The stated frequencies of adverse events represent the proportion of individuals who experienced, at least once, a treatment-emergent adverse event of the type listed. An event was considered treatment-emergent if it occurred for the first time or worsened while receiving therapy following baseline evaluation.
Overview of Clinical Trial and Post-Market Adverse Drug Reactions: The most commonly reported adverse drug reactions in both clinical trials and during post-marketing experience with quetiapine (≥ 10%) are somnolence dizziness, dry mouth, withdrawal (discontinuation) symptoms, elevations in serum triglyceride levels, elevations in total cholesterol (predominantly LDL cholesterol), decreases in HDL cholesterol, weight gain, decreased hemoglobin and extrapyramidal symptoms.
Clinical Trial Adverse Drug Reactions: The prescriber should be aware that the figures in the tables and tabulations cannot be used to predict the incidence of side effects in the course of usual medical practice where patient characteristics and other factors differ from those that prevailed in the clinical trials. Similarly, the cited frequencies cannot be compared with figures obtained from other clinical investigations involving different treatments, uses, and investigators. The figures cited, however, do provide the prescribing physician with some basis for estimating the relative contribution of drug and nondrug factors to the side effect incidence in the populations studied.
Adverse Events Associated with Discontinuation: Short-Term Placebo-Controlled Clinical Trials: Schizophrenia: Overall, 3.9% of quetiapine fumarate immediate-release treated patients (n = 510) discontinued treatment due to adverse events compared with 2.9% of placebo-treated patients (n = 206). Somnolence, the single most common adverse event leading to withdrawal from quetiapine treatment, led to the withdrawal of four quetiapine-treated patients and no placebo-treated patients. Postural hypotension, hypotension, and/or tachycardia led to withdrawal of 1.8% of quetiapine-treated subjects, compared to 0.5% of placebo-treated subjects.
Bipolar Disorder: Bipolar Mania: Discontinuations due to adverse events were similar for quetiapine fumarate (5.7%) and placebo (5.1%).
Bipolar Depression: Discontinuations due to adverse events were 13.1% for quetiapine fumarate and 6.3% for placebo. Sedation, somnolence and dizziness were the most common adverse events leading to discontinuation in the quetiapine fumarate treatment groups.
Combined Short- and Long-Term Controlled Trial Database in Schizophrenia: In a premarketing controlled clinical trial database of 1,710 quetiapine fumarate-treated patients, 5% discontinued due to an adverse event. Somnolence was the single most common adverse event leading to withdrawal of 24 patients from quetiapine fumarate, and was the only adverse event leading to withdrawal that occurred in more than 1% of patients. Cardiovascular adverse events (e.g., postural hypotension, hypotension, tachycardia, dizziness) accounted for 20% of all subject withdrawals from quetiapine treatment. Sixteen (0.9%) quetiapine-treated subjects were withdrawn due to elevated liver enzymes. Four quetiapine-treated subjects were withdrawn because of leucopenia. Two of these subjects had at least one clinically significant, non-baseline low neutrophil count. Two quetiapine-treated subjects were withdrawn from the trial because of suspected neuroleptic malignant syndrome (NMS).
Commonly Observed Adverse Events in Short-Term Placebo-Controlled Clinical Trials: Schizophrenia: The following treatment-emergent adverse events, derived from Table 8, commonly occurred during acute therapy with quetiapine fumarate (incidence of at least 5%, and an incidence at least 5% higher than that observed with placebo): somnolence, dizziness, dry mouth, postural hypotension, and elevated ALT levels.
Bipolar Disorder: Bipolar Mania: In the bipolar mania studies, the following treatment-emergent adverse events commonly occurred during acute therapy with quetiapine fumarate (incidence of at least 5%, and an incidence at least 5% higher than that observed with placebo): somnolence, dry mouth, and weight gain.
Bipolar Depression: In the bipolar depression studies, the following treatment-emergent adverse events commonly occurred during acute therapy with quetiapine fumarate (incidence of at least 5%, and an incidence at least 5% higher than that observed with placebo): dry mouth, somnolence, sedation, dizziness and constipation.
Incidence of Adverse Events in Placebo-Controlled Clinical Trials: Certain portions of the following discussion relating to objective or numeric safety parameters are derived from studies in patients with schizophrenia and have not been duplicated for bipolar mania trials. However, this information is also generally applicable to bipolar mania. Table 8 enumerates the incidence, rounded to the nearest percent, of treatment-emergent adverse events that occurred during acute therapy (up to 6 weeks) of schizophrenia in 1% or more of patients treated with quetiapine fumarate (doses of 150 mg/day or more) where the incidence in patients treated with quetiapine fumarate was greater than the incidence in placebo-treated patients. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Table 9 enumerates the incidence, rounded to the nearest percent, of treatment-emergent adverse events that occurred during acute therapy (8 weeks) of bipolar depression in ≥ 1% of patients treated with quetiapine fumarate (doses of 300 or 600 mg/day) where the incidence in patients treated with quetiapine fumarate was greater than the incidence in placebo-treated patients. (See Table 9.)
Click on icon to see table/diagram/image
Other Adverse Events: Frequencies are reported as follows: Very common (≥ 10%); Common (≥ 1% - < 10%); Uncommon (≥ 0.1% - < 1%); Rare (≥ 0.01% - < 0.1%).
