Pharmacology: Mechanism of Action: Carvedilol is a cardiovascular agent for the treatment of congestive heart failure that combines beta-adrenoceptor blockade and vasodilation in a single racemic mixture. Nonselective beta-adrenoceptor blocking activity is present in the S(-) enantiomer and alpha
1-adrenoceptor blocking activity is present at equal potency in both the R(+) and S(-) enantiomers. Carvedilol has no intrinsic sympathomimetic activity. Its action on beta-receptors is 10 times stronger than on alpha
1-receptors.
Carvedilol reduces peripheral vascular resistance by vasodilation, thereby causing a fall in systemic blood pressure after acute administration, predominantly mediated through selective alpha
1-antagonism. Beta blockade prevents reflex tachycardia with the net result that heart rate is unchanged or decreased. Carvedilol reduces renin release through beta blockade.
The mechanism for the beneficial effects of carvedilol in congestive heart failure has not been established.
Detailed Pharmacology: Beta-adrenoceptor blocking activity has been demonstrated in animal and human studies by showing that carvedilol 1) reduces exercise- and/or isoproterenol-induced tachycardia, and 2) reduces reflex orthostatic tachycardia. Significant beta-adrenoceptor blocking effect is usually seen within 1 hour of oral drug administration (in the fasting state). Carvedilol is not cardioselective, does not have intrinsic sympathomimetic activity, and possesses some membrane stabilizing activity.
Alpha
1-adrenoceptor blocking activity has been demonstrated in animal and human studies by showing that carvedilol 1) attenuates the pressor effects of phenylephrine but not of angiotensin II, 2) causes vasodilation; and 3) reduces peripheral vascular resistance. The onset of these effects is usually seen within 30 minutes of oral drug administration (in the fasting state).
In animal
in vivo studies, and in human
in vitro studies, carvedilol has been shown to have antioxidant activity. Some metabolites are ten-fold more potent than carvedilol in this regard, although these metabolites are found at serum concentrations ten-fold lower than those of carvedilol. The carbazole portion of the molecule is responsible for this antioxidant activity, which is found to be equally potent in each enantiomer; the beta-blocking and vasodilating actions reside in other parts of the molecular structure and both enantiomers of carvedilol are equally potent as antioxidants. The clinical significance of the antioxidant effect has not been established.
Pharmacodynamics: In two studies that compared the acute hemodynamic effects of carvedilol to baseline measurements in patients with congestive heart failure, there were significant reductions in systemic blood pressure, pulmonary artery pressure, pulmonary capillary wedge pressure, and heart rate. Initial effects on cardiac output, stroke volume index and systemic vascular resistance were small and variable.
In terms of chronic hemodynamic effects (12 to 14 weeks), carvedilol significantly reduced systemic blood pressure, pulmonary artery pressure, right atrial pressure, systemic vascular resistance and heart rate while stroke volume index was increased.
