Each tablet contains 10 mg or 25 mg nortriptyline (as 11.38 mg and 28.45 mg nortriptyline hydrochloride, respectively).
Excipients/Inactive Ingredients: Tablet core: Maize starch, Lactose monohydrate, Copovidone, Glycerol (85%), Cellulose microcrystalline, Talc, Magnesium stearate.
Coating: Hypromellose 5, Macrogol 6000.
Colour: Titanium dioxide (E 171).
Pharmacotherapeutic group: Antidepressants - Non-selective monoamine reuptake inhibitor (tricyclic antidepressant). ATC-code: N 06 AA 10.
Pharmacology: Pharmacodynamics: Mechanism of action: Nortriptyline is a tricyclic antidepressant. Nortriptyline, a secondary amine, is also the main active metabolite of amitriptyline. Nortriptyline is a more potent inhibitor of noradrenaline than of serotonin uptake, while amitriptyline inhibits the uptake of noradrenaline and serotonin equally well. Nortriptyline is less anticholinergic than amitriptyline but has quite potent antihistaminergic effect and it potentiates the effects of catecholamines.
Suppression of rapid eye movement (REM) sleep is considered a predictor of antidepressant activity. Tricyclic antidepressants, as well as SSRIs and MAO inhibitors, suppresses REM-sleep and increases deep slow-wave sleep.
Clinical efficacy: Nortriptyline elevates the pathological lowered mood level. Due to its central stimulating properties nortriptyline is of special value in depressions when inhibition, apathy and lack of initiative are features of the illness. The antidepressant effect usually sets in after 2-4 weeks, whereas release of inhibition may set in considerably sooner. Among tricyclics, nortriptyline may have a particularly low risk of inducing orthostatic changes.
Pharmacokinetics: Absorption: Oral administration results in maximum plasma levels in about 5 hours (Tmax = 5.5±1.9 hours; range 4.0-8.8 hours). The mean absolute oral bioavailability is 51% (Fabs = 0.51±0.05; range 0.46-0.59).
Distribution: The apparent volume of distribution (Vd)β estimated after intravenous administration is 1633±268 l; range 1460-2030 l (21±4 l/kg). The plasma protein binding is about 93 %.
Nortriptyline passes across the placental barrier.
Biotransformation: The metabolism of nortriptyline proceeds by demethylation and hydroxylation followed by conjugation with glucuronic acid. The metabolism is subject to genetic polymorphism (CYP2D6).
The main active metabolite is 10-hydroxynortriptyline, which exists in a cis and trans form with the trans form dominating in the organism. N-demethylnortriptyline is also formed to some degree. The metabolites have the same profile as nortriptyline but are somewhat weaker. Trans 10-hydroxynortriptyline is more potent than the cis form. In plasma the amount of total 10-hydroxynortriptyline dominates but most of the metabolites are conjugated.
Elimination: The elimination half-life (T½ β) of nortriptyline after peroral administration is about 26 hours (25.5±7.9 hours; range 16-38 hours). The mean systemic clearance (Cls) is 30.6±6.9 l/h; range 18.6-39.6 l/h.
The excretion proceeds mainly with urine. The renal elimination of unchanged nortriptyline is insignificant (about 2%).
In nursing mothers nortriptyline is excreted in small amounts with the breast milk. The ratio milk conc./plasma conc. in women is 1:2. The estimated daily infant exposure averages 2% of the corresponding maternal weight-related doses of nortriptyline (in mg/kg).
Steady state plasma levels of nortriptyline are reached within a week for most patients.
Elderly patients: Longer half-lives and decreased oral (Clo) clearance values due to a reduced rate of metabolism have been demonstrated in elderly patients.
Reduced hepatic function: Hepatic affection of a certain degree of severity may reduce hepatic extraction resulting in higher plasma levels.
Reduced renal function: Renal failure has no influence on the kinetics.
Polymorphism: The metabolism is subject to genetic polymorphism (CYP2D6).
Pharmacokinetic / Pharmacodynamic relationship: The therapeutic plasma concentration in endogenous depression is 50-140 ng/ml (~ 190-530 nmol/l). Levels above 170-200 ng/ml are associated with increased risk of disturbance in cardiac conduction in terms of prolonged QRS-complex or AV block.
Toxicology: Preclinical safety data: Acute toxicity: The acute toxicity of tricyclic antidepressants including nortriptyline is high.