Weight Gain: During acute therapy (up to 6 weeks) in placebo-controlled schizophrenia clinical trials, mean weight gain in patients taking quetiapine fumarate was 2.3 kilograms compared to a mean weight gain of 0.1 kilograms in patients taking placebo. In open-label extension trials with quetiapine fumarate monotherapy, mean weight gain after 9 to 13 weeks was 1.58 kg, after 14 to 26 weeks, 0.26 kg, after 27 to 39 weeks, 1.66 kg, after 40 to 52 weeks, -1.53 kg and after 53 to 78 weeks, 1.98 kg (see Endocrine and Metabolism: Weight Gain under Precautions). In the acute placebo-controlled bipolar mania clinical trials (up to 12 weeks), mean weight gain in patients taking quetiapine fumarate was 1.8 kg compared to a mean weight loss of 0.1 kg in patients taking placebo. In patients completing the entire 12 weeks of treatment mean weight gain in patients taking quetiapine fumarate was 2.8 kg.
In the acute placebo-controlled bipolar depression clinical trials (8 weeks) mean weight gain in patients taking quetiapine fumarate was 1.15 kg compared to a mean weight gain of 0.1 kg in patients taking placebo. During maintenance treatment, patients treated with quetiapine fumarate 300 mg or placebo lost on average 0.1 kg and 0.6 kg, respectively, while patients treated with quetiapine 600 mg gained on average 0.8 kg. In patients who completed 40 and 54 weeks of maintenance treatment a small mean decrease was seen in the quetiapine fumarate 300 mg group (-0.2 kg) and placebo group (-0.8 kg) while patients in the quetiapine fumarate 600 mg group showed a mean weight gain of 1.2 kg (see Endocrine and Metabolism: Weight Gain under Precautions).
Based on the cumulative acute placebo-controlled clinical trial database, weight gain (based on ≥ 7% increase in body weight from baseline) was reported in 9.6% in quetiapine-treated patients and 3.8% in placebo-treated patients, which occurs predominantly during the early weeks of treatment in adults (see Endocrine and Metabolism: Weight Gain under Precautions).
Seizures: There have been uncommon reports of seizures in patients administered quetiapine, although the frequency was no greater than that observed in patients administered placebo in controlled clinical trials (see Neurologic: Seizures under Precautions).
Restless Legs Syndrome: There have been uncommon cases of restless legs syndrome in patients administered quetiapine.
Priapism: There have been rare reports of priapism in patients administered quetiapine.
Somnolence: Somnolence may occur, usually during the first two weeks of treatment, which generally resolves with the continued administration of quetiapine.
Somnambulism: In rare cases, somnambulism and other related events, such as sleep-related eating disorders, have been reported.
Neuroleptic Malignant Syndrome: As with other antipsychotics, rare cases of neuroleptic malignant syndrome have been reported in patients treated with quetiapine (see Neurologic: Neuroleptic Malignant Syndrome (NMS) under Precautions).
Hypothermia: There have been rare cases of hypothermia in patients treated with quetiapine.
Vital Signs: As with other antipsychotics with α
1 adrenergic blocking activity, quetiapine may induce postural hypotension, associated with very common cases of dizziness, common cases of tachycardia and, in uncommon cases, some patients may experience syncope especially during the initial dose titration period (see Cardiovascular: Hypotension and Syncope under Precautions). In placebo-controlled clinical trials in schizophrenia, postural hypotension was reported with an incidence of 8% in quetiapine fumarate-treated patients compared to 2% in placebo-treated patients. Quetiapine fumarate was associated with a mean baseline to endpoint increase in heart rate of 3.9 beats per minute, compared to 1.6 beats per minute among placebo-treated patients.
Bradycardia: Uncommon cases of bradycardia and related events have been reported in patients treated with quetiapine. It may occur at or near initiation of treatment and be associated with hypotension and/or syncope.
Pancreatitis: Rare cases of pancreatitis have been reported from a review of all clinical trials with quetiapine.
Dyspnea: Common cases of dyspnea often occurred in the setting of tachycardia, dizziness, orthostatic hypotension and/or underlying cardiac/respiratory disease.
Palpitations: Common cases of palpitations have occurred in the setting of tachycardia, dizziness, orthostatic hypotension and/or underlying cardiac/respiratory disease.
Peripheral Edema: As with other antipsychotic agents, common cases of peripheral edema have been reported in patients treated with quetiapine.
Pyrexia: There have been common cases of pyrexia in patients treated with quetiapine.
Vomiting: There have been common cases of vomiting in patients treated with quetiapine although this has been seen more often in elderly patients (> 65 years of age).
Mild Asthenia: As with other antipsychotic agents, common cases of mild asthenia have been reported in patients treated with quetiapine.
Rhinitis: Uncommon cases of rhinitis have been reported.
Hypersensitivity: Uncommon cases of hypersensitivity including angioedema have been reported.
ECG Changes: Between group comparisons for pooled placebo-controlled trials revealed no statistically significant quetiapine fumarate/placebo differences in the proportions of patients experiencing potentially important changes in ECG parameters, including QT, QTc, and PR intervals. However, the proportions of patients meeting the criteria for tachycardia were compared in four 3- to 6-week-placebo-controlled clinical trials for the treatment of schizophrenia revealing a 1% (4/399) incidence for quetiapine fumarate compared to 0.6% (1/156) incidence for placebo. Quetiapine fumarate use was associated with a mean increase in heart rate, assessed by ECG, of 7 beats per minute compared to a mean increase of 1 beat per minute among placebo patients. This slight tendency to tachycardia may be related to the potential of quetiapine for inducing orthostatic changes (see Cardiovascular: Hypotension and Syncope under Precautions). In bipolar mania trials, the proportion of patients meeting the criteria for tachycardia was 0.5% (1/192) for quetiapine fumarate compared to 0% (0/178) for placebo. In bipolar depression trials, the proportion of patients meeting the criteria for tachycardia in the acute phase was 0.06% (1/1,704) for quetiapine fumarate compared to 0% (0/598) for placebo. During maintenance treatment, the proportion was 0.4% (1/278) compared to 0.4% (1/284) for placebo.