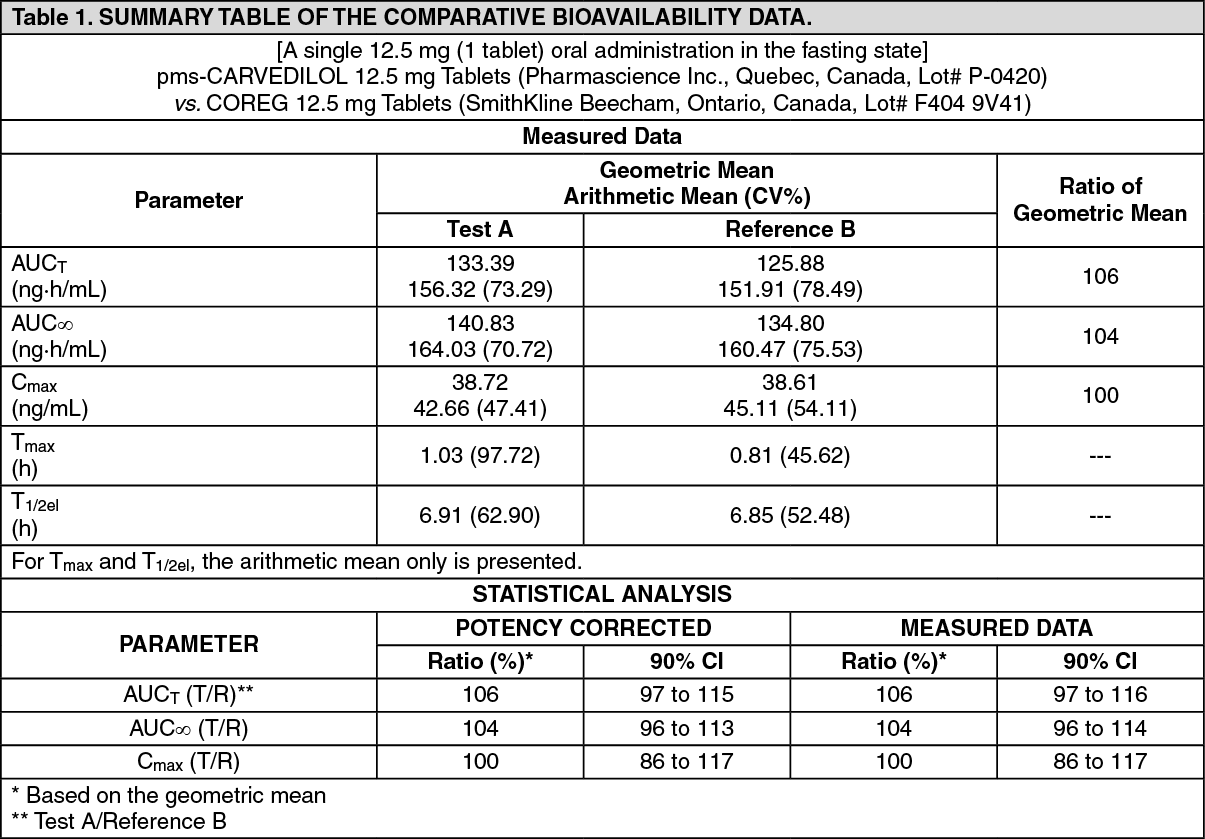
Clinical Trials: See Tables 1 & 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In a US multicentre program, 1197 patients with stable symptomatic congestive heart failure, NYHA class II to IV, were challenged with a low dose of carvedilol (3.125 or 6.25 mg twice daily) for 2 to 4 weeks to determine tolerability. Of these patients, 1094 were then randomized to double-blind treatment with carvedilol (n=696) or placebo (n=398) and stratified to one of four studies based on baseline exercise performance, with the prestated objective to evaluate total mortality. The average duration of therapy on carvedilol was 6.5 months in this program. Patients entering the program had symptomatic congestive heart failure due to ischemic or non-ischemic cardiomyopathy with an ejection fraction ≤ 35%. All patients received conventional therapy, i.e. diuretics, angiotensin-converting enzyme (ACE) inhibitors, if tolerated, with or without digoxin.
On an intent-to-treat basis, total mortality in this program was 3.2% in the carvedilol group and 7.8% in the placebo group. Thus, a relative risk reduction of 65% (95% confidence limits 39 and 80%, p=0.001) was observed. Treatment with carvedilol was associated with a significant decrease in the relative risk of death from progressive pump failure (81%, p=0.001) and the relative risk of sudden death (56%, p=0.033). The incidence of cardiovascular hospitalizations was 13% in the carvedilol group and 21% in the placebo group, with a relative risk reduction of 36% (95% confidence limits 14% and 53%, p=0.004).
Improved patient well-being was observed with carvedilol treatment in the US multicentre program, as indicated by a change in the NYHA class from baseline to endpoint for the four US phase III placebo-controlled studies. The overall between-group difference in distributions, stratified by protocol and baseline classification, was significant (p<0.001) and as also indicated by patient and physician global assessments during US Phase III trials, 78% of patients in the carvedilol group rated their condition as improved compared to 63% in the placebo group (p values over four studies from 0.001 to 0.032). However, exercise tolerance was not improved.