LD50 of nortriptyline hydrochloride in rats was 502 mg/kg p.o.
Nortriptyline has been used clinically since 1963.
Major depressions, especially when inhibition, apathy and lack of initiative are features of the illness.
Depressive states in schizophrenics used in combination with a neuroleptic to prevent exacerbation of hallucinations and paranoid delusions.
Dosage should be initiated at a low level and increased gradually, noting carefully the clinical response and any evidence of intolerability. Dosages exceeding 150 mg/day should preferably be restricted to hospitalised patients (up to 200-250 mg).
Adults: Initially 50 mg once a day administered in the morning or 25 mg 2-3 times daily gradually increased, if necessary, by 25 mg every other day up to 100-150 mg once a day or 50 mg 2-3 times daily (rarely 200 mg daily in hospitalised patients). The additional doses are primarily administered in the morning.
The maintenance dose is the same as the optimal therapeutic dose.
Elderly patients: Patients over 60 years of age: Initially 10 mg 2-3 times daily or 25 mg once a day, gradually increased, if necessary, every other day up to 150 mg daily. The additional doses are primarily administered in the morning.
The maintenance dose is the same as the optimal therapeutic dose.
Children and adolescents (<18 years): Nortrilen is not recommended for use in children and adolescents due to lack of data on safety and efficacy.
Reduced renal function: Nortriptyline can be given in usual doses to patients with renal failure.
Reduced liver function: Careful dosing and, if possible, a serum level determination is advisable.
Duration of treatment: The antidepressant effect usually sets in after 2 to 4 weeks. Treatment with antidepressants is symptomatic and must therefore be continued for an appropriate length of time usually up to 6 months after recovery in order to prevent relapse. In patients with recurrent depression (unipolar) maintenance therapy may need to be continued for a number of years to prevent new episodes.
Discontinuation: When stopping therapy the drug should be gradually withdrawn during several weeks.
Method of administration: Dose increases are made preferably in the morning.
The tablets are swallowed with water.
There is considerably individual variability in response to overdose.
Children are especially susceptible to cardiotoxicity and seizures.
In adults more than 500 mg have caused moderate to serious intoxication and less than 1000 mg have been fatal.
Symptoms: The symptoms can occur slowly and insidious or abruptly and surprisingly. During the first hours somnolence or excitation, agitation and hallucinations.
Anticholinergic symptoms: Mydriasis, tachycardia, urinary retention, dry mucous membranes, reduced bowel motility. Convulsions. Fever. Sudden occurrence of CNS depression. Lowered consciousness progressing into coma. Respiratory depression.
Cardiac symptoms: Arrhythmias (ventricular tachyarrhythmias, torsade de pointes, ventricular fibrillation). The ECG characteristically show prolonged PR interval, widening of the QRS-complex, QT prolongation, T-wave flattening or inversion, ST segment depression, and varying degrees of heart block progressing to cardiac standstill. Widening of the QRS-complex usually correlates well with the severity of the toxicity following acute overdoses. Heart failure, hypotension, cardiogenic shock. Metabolic acidosis, hypokalemia.
During awakening possibly again confusion, agitation and hallucinations and ataxia.
Treatment: Patients should be admitted to hospital (intensive care unit) and closely monitored even in apparently uncomplicated cases. The treatment is symptomatic and supportive.
ABC's (airway, breathing and circulation) should be assessed and treated as appropriate. Patency of the airway is maintained by intubation, where required. Treatment in a respirator is advised to prevent a possible respiratory arrest. Continuous ECG-monitoring of cardiac function for 3-5 days is advised. Urea and electrolytes should be checked, in particular for low potassium. Urine output should be monitored. Arterial blood gases should be checked, in particular for acidosis. Consider gastric lavage only if within one hour of a potentially fatal overdose. Give 50 g of charcoal if within one hour of ingestion.
Treatment of the following will be decided on a case by case basis: Wide QRS-intervals, cardiac failure and ventricular arrhythmias; Circulatory failure; Hypotension; Hyperthermia; Convulsions; Metabolic acidosis.
Unrest and convulsions may be treated with diazepam.
Patients who display signs of toxicity should be monitored for a minimum of 12 hours. Monitor for rhabdomyolysis if the patient has been unconscious for a considerable time. Since overdosage is often deliberate, patients may attempt suicide by other means during the recovery phase. Deaths by deliberate or accidental overdosage have occurred with this class of medicament.