Tardive Dyskinesia: There have been uncommon cases of tardive dyskinesia reported in patients administered quetiapine (see Neurologic: Tardive Dyskinesia (TD) and Extrapyramidal Symptoms (EPS) under Precautions).
Extrapyramidal Symptoms (EPS): There have been very common cases of EPS reported. Table 10 enumerates the percentage of patients with treatment-emergent extrapyramidal symptoms in a short-term acute phase clinical trial in patients with schizophrenia comparing five fixed doses of quetiapine fumarate with placebo (n = ~ 50 patients per group), as assessed by: 1) spontaneous complaints of parkinsonism (extrapyramidal syndrome, hypertonia, tremor and cogwheel rigidity), or akathisia; 2) Simpson-Angus scores (mean change from baseline); and 3) use of anticholinergic medication to treat emergent EPS. (See Table 10.)
Click on icon to see table/diagram/image
There were no differences between the quetiapine fumarate and placebo treatment groups in the incidence of EPS or concomitant use of anticholinergics and no evidence of dose-related increase in EPS or in the use of concomitant anticholinergics across the dose range of 75 - 750 mg/day. In 2 bipolar mania placebo-controlled clinical trials using variable doses of quetiapine fumarate, there were no differences between the quetiapine fumarate and placebo treatment groups in the incidence of EPS, as assessed by Simpson-Angus total scores and Barnes Akathisia rating scale, spontaneous complaints of EPS and the use of concomitant anticholinergic medications to treat EPS.
In short-term placebo-controlled clinical trials in schizophrenia and bipolar mania, the aggregated incidence of EPS-related adverse events was similar to placebo (schizophrenia: 7.8% for quetiapine and 8.0% for placebo; bipolar mania: 11.2% for quetiapine and 11.4% for placebo). In short-term placebo-controlled clinical trials in bipolar depression, the aggregated incidence of EPS-related adverse events was 8.9% for quetiapine compared to 3.8% for placebo. The incidence of individual EPS-related adverse events (e.g., akathisia, extrapyramidal disorder, tremor, dyskinesia, dystonia, restlessness, muscle contractions involuntary, psychomotor hyperactivity and muscle rigidity), however was generally low and did not exceed 4% for any individual adverse event. In long-term studies of schizophrenia and bipolar disorder the aggregated exposure adjusted incidence of treatment-emergent EPS was similar between quetiapine and placebo (see Neurologic: Tardive Dyskinesia (TD) and Extrapyramidal Symptoms (EPS) under Precautions).
Blurred Vision: There have been common cases of blurred vision in patients administered quetiapine.
Dysphagia: There have been uncommon cases of dysphagia in patients administered quetiapine. In clinical trials an increase in the rate of dysphagia with quetiapine versus placebo was only observed in bipolar depression (see Gastrointestinal: Dysphagia and Aspiration Pneumonia; and Use in Elderly: Use in Geriatric Patients with Dementia: Dysphagia under Precautions).
Dysarthria: There have been common cases of dysarthria in patients administered quetiapine.
Acute Withdrawal (discontinuation) Symptoms: Acute discontinuation symptoms such as insomnia, nausea, headache, diarrhea, vomiting, dizziness and irritability, have been described after abrupt cessation of antipsychotic drugs including quetiapine fumarate. Gradual withdrawal over a period of at least one to two weeks is advisable. Symptoms usually resolved after 1-week post-discontinuation (see General: Acute Withdrawal (discontinuation) Symptoms under Precautions).
Abnormal Dreams and Nightmares: There have been common cases of abnormal dreams and nightmares in patients administered quetiapine.
Suicide-related Events: In short-term placebo-controlled clinical trials across all indications and ages, the incidence of suicide-related events (suicidal thoughts, self-harm and suicide) was 0.8% for both quetiapine (76/9,327) and for placebo (37/4,845).
In these trials of patients with schizophrenia, the incidence of suicide-related events was 1.4% (3/212) for quetiapine and 1.6% (1/62) for placebo in patients 18-24 years of age, 0.8% (13/1,663) for quetiapine and 1.1% (5/463) for placebo in patients ≥ 25 years of age.
In these trials of patients with bipolar mania the incidence of suicide-related events was 0% for both quetiapine (0/60) and placebo (0/58) in patients 18-24 years of age, 1.2% for both quetiapine (6/496) and placebo (6/503) in patients ≥ 25 years of age.
In these trials of patients with bipolar depression the incidence of suicide-related events was 3.0% (7/233) for quetiapine and 0% (0/120) for placebo in patients 18-24 and 1.2% for both quetiapine (19/1,616) and placebo (11/622) in patients ≥ 25 years of age (see Psychiatric: Suicide/Suicidal Thoughts or Clinical Worsening under Precautions).
Irritability: There have been common cases of irritability in patients administered quetiapine.
Increased Appetite: There have been common cases of increased appetite in patients administered quetiapine.
Constipation: Patients should be advised of the risk of severe constipation during quetiapine fumarate treatment, and that they should tell their doctor if constipation occurs or worsens, as they may need laxatives.
Urinary Retention: There have been uncommon cases of urinary retention in patients administered quetiapine.