In a large multicenter trial of carvedilol, performed in Australia and New Zealand, 443 patients with stable symptomatic congestive heart failure NYHA Class I to III, were challenged with a low dose of carvedilol (3.125 mg or 6.25 mg twice daily) for 2 to 4 weeks to determine tolerability. Of these patients, 415 were then randomized to double-blind treatment with carvedilol (n=207) or placebo (n=208). The average duration of therapy on carvedilol was 16.1 months in this study. Patients entering the program had symptomatic congestive heart failure due to ischemic cardiomyopathy with an ejection fraction ≤ 45%. All patients received conventional therapy, i.e. diuretics, (ACE) inhibitors, if tolerated, with or without digoxin.
On an intent-to-treat basis, total mortality in this Australia and New Zealand trial was 10.1% in the carvedilol group and 13.9% in the placebo group, a non-statistically significant relative risk reduction of 29% (confidence limits -24% and 59%, p=0.231). Cardiovascular hospitalizations were 31% in the carvedilol group and 40% in the placebo group, a relative risk reduction of 28% (95% confidence limits: 1% and 48%, p=0.044). Patient well-being, as judged by NYHA class or Specific Activity Scale rating, as well as exercise tolerances were no different in the carvedilol group compared to the placebo group.
In the COPERNICUS trial, 2289 patients with severe heart failure were randomly assigned to treatment with placebo or carvedilol for up to 29 months. Patients had symptoms at rest or on minimal exertion and had a left ventricular ejection fraction < 25% (mean 20%), despite treatment with diuretics (99%), an ACE inhibitor (89%), and digitalis (66% worldwide, 85% within Canada) for more than 2 months. Patients with cardiac impairment not related to left ventricular dysfunction were excluded as were patients with prior cardiac transplant, cardioplasty, unstable angina, myocardial infarction, destabilizing cardiac arrhythmias, or treatment within 1 month with an α-adrenoceptor antagonist (except for prostatism), a calcium channel blocker or a class I antiarrhythmic agent. The trial was followed by a data safety monitoring committee, which stopped the trial early after a median follow-up of 10.4 months because of an observed reduction in total mortality, the primary endpoint, from 19.7% per patient-year on placebo to 12.8% per patient-year on carvedilol, (a relative risk reduction of 35%; hazard ratio 0.65, 95% CI 0.52 and 0.81, and a P value adjusted for interim analyses of 0.0014). The results are summarized in Table 3 and the figure. (See Table 3 and figure.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics: See Table 4.
Click on icon to see table/diagram/image
Absorption: Carvedilol is rapidly absorbed following oral administration, with peak plasma concentrations of carvedilol observed at 1 hour post-dose in fasting subjects. Despite being well-absorbed, absolute bioavailability is approximately 25% to 35% due to a significant degree of first-pass metabolism.
Plasma concentrations achieved are proportional to the oral dose administered. When administered with food, the rate of absorption is slowed, as evidenced by a delay in time to reach peak plasma concentrations (about 2.3 hours post-dose), with no significant difference in extent of bioavailability.
Distribution: Carvedilol is highly bound to plasma proteins, (greater than 98%) primarily to albumin. The plasma-protein binding is independent of concentration over the therapeutic range. Carvedilol is a basic, lipophilic compound with a steady-state volume of distribution of approximately 115 L.
Metabolism: Following oral administration, the apparent mean terminal elimination half-life of carvedilol ranges from 7 to 10 hours. Plasma clearance ranges from 500 to 700 mL/min. Carvedilol is extensively metabolized with less than 2% of the dose excreted unchanged in the urine. Carvedilol is metabolized mainly by glucuronidation and aromatic ring oxidation by the cytochrome P450 system (primarily CYP2D6 and CYP2C9 isozymes). The metabolites of carvedilol are excreted mainly via the bile into the feces.