Hypersensitivity to the active substance or to any of the excipients listed in Description.
Recent myocardial infarction, any degree of heart block, conduction disturbances affecting the heart rhythm and coronary artery insufficiency.
Concomitant or recent treatment with MAOIs (monoamine oxidase inhibitors) (see Interactions).
Nortriptyline should not be administered together with MAOIs (see Contraindications and Interactions).
Cardiac arrhythmias are likely to occur with high dosage. They may also occur in patients with pre-existing heart disease taking normal dosage.
Nortriptyline should be used with caution in patients with convulsive disorders, urinary retention, prostatic hypertrophy, hyperthyroidism, paranoid symptomatology, and advanced hepatic or cardiovascular disease.
Serotonergic psychiatric drugs should not be started in a patient receiving linezolid. Wait until 24 hours after the last dose of linezolid before starting the serotonergic psychiatric drugs.
Suicide/suicidal thoughts or clinical worsening: Depression is associated with an increased risk of suicidal thoughts, self-harm and suicide (suicide-related events.). This risk persist until significant remission occurs. As improvement may not occur during the first few weeks or more of treatment, patients should be closely monitored until such improvement occurs. It is general clinical experience that the risk of suicide may increase in the early stages of recovery.
Patients with a history of suicide-related events, or those exhibiting a significant degree of suicidal ideation prior to commencement of treatment, are known to be at greater risk of suicidal thoughts or suicide attempts, and should receive careful monitoring during treatment. A meta-analysis of placebo-controlled clinical trials of antidepressant drugs in adult patients with psychiatric disorders showed an increased risk of suicidal behaviour with antidepressants compared to placebo in patients less than 25 years old.
Close supervision of patients and in particular those at high risk should accompany drug therapy especially in early treatment and following dose changes. Patients (and caregivers of patients) should be alerted about the need to monitor for any clinical worsening, suicidal behaviour or thoughts and unusual changes in behaviour and to seek medical advice immediately if these symptoms present.
Great care is necessary if nortriptyline is administered to hyperthyroid patients or to those receiving thyroid medication, since cardiac arrhythmias may develop.
Elderly patients are particularly susceptible to orthostatic hypotension. However, nortriptyline is less inclined than other tricyclic antidepressants to cause orthostatic hypotension.
In manic-depressives, a shift towards the manic phase may occur; should the patient enter a manic phase nortriptyline should be discontinued.
When nortriptyline is used for the depressive component of schizophrenia, psychotic symptoms may be aggravated. Nortriptyline should be used in combination with a neuroleptic.
In patients with the rare condition of shallow anterior chamber and narrow chamber angle attacks of acute glaucoma due to dilation of the pupil may be provoked.
Anaesthetics given during tri/tetracyclic antidepressant therapy may increase the risk of arrhythmias and hypotension. If possible, discontinue nortriptyline several days before surgery; if emergency surgery is unavoidable, the anaesthetist should be informed that the patient is being so treated.
As described for other psychotropics nortriptyline may modify insulin and glucose responses calling for adjustment of the antidiabetic therapy in diabetic patients; in addition the depressive illness itself may affect patients' glucose balance.
Hyperpyrexia has been reported with tricyclic antidepressants when administered with anticholinergic or with neuroleptic medications, especially in hot weather.
After prolonged administration, abrupt cessation of therapy may produce withdrawal symptoms such as headache, malaise, insomnia and irritability. These symptoms are not indicative of addiction.
Excipients: The tablets contain lactose monohydrate. Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicine.
Effects on ability to drive and use machines: Nortriptyline is not a particularly sedative drug.
However, patients who are prescribed psychotropic medication may be expected to have some impairment in general attention and concentration and should be cautioned about their ability to drive or operate machinery.
Use in Children: Nortrilen is not recommended for use in children and adolescents under the age of 18 due to lack of data on efficacy and safety. Treatment with Nortrilen is associated with a risk of cardiovascular adverse events in all age groups.
Pregnancy: Nortriptyline should not be administered during pregnancy unless the expected benefit to the patient outweighs the theoretical risk to the foetus.
Using high dosages of TCAs in the third trimester may result in effects, including neurobehavioral disturbances, in the newborn infant.
Lethargy has been reported in neonates with amitriptyline and urine retention with nortriptyline (metabolite of amitriptyline) administered to pregnant women until date of birth.
