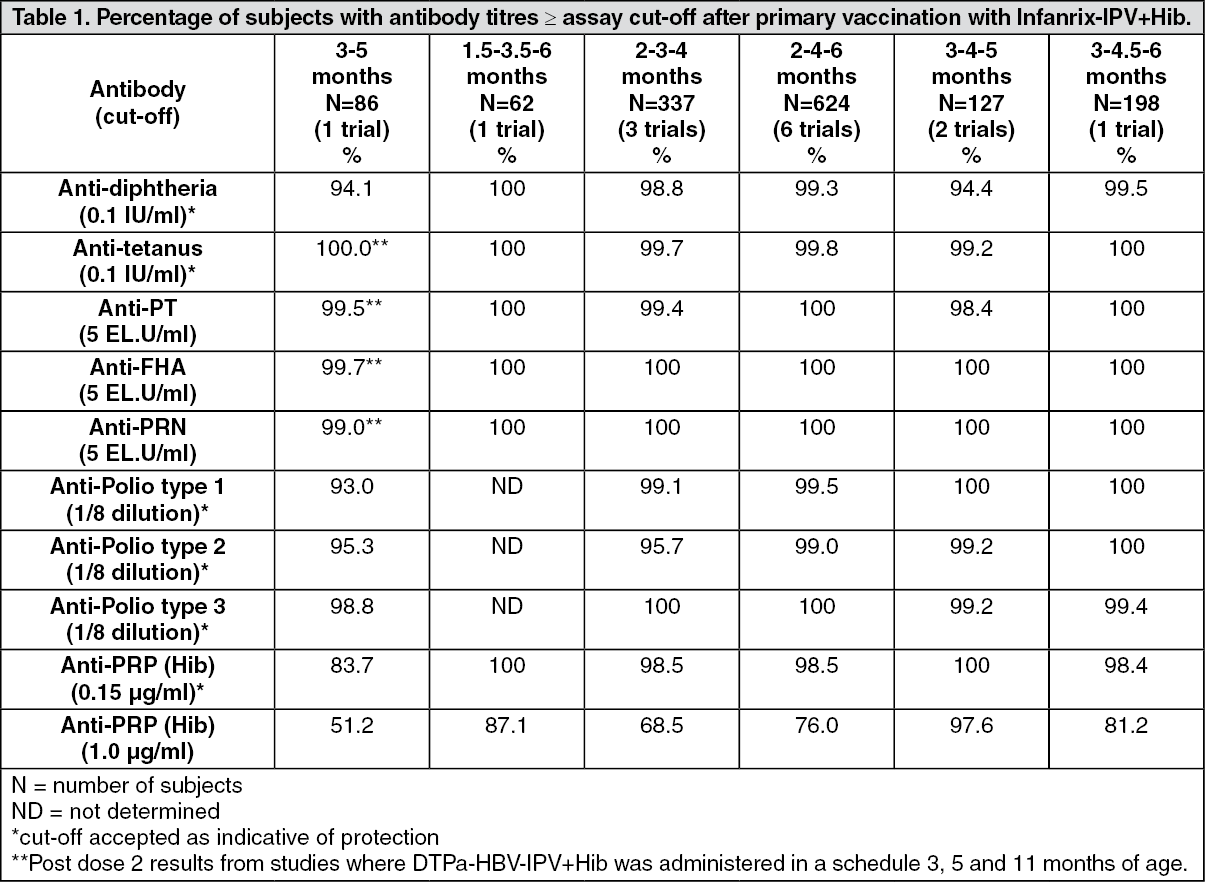 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image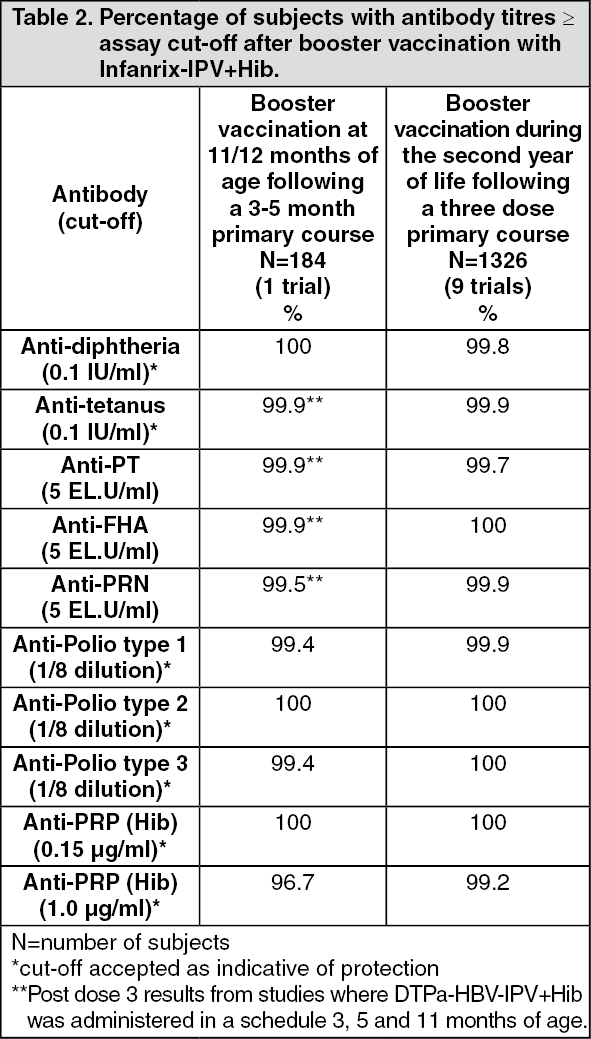 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