Agranulocytosis: There have been rare cases of agranulocytosis based on the frequency of patients during all quetiapine clinical trials with severe neutropenia (< 0.5 x 10
9/L) and infection.
Abnormal Hematologic and Clinical Chemistry Findings: As with other antipsychotics, common cases of leucopenia and/or neutropenia have been observed in patients administered quetiapine. In clinical trial and post-marketing experience, events of severe neutropenia (< 0.5 x 10
9/L), granulocytopenia and agranulocytosis (severe neutropenia and infection) have been reported during antipsychotic use, including quetiapine (see Pharmacology under Actions). Leucopenia cases were based on shifts from normal baseline to potentially clinically important values at any time post-baseline in all trials. Shifts in white blood cells were defined as ≤ 3 x 10
9 cells/L at any time (see Hematologic: Leukopenia, Neutropenia and Agranulocytosis under Precautions). Based on shifts (eosinophil shifts were defined as ≥ 1 x 10
9 cells/L at any time) from normal baseline to potentially clinically important values at any time post-baseline in all trials, common cases of increased eosinophils have been observed. Uncommon cases of thrombocytopenia (platelet count decreased, ≤ 100 x 10
9/L on at least one occasion) have been observed.
Decreased hemoglobin to ≤ 130 g/L males, ≤ 120 g/L females on at least one occasion occurred in 11% of quetiapine patients in all trials including open-label extensions. In short-term placebo-controlled trials, decreased hemoglobin to ≤ 130 g/L males, ≤ 120 g/L females on at least one occasion occurred in 8.3% of quetiapine patients compared to 6.2% of placebo patients.
Based on clinical trial adverse event reports not associated with neuroleptic malignant syndrome, rare cases of elevations in blood creatine phosphokinase have been reported in patients administered quetiapine.
Hyperprolactinemia: Common cases of elevations in serum prolactin levels have been observed (> 20 mcg/L in males and > 30 mcg/L in females) (see Endocrine and Metabolism: Hyperprolactinemia under Precautions).
Neutropenia: In all short-term placebo-controlled monotherapy clinical trials among patients with a baseline neutrophil count ≥ 1.5 x 10
9/L, the incidence of at least one occurrence of neutrophil count < 1.5 x 10
9/L was 1.9% in patients treated with quetiapine, compared to 1.5% in placebo-treated patients. The incidence ≥ 0.5 - < 1.0 x 10
9/L was 0.2% in patients treated with quetiapine and 0.2% in placebo-treated patients. In clinical trials conducted prior to a protocol amendment for discontinuation of patients with treatment-emergent neutrophil count < 1.0 x 10
9/L, among patients with a baseline neutrophil count ≥ 1.5 x 10
9/L, the incidence of at least one occurrence of neutrophil count < 0.5 x 10
9/L was 0.21% in patients treated with quetiapine and 0% in placebo-treated patients (see Hematologic: Leukopenia, Neutropenia and Agranulocytosis under Precautions).
Transaminase Elevations: Common cases of asymptomatic elevations (shift from normal to > 3 times the upper limits of normal at any time) in serum alanine aminotransferase (ALT) or gamma-GT levels have been observed in some patients administered quetiapine. Uncommon cases of asymptomatic elevations (shift from normal to > 3 times the upper limits of normal at any time) in serum aspartate aminotranferase (AST) have been observed in some patients administered quetiapine. These elevations were usually reversible on continued quetiapine treatment (see Hepatic/Pancreatic: Transaminase Elevations under Precautions).
Thyroid: Quetiapine treatment was associated with dose-related decreases in thyroid hormone levels. Based on shifts (total T
4, free T
4, total T
3 and free T
3 < 0.8 x LLN (pmol/L) and TSH > 5mIU/L at any time) from normal baseline to a potentially clinically important value at any time post-baseline in all trials, uncommon cases of decreases in free T
3 and common cases of decreases in total T
4, free T
4 and total T
3, as well as increases in TSH have been reported. The following table shows the incidence of these shifts in short-term placebo-controlled clinical trials: See Table 11.
Click on icon to see table/diagram/image
In short-term placebo-controlled monotherapy trials, the incidence of reciprocal, potentially clinically significant shifts in T
3 and TSH was 0.0% for both quetiapine and placebo and 0.1% for quetiapine versus 0.0% for placebo for shifts in T
4 and TSH. These changes in thyroid hormone levels are generally not associated with clinically symptomatic hypothyroidism. The reduction in total and free T
4 was maximal within the first 6 weeks of quetiapine treatment, with no further reduction during long-term treatment. There was no evidence of clinically significant changes in TSH concentration over time. In nearly all cases, cessation of quetiapine treatment was associated with a reversal of the effects on total and free T
4, irrespective of the duration of treatment. In 8 patients, where TBG was measured, levels of TBG were unchanged (see Endocrine and Metabolism: Hypothyroidism under Precautions).
Hyperglycemia: Blood glucose increases to hyperglycemic levels (fasting blood glucose ≥ 7.0 mmol/L or a non-fasting blood glucose ≥ 11.1 mmol/L on at least one occasion) have been observed commonly (≥ 1% - < 10%) with quetiapine in clinical trials (see Endocrine and Metabolism: Hyperglycemia under Precautions).
In 2 long-term bipolar maintenance placebo-controlled adjunct clinical trials, mean exposure 213 days for quetiapine fumarate (646 patients) and 152 days for placebo (680 patients), the exposure-adjusted rate of any increased blood glucose level (≥ 7.0 mmol/L) for patients more than 8 hours since a meal was 18.0 per 100 patient years for quetiapine fumarate (10.7% of patients) and 9.5 for placebo per 100 patient years (4.6% of patients).