Excretion: Elimination is mainly biliary. The primary route of excretion is via the feces.
A minor part is eliminated via the kidneys in the form of various metabolites.
Carvedilol undergoes stereoselective first-pass metabolism with plasma levels of R(+)-carvedilol approximately 2- to 3-fold higher than S(-)-carvedilol following oral administration in healthy subjects. The mean apparent terminal elimination half-life for R(+)-carvedilol ranges from 5 to 9 hours compared with 7 to 11 hours for the S(-) enantiomer.
There are at least 5 pharmacologically active metabolites of carvedilol: desmethyl, 4'-hydroxyphenyl, 5'-hydroxyphenyl, 1-hydroxycarbazolyl and 8-hydroxycarbazolyl metabolites. Each of these metabolites has two enantiomeric forms and each metabolite possesses different relative potencies with regard to α- and β-receptor blocking activities. Plasma concentrations of these metabolites are 10- to 50-fold lower than those observed for the parent compound. Therefore, even for metabolites that are more active or at least as active as carvedilol itself, they are present at such low concentrations that they would produce effects less than, or at least not greater than, the parent compound.
Special Populations and Conditions: Geriatrics: Compared to young subjects (18 to 43 years old), AUC values for carvedilol were, on average, 38% higher in elderly (65 to 76 years old) subjects. Moreover, AUC values were 50% higher for S(-)-carvedilol and 23% for R(+)-carvedilol in the elderly compared to the young subjects. Changes in C
max values for carvedilol and its enantiomers were less pronounced, approximately 8% to 17% higher in elderly subjects with no apparent change in T
max. Although the terminal elimination half-lives of carvedilol were similar in both young and elderly subjects, the initial decline in plasma concentrations in the elderly appeared to be slower than in the young subjects suggesting a decrease in systemic clearance of carvedilol in the elderly (see Precautions and Dosage & Administration).
Hepatic Insufficiency: In patients with cirrhotic liver disease, the absolute bioavailability of carvedilol was 4 times greater as compared to healthy subjects with median C
max and AUC values for carvedilol 4 to 7 times higher in patients with liver disease following oral administration (see Contraindications and Precautions).
Renal Insufficiency: Although carvedilol is metabolized primarily by the liver, plasma concentrations of carvedilol have been reported to be increased in patients with renal impairment. Based on AUC data, approximately 40% to 50% higher plasma concentrations of carvedilol were observed in hypertensive patients with moderate to severe renal impairment compared to a control group of hypertensive patients with normal renal function. However, the ranges of AUC values were similar for both groups. Changes in C
max data were less pronounced, approximately 12% to 26% higher in patients with impaired renal function.
The pharmacokinetics of carvedilol are not altered by hemodialysis.
Patients with Congestive Heart Failure: Steady-state plasma concentrations of carvedilol and its enantiomers increased proportionally over the 6.25 to 50 mg b.i.d. dose range in patients with congestive heart failure. Compared to healthy subjects, patients with Class IV congestive heart failure had increased mean AUC and C
max values for carvedilol and its enantiomers with up to 50% to 100% higher values than normal volunteers. The mean apparent terminal elimination half-life for carvedilol was similar to that observed in healthy subjects.
Genetic Polymorphism: Carvedilol is subject to genetic polymorphism with poor metabolizers of debrisoquin (deficient in CYP2D6) exhibiting 2- to 3-fold higher plasma concentrations of the R(+)-carvedilol compared to extensive metabolizers. In contrast, plasma levels of S(-)-carvedilol are increased only about 20% to 25% in poor metabolizers, indicating that the metabolism of this enantiomer is affected to a lesser extent by CYP2D6 than R(+)-carvedilol. The pharmacokinetics of carvedilol enantiomers do not appear to be different in poor metabolizers of S-mephenytoin, i.e., deficient in CYP2C19.
Toxicology: LD
50 values in mg/kg after 14 days observation time (n=10 for all groups): See Table 5.