Lactation: As nortriptyline is found in breast milk in low concentrations it is not likely to affect the infant when therapeutic doses are used. The dose ingested by the infant is about 2% of the weight-related maternal daily dose (in mg/kg).
Breast-feeding can be continued during nortriptyline therapy if considered of clinical importance but observation of the infant is recommended, particularly in the first 4 weeks after giving birth.
Fertility: No data on the effect of nortriptyline on human and animal fertility is available.
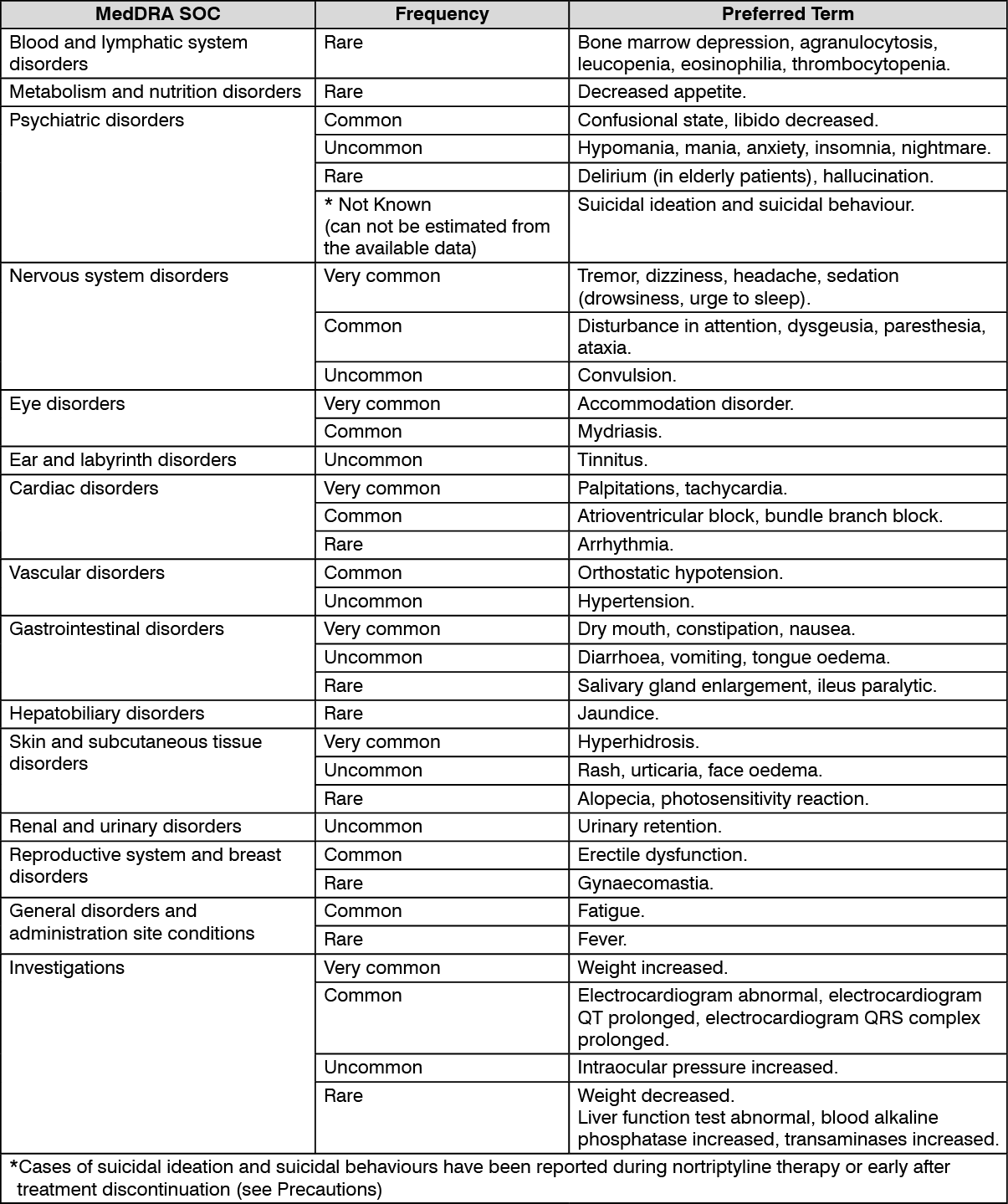
Nortriptyline may induce side effects similar to other cyclic antidepressants. Some of the following mentioned side effects e.g. headache, tremor, disturbance in attention, dry mouth, constipation and decreased libido may also be symptoms of depression and usually attenuate when the depressive state improves.