In short-term (12 weeks duration or less) placebo-controlled clinical trials (3,342 treated with quetiapine and 1,490 treated with placebo), the percent of patients who had a fasting blood glucose ≥ 7.0 mmol/L or a non-fasting blood glucose ≥ 11.1 mmol/L was 3.5% for quetiapine and 2.1% for placebo.
In a 24-week trial (active-controlled, 115 patients treated with quetiapine fumarate) designed to evaluate glycemic status with oral glucose tolerance testing of all patients, at week 24 the incidence of a treatment-emergent post-glucose challenge glucose level ≥ 11.1 mmol/L was 1.7% and the incidence of a fasting treatment-emergent blood glucose level ≥ 7.0 mmol/L was 2.6% (see Endocrine and Metabolism: Hyperglycemia under Precautions).
Cholesterol and Triglyceride Elevations: Very common (≥ 10%) cases of elevations in serum triglyceride levels (≥ 2.258 mmol/L on at least one occasion), elevations in total cholesterol (predominantly LDL cholesterol) (≥ 6.2064 mmol/L on at least one occasion), and decreases in HDL cholesterol levels (< 1.025 mmol/L males; < 1.282 mmol/L females at any time) have been observed during treatment with quetiapine in clinical trials (see Endocrine and Metabolism: Cholesterol and Triglyceride Elevations under Precautions). Lipid changes should be managed as clinically appropriate.
In one 24-week clinical trial, where LDL cholesterol was directly measured as opposed to calculated, there was a slight mean increase in total cholesterol in patients administered quetiapine fumarate, which was driven by increases in LDL cholesterol. The mean LDL level increased at Week 24 by 10% in patients administered quetiapine fumarate, which was statistically significant. The total cholesterol/HDL ratio did not change significantly during therapy with quetiapine fumarate. Furthermore, triglycerides did not increase significantly, nor did HDL cholesterol decrease during therapy (see Endocrine and Metabolism: Cholesterol and Triglyceride Elevations under Precautions).
Adverse Drug Reactions in Pediatrics (< 18 years of age): The safety and efficacy of quetiapine fumarate in children under the age of 18 years have not been established and its use is not recommended.
The same adverse drug reactions described previously for adults should be considered for children and adolescents. The following table summarizes adverse drug reactions that occur in a higher frequency category in children and adolescent patients (ages 10-17 years) than in the adult population or adverse drug reactions that have not been identified in the adult population, based on data for formulations containing quetiapine (see Use in Children: Pediatrics (< 18 years of age) under Precautions). (See Table 12.)
Click on icon to see table/diagram/image
Weight Gain in Children and Adolescents: In one 6-week, placebo-controlled trial in adolescent patients (13-17 years of age) with schizophrenia, the mean increase in body weight, was 2.0 kg in the quetiapine fumarate group and -0.4 kg in the placebo group. Twenty one percent of quetiapine fumarate treated patients and 7% of placebo-treated patients gained ≥ 7 % of their body weight.
In one 3-week, placebo-controlled trial in children and adolescent patients (10-17 years of age) with bipolar mania, the mean increase in body weight was 1.7 kg in the quetiapine fumarate group and 0.4 kg in the placebo group. Twelve percent of quetiapine fumarate treated patients and 0% of placebo-treated patients gained ≥ 7 % of their body weight.
In the open-label study that enrolled patients from the previously mentioned two trials, 63% of patients (241/380) completed 26 weeks of therapy with quetiapine fumarate. After 26 weeks of treatment, the mean increase in body weight was 4.4 kg. Forty five percent of the patients gained ≥ 7% of their body weight, not adjusted for normal growth. In order to adjust for normal growth over 26 weeks, an increase of at least 0.5 standard deviation from baseline in BMI was used as a measure of a clinically significant change; 18.3% of patients on quetiapine fumarate met this criterion after 26 weeks of treatment.
In one 8-week, placebo-controlled trial in children and adolescent patients (10-17 years of age) with bipolar depression, the mean increase in body weight was 1.4 kg in the quetiapine fumarate extended-release tablet group and 0.6 kg in the placebo group. 13.7 % of quetiapine fumarate extended-release tablet-treated patients and 6.8% of placebo-treated patients gained ≥ 7 % of their body weight.
Cumulatively, 17% of quetiapine treated children and adolescents gained ≥ 7% of their body weight versus 2.5% of placebo treated in these studies. In contrast, 9.6% of adults treated with quetiapine gained ≥ 7% of their body weight versus 3.8% of placebo treated based on the cumulative acute placebo-controlled clinical trial database.
Extrapyramidal Symptoms in Children and Adolescent Population: Across the placebo-controlled studies, the incidences of adverse events potentially related to extrapyramidal symptoms for adolescents and children in both schizophrenia and bipolar mania were higher in quetiapine treated patients, a finding that was not observed in trials of adults with these indications.
In a short-term placebo-controlled monotherapy trial in adolescent patients (13-17 years of age) with schizophrenia, the aggregated incidence of extrapyramidal symptoms was 12.9% for quetiapine fumarate and 5.3% for placebo, though the incidence of the individual adverse events (e.g., akathisia, tremor, extrapyramidal disorder, hypokinesia, restlessness, psychomotor hyperactivity, muscle rigidity, dyskinesia) was generally low and did not exceed 4.1% in any treatment group. In a short-term placebo-controlled monotherapy trial in children and adolescent patients (10-17 years of age) with bipolar mania, the aggregated incidence of extrapyramidal symptoms was 3.6% for quetiapine fumarate and 1.1% for placebo.