Click on icon to see table/diagram/image
Almost all deaths occurred one to two days after dosing. No systemic clinical signs were observed in the animals treated orally. Animals dosed parenterally (except doses intraperitoneally) showed transient apathy and ptosis.
Long-Term Toxicity: Carvedilol was administered daily for 12 months to 5 dogs/sex/group at 0, 10, 30, 100, and 300 mg/kg given orally in two divided doses. Carvedilol was also administered daily in the food for 12 months to 30 rats/sex/group at doses of 30, 100, or 300 mg/kg and in another study for 18 months to 30 rats/sex/group at doses of 10, 31, 89, 261 mg/kg. Following oral administration, no toxic effects were seen at 10 mg/kg in the dog and at 30 mg/kg in the rat. These no-effect doses are 14 and 42 times higher than a relatively high therapeutic dose in humans (based on a daily dose of 50 mg in a 70 kg patient).
Teratology Studies: Teratology studies show no evidence of carvedilol having teratogenic effects. In the fertility study, high doses resulted in reduced fertility and diminished general reproductive capacity in the F
0 generation and retardation in physical development in the F
1 generation. These adverse effects are regarded as nonspecific effects due to loading the parental generation with toxic dosages.
Mutagenicity Studies: No mutagenic potential of carvedilol was demonstrated in several
in vitro and
in vivo test systems.