In the listing as follows the following convention is used: MedDRA system organ class / preferred term.
Very common (> 1/10); common (> 1/100, < 1/10); uncommon (> 1/1,000, < 1/100); rare (> 1/10,000, < 1/1,000); very rare (< 1/10,000), not known (can not be estimated from available data). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Epidemiological studies, mainly conducted in patients 50 years of age and older, show an increased risk of bone fractures in patients receiving SSRIs and TCAs. The mechanism leading to this risk is unknown.
Pharmacodynamic interactions: Contra-indicated combinations: MAOIs (non-selective as well as selective A (moclobemide) and B (selegiline)): risk of "serotonin syndrome" (see Contraindications).
Nortriptyline should not be given to patients receiving monoamine oxidase inhibitors (MAOIs). Treatment with nortriptyline may be instituted 14 days after discontinuation of irreversible non-selective MAOIs and minimum one day after discontinuation of the reversible moclobemide. Treatment with MAOIs may be introduced 14 days after discontinuation of nortriptyline.
Inadvisable combinations: Sympathomimetic agents: Nortriptyline may potentiate the cardiovascular effects of adrenaline, ephedrine, isoprenaline, noradrenaline, phenylephrine, and phenylpropanolamine (e.g. as contained in local and general anaesthetics and nasal decongestants).
Adrenergic neurone blockers: Tricyclic antidepressants may counteract the antihypertensive effects of guanethidine, betanidine, reserpine, clonidine and methyldopa. It is advisable to review all antihypertensive therapy during treatment with tricyclic antidepressants.
Anticholinergic agents: Tricyclic antidepressants may potentiate the effects of these drugs on the eye, central nervous system, bowel and bladder; concomitant use of these should be avoided due to an increased risk of paralytic ileus, hyperpyrexia, etc.
Drugs which prolong the QT-interval: Drugs which prolong the QT-interval, including antiarrhythmics such as quinidine, the antihistamines astemizole and terfenadine, some antipsychotics (notably pimozide and sertindole), cisapride, halofantrine, and sotalol, may increase the likelihood of ventricular arrhythmias when taken with tricyclic antidepressants.
Antifungals: Antifungals such as fluconazole and terbinafine increase serum concentrations of tricyclics and accompanying toxicity. Syncope and torsade de pointes have occurred.
Combinations requiring precautions for use: CNS depressants: Nortriptyline may enhance the sedative effects of alcohol, barbiturates and other CNS depressants.
Pharmacokinetic interactions: Influence of other medicinal products on the pharmacokinetics of tricyclic antidepressants: Tricyclic antidepressants including nortriptyline are metabolised by the hepatic cytochrome P450 isoenzyme CYP2D6. CYP2D6 is polymorphic in the population.
The CYP2D6 isozyme can be inhibited by a variety of psychotropic and other drugs, e.g. neuroleptics, serotonin reuptake inhibitors except citalopram (which is a very weak inhibitor), beta-blockers, and newer antiarrhythmics. These drugs may produce substantial decreases in tricyclic metabolism and marked increases in plasma concentrations.
Barbiturates and other enzyme inducers may lower plasma levels of tricyclic antidepressants and reduce antidepressant response.
Cimetidine, methylphenidate and calcium-channel blockers increase plasma levels of tricyclics and accompanying toxicity.
Tricyclic antidepressants and neuroleptics mutually inhibit the metabolism of each other; this may lead to a lowered convulsion threshold, and seizures. It may be necessary to adjust the dosage of these drugs.
Antifungals such as fluconazole and terbinafine have been observed to increase serum levels of amitriptyline and nortriptyline.
Nortriptyline plasma concentration can be increased by valproic acid. Clinical monitoring is therefore recommended.
Special precautions for disposal and other handling: Any unused product or waste material should be disposed of in accordance with local requirements.
Incompatibilities: Not applicable.
N06AA10 - nortriptyline ; Belongs to the class of non-selective monoamine reuptake inhibitors. Used in the management of depression.
Nortrilen tab 10 mg
100's
Nortrilen tab 25 mg
100's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out