In a short-term placebo-controlled monotherapy trial in children and adolescent patients (10-17 years of age) with bipolar depression, the aggregated incidence of extrapyramidal symptoms was 1.1% for quetiapine fumarate extended-release tablets and 0.0% for placebo.
Cholesterol and Triglyceride Elevations: Very common (≥ 10%) cases of elevations in serum triglyceride levels (≥ 1.69 mmol/L on at least one occasion), elevations in total cholesterol (predominantly LDL cholesterol) (≥ 5.172 mmol/L on at least one occasion) have been observed during treatment with quetiapine in patients < 18 years of age in clinical trials.
Increased Blood Pressure: In placebo-controlled trials in children and adolescents with schizophrenia (6-week duration) or bipolar mania (3-week duration), the incidence of increases at any time in systolic blood pressure (≥ 20 mmHg) was 15.2% (51/335) for quetiapine fumarate and 5.5% (9/163) for placebo; the incidence of increases at any time in diastolic blood pressure (≥ 10 mmHg) was 40.6% (136/335) for quetiapine fumarate and 24.5% (40/163) for placebo. In the 26-week open-label clinical trial, one child with a reported history of hypertension experienced a hypertensive crisis.
Suicide Related Events: Although not indicated, in clinical trials in patients < 18 years of age with schizophrenia, the incidence of suicide-related events was 1.4% (2/147) for quetiapine and 1.3% (1/75) for placebo.
Although not indicated, in clinical trials in patients < 18 years of age with bipolar mania, the incidence of suicide-related events was 1.0% (2/193) for quetiapine and 0% (0/90) for placebo.
Although not indicated, there has been one trial conducted in patients 10-17 years of age with bipolar depression. The incidence of suicide-related events was 1.0% (1/92) for quetiapine and 0% (0/100) for placebo. In this study there were two additional events in two patients that occurred during an extended post-treatment follow-up phase of the study; one of these patients was on quetiapine at the time of the event.
Post-Market Adverse Drug Reactions: The following adverse reactions were identified during post approval use of quetiapine. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
During post-marketing experience, leucopenia and/or neutropenia have been reported during quetiapine fumarate treatment. Resolution of leucopenia and/or neutropenia has followed cessation of therapy with quetiapine fumarate. Possible risk factors for leucopenia and/or neutropenia include pre-existing low white cell count and history of drug induced leucopenia and/or neutropenia. In post-marketing reports, there have been cases of agranulocytosis (including fatal cases) in patients administered quetiapine (see Hematologic: Leukopenia, Neutropenia and Agranulocytosis under Precautions).
Drug reaction with eosinophilia and systemic symptoms (DRESS) has been reported with unknown frequency (see Skin under Precautions).
As with other antipsychotics, hyperglycemia and diabetes mellitus (including exacerbation of pre-existing diabetes, diabetic ketoacidosis, and diabetic coma including some fatal cases) in the aggregate have been reported rarely (≥ 0.01% - < 0.1%) during the use of quetiapine fumarate, sometimes in patients with no reported history of hyperglycemia (see Endocrine and Metabolism: Hyperglycemia under Precautions).
Anaphylactic reactions have been reported very rarely in post-marketing reports, including a case with a fatal outcome, possibly related to quetiapine fumarate treatment. The reporting rate of anaphylaxis associated with quetiapine fumarate use, which is generally accepted to be an underestimate due to underreporting, does not exceed the background incidence rate estimates. Estimates of the background incidence rate (all cause) of severe life-threatening anaphylaxis in the general population range between 80 and 210 cases per million person-years, and the incidence rate of drug-induced anaphylaxis is reported to be 16 cases per million person-years. In addition, the all cause fatal anaphylaxis rate is reported to be one case per million person-years, while the drug-induced fatal anaphylaxis is estimated to be 0.3 cases per million person-years. If a patient develops anaphylaxis after treatment with quetiapine, the drug should be discontinued and an alternative treatment started.
In patients who have a history of or are at risk for sleep apnea, and are receiving concomitant central nervous system (CNS) depressants, quetiapine should be prescribed with caution.
Based on post-marketing reports, galactorrhea has been reported rarely.
During post-marketing experience, there have been cases of intestinal obstruction (ileus) in patients administered quetiapine (see Gastrointestinal: Constipation and Intestinal Obstruction under Precautions).
Although there have been post-marketing cases of neonatal withdrawal in mothers administered quetiapine, the frequency is unknown (see Use in Children: Neonates under Precautions).
In post-marketing reports, there have been cases of urinary retention in patients administered quetiapine (see Neurologic: Anticholinergic (Muscarinic) Effects under Precautions).
Hepatic failure, including fatalities, has been reported very rarely during the post-marketing period. Rare post-marketing reports of hepatitis (with or without jaundice), in patients with or without prior history, have been received. Very rare cases of hepatic steatosis, cholestatic or mixed liver injury have also been reported in the post-marketing period (see Hepatic/Pancreatic: Transaminase Elevations under Precautions).
Other adverse reactions reported since market introduction, which were temporally related to quetiapine therapy, but not necessarily causally related include the following: rhabdomyolysis, cardiomyopathy, myocarditis (see Cardiovascular: Cardiomyopathy and Myocarditis under Precautions) and syndrome of inappropriate secretion of antidiuretic hormone (SIADH).