Carcinogenicity Studies: Two-year carcinogenicity studies were conducted in both mice and rats. In the mouse study, groups of 50 mice/sex/group received daily doses of 20, 65 or 200 mg/kg in the diet. A group of 100 mice/sex/group were untreated and served as controls. In the rat study, groups of 50 rats/sex/group received 0, 200, 400, 800, or 1600 ppm carvedilol in the diet. These concentrations corresponded to daily dosages at the start of the study up to 21.7, 43, 86.7 and 169.5 mg/kg. Since the carvedilol dietary concentration did not change throughout the study and the animals gained weight, by the end of the study the actual daily dosages decreased to 9.5, 18.8, 38.1 and 74.7 mg/kg.
The results of the histopathologic examinations from these carcinogenicity studies indicated that carvedilol does not have either a tumorigenic or a carcinogenic potential.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image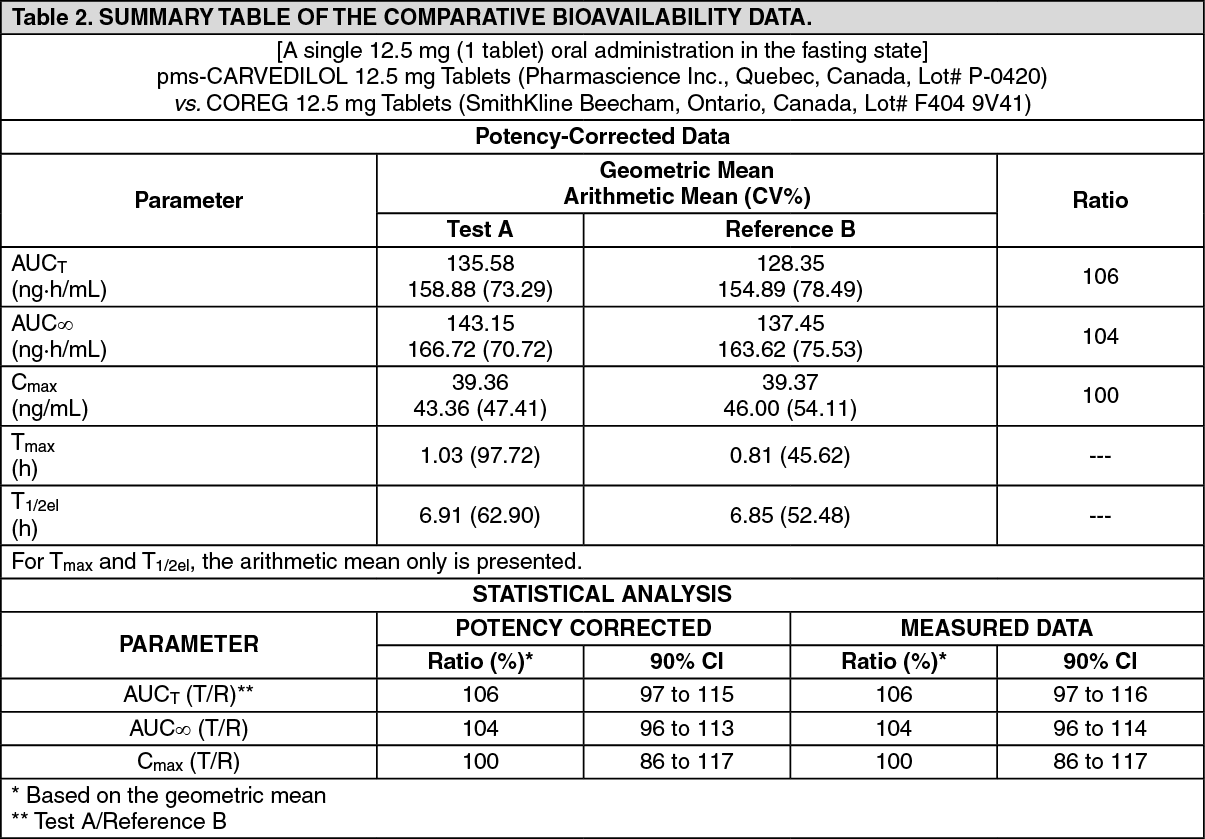 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image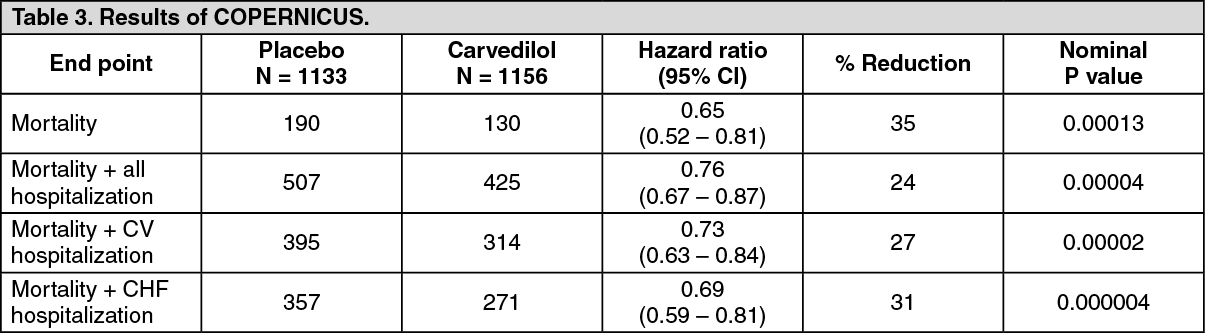 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image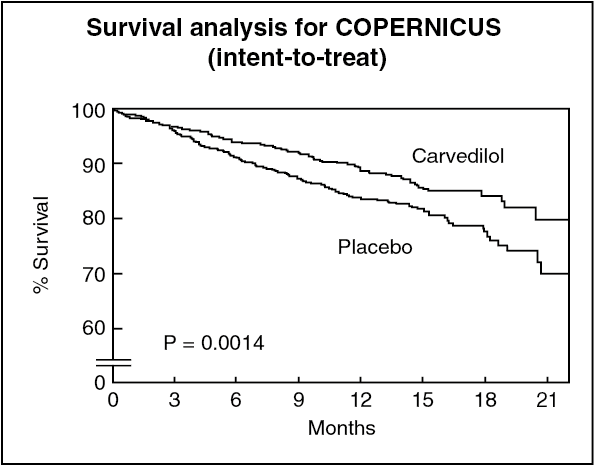 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image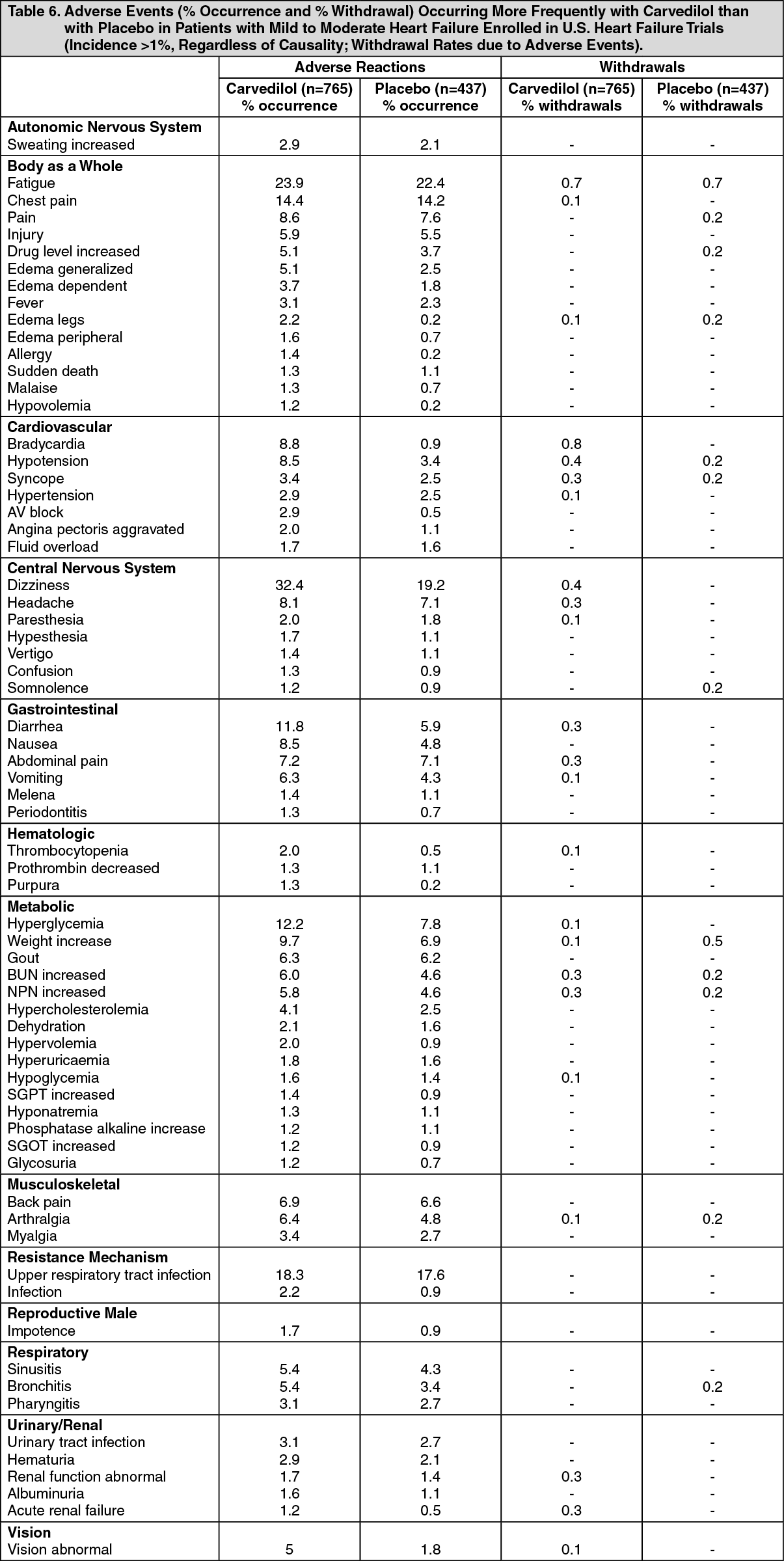 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image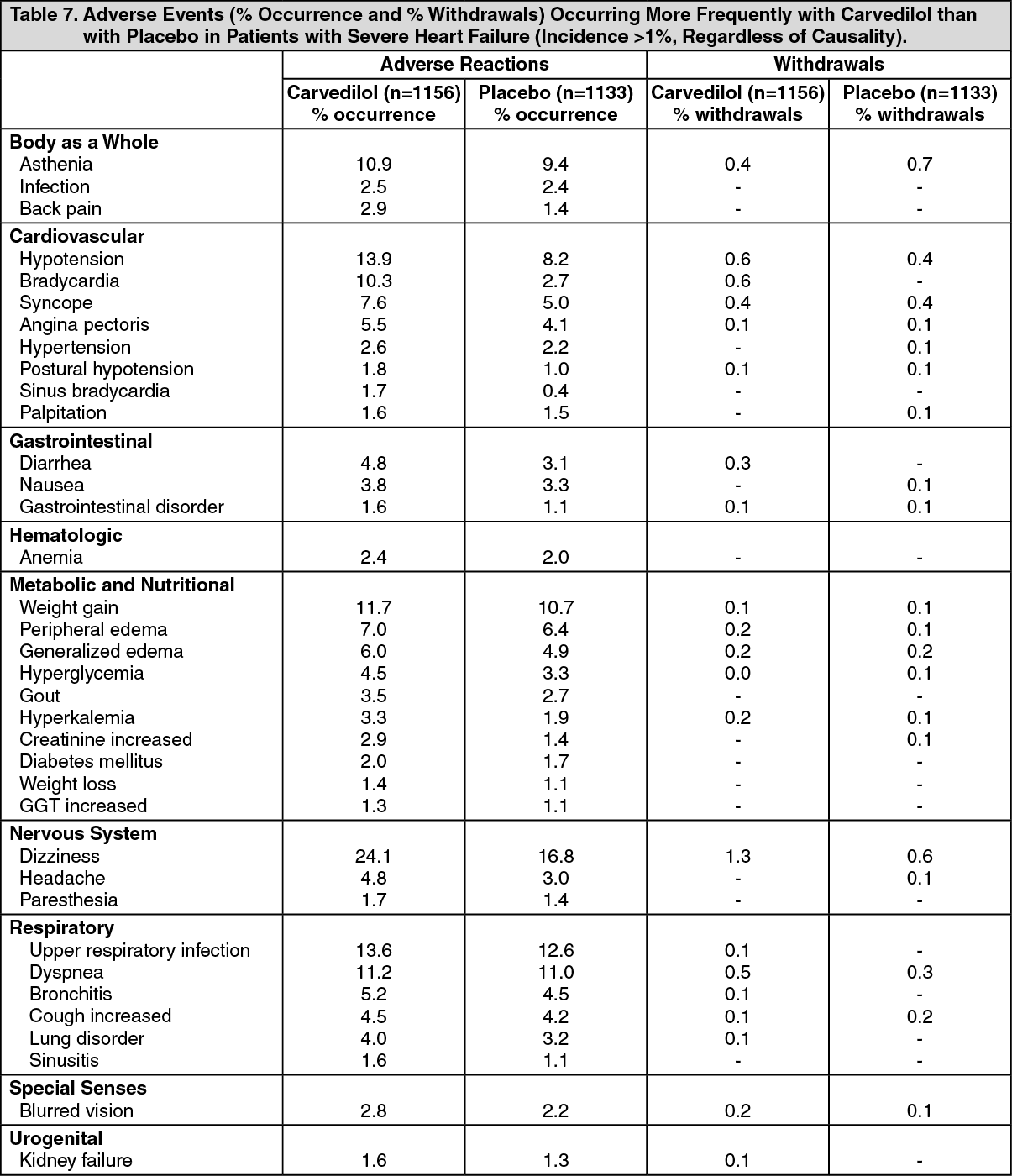 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image




 Sign Out
Sign Out