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image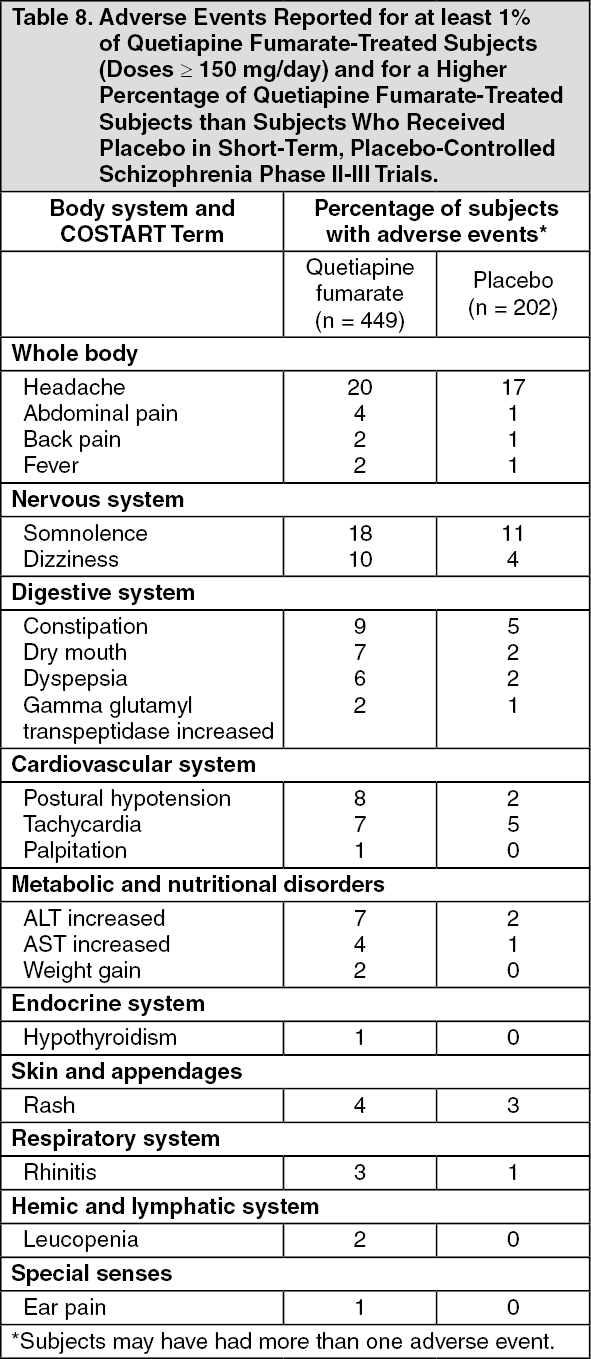 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image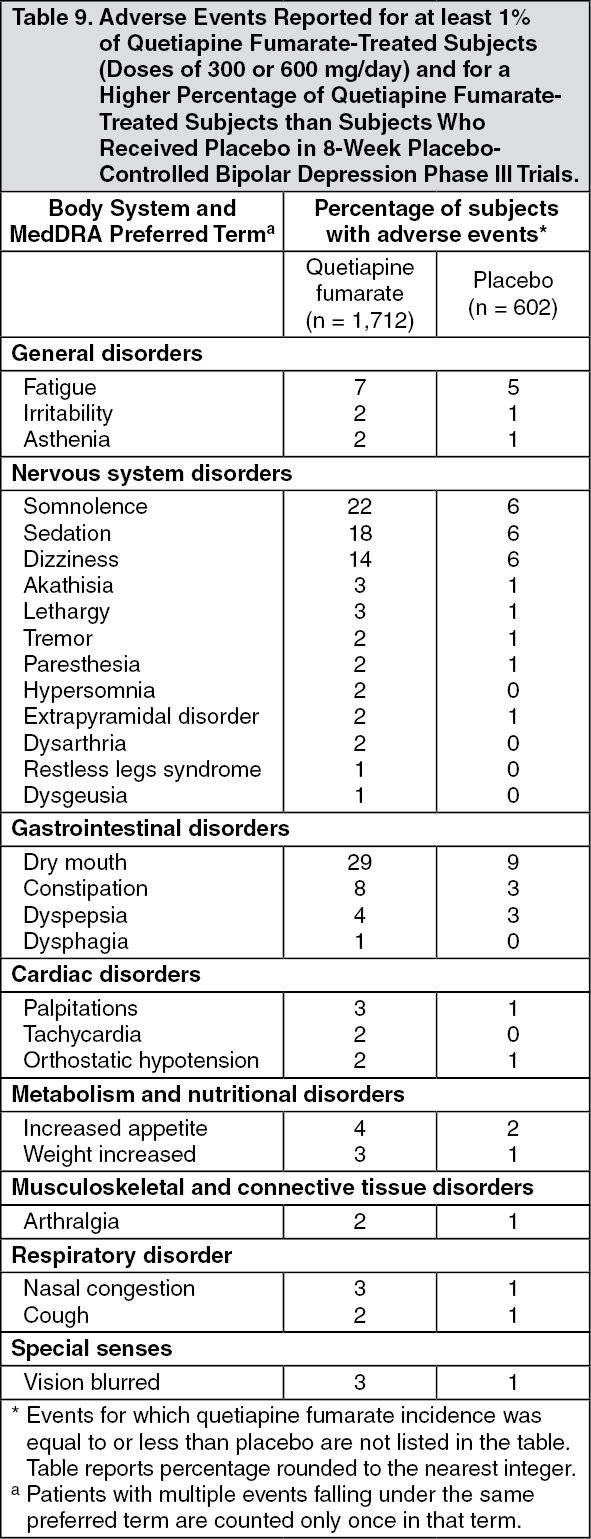 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image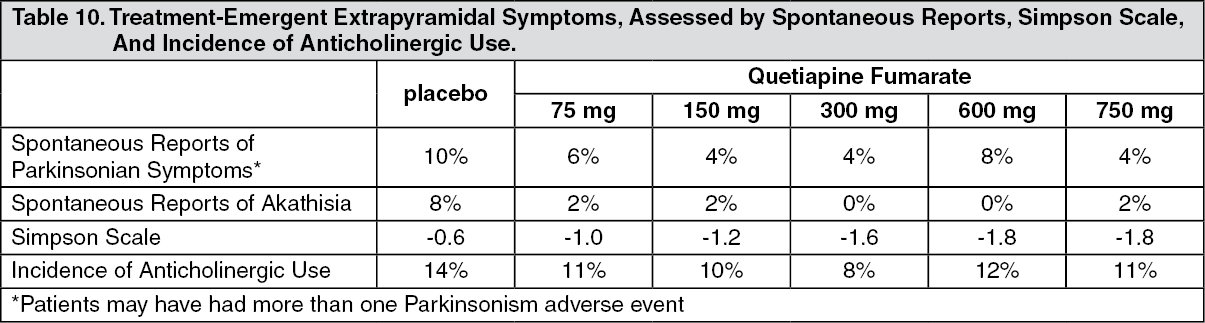 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image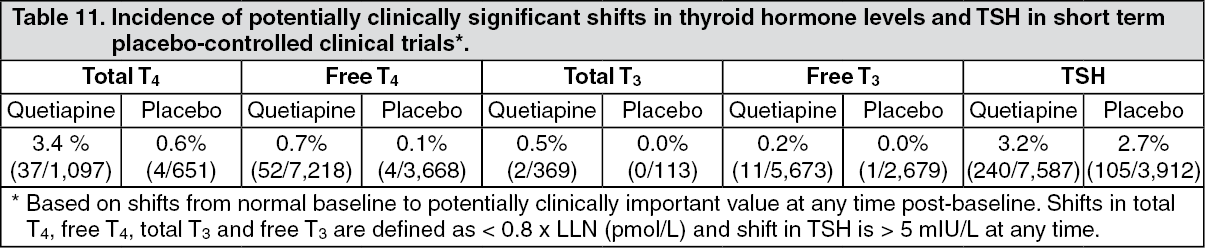 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image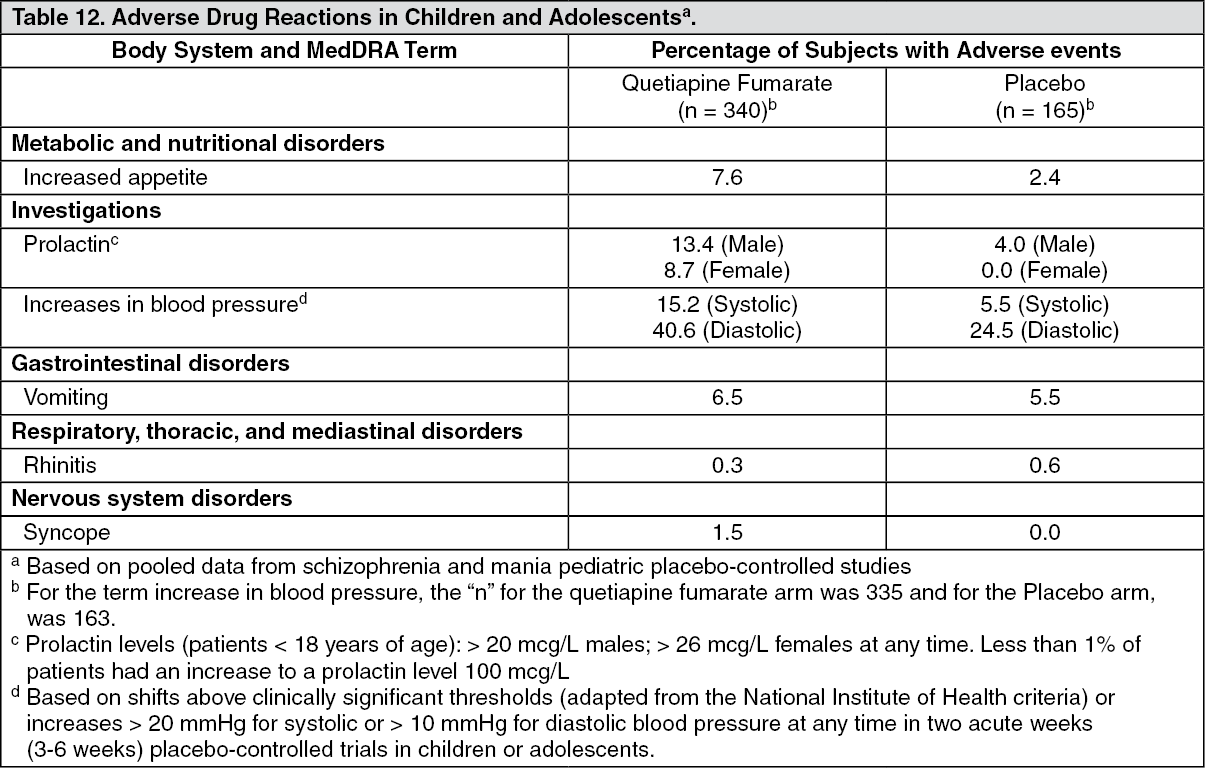 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
