Each film-coated tablet contains 1 mg prucalopride (as succinate).
White to off-white, round, biconvex tablets marked "PRU 1" on one side.
Excipients with known effect: Each film-coated tablet contains 150 mg lactose monohydrate.
Excipients/Inactive Ingredients: Tablet core: Lactose monohydrate, Microcrystalline cellulose, Colloidal silicon dioxide, Magnesium stearate.
Tablet coating: Hypromellose, Lactose monohydrate, Triacetin, Titanium dioxide (E171), Macrogol.
Pharmacotherapeutic group: Other drugs for constipation. ATC code: A06AX05.
Pharmacology: Pharmacodynamics: Mechanism of action: Prucalopride is a dihydrobenzofurancarboxamide with gastrointestinal prokinetic activities.
Prucalopride is a selective, high affinity serotonin (5-HT4) receptor agonist, which is likely to explain its prokinetic effects. In vitro, only at concentrations exceeding its 5-HT4 receptor affinity by at least 150-fold, affinity for other receptors was detected. In rats, prucalopride in vivo, at doses above 5 mg/kg (at and above 30-70 times the clinical exposure), induced hyperprolactinaemia caused by an antagonistic action at the D2 receptor.
In dogs, prucalopride alters colonic motility patterns via serotonin 5-HT4 receptor stimulation: it stimulates proximal colonic motility, enhances gastroduodenal motility and accelerates delayed gastric emptying. Furthermore, giant migrating contractions are induced by prucalopride. These are equivalent to the colonic mass movements in humans, and provide the main propulsive force to defecation. In dogs, the effects observed in the gastrointestinal tract are sensitive to blockade with selective 5-HT4 receptor antagonists illustrating that the observed effects are exerted via selective action on 5-HT4 receptors.
These pharmacodynamic effects of prucalopride have been confirmed in human subjects with chronic constipation using manometry in an open-label, randomised, crossover, reader-blinded study investigating the effect of prucalopride 2 mg and an osmotic laxative on colon motility as determined by the number of colonic high-amplitude propagating contractions (HAPCs, also known as giant migrating contractions). Compared with a constipation treatment working through osmotic action, prokinetic stimulation with prucalopride increased colonic motility as measured by the number of HAPCs during the first 12 hours after intake of the investigational product. The clinical significance or benefit of this mechanism of action when compared with other laxatives has not been investigated.
Clinical efficacy and safety: Adult population: The efficacy of Resolor was established in three multicentre, randomised, double-blind, 12-week placebo-controlled studies in subjects with chronic constipation (n=1,279 on Resolor, 1,124 females, 155 males). The Resolor doses studied in each of these three studies included 2 mg and 4 mg once daily. The primary efficacy endpoint was the proportion (%) of subjects that reached normalisation of bowel movements defined as an average of three or more spontaneous, complete bowel movements (SCBM) per week over the 12-week treatment period.
The proportion of female patients in whom laxatives fail to provide adequate relief treated with the recommended dose of 2 mg Resolor (n=458) that reached an average of ≥ 3 SCBM per week was 31.0% (week 4) and 24.7% (week 12), versus 8.6% (week 4) and 9.2% (week 12) on placebo. A clinically meaningful improvement of ≥ 1 SCBM per week, the most important secondary efficacy endpoint, was achieved in 51.0% (week 4) and 44.2% (week 12) treated with 2 mg Resolor versus 21.7% (week 4) and 22.6% (week 12) of placebo patients.
The effect of Resolor on spontaneous bowel movements (SBM) also proved to be statistically superior to placebo for the portion of patients that had an increase of ≥1 SBM/week over the 12-week treatment period. At week 12, 68.3% of patients treated with 2 mg prucalopride had an average increase of ≥1 SBM/week versus 37.0% of placebo patients (p<0.001 vs placebo).
In all three studies, treatment with Resolor also resulted in significant improvements in a validated and disease specific set of symptom measures (PAC-SYM), including abdominal (bloating, discomfort, pain and cramps), stool (incomplete bowel movements, false alarm, straining, too hard, too small) and rectal symptoms (painful bowel movements, burning, bleeding/tearing), determined at week 4 and week 12. At week 4, the proportion of patients with an improvement of ≥1 versus baseline in the PAC-SYM abdominal, stool, and rectal symptom subscales was 41.3%, 41.6%, and 31.3% respectively in patients treated with prucalopride 2 mg compared with 26.9%, 24.4% and 22.9% in patients on placebo. Similar results were observed at Week 12: 43.4%, 42.9%, and 31.7% respectively in 2 mg Resolor patients versus 26.9%, 27.2%, and 23.4% in placebo patients (p<0.001 vs placebo).
A significant benefit on a number of Quality of Life measures, such as degree of satisfaction with treatment and with bowel habits, physical and psychosocial discomfort and worries and concerns, was also observed at both the 4 and 12 week assessment time points. At Week 4, the proportion of patients with an improvement of ≥1 versus baseline in the Patient Assessment of Constipation-Quality of Life satisfaction subscale (PAC-QOL) was 47.7% in patients treated with Resolor 2 mg compared with 20.2% in patients on placebo. Similar results were observed at Week 12: 46.9% in 2 mg Resolor patients versus 19.0% in placebo patients (p<0.001 vs placebo).
In addition, the efficacy, safety and tolerability of Resolor in male patients with chronic constipation were evaluated in a 12-week, multi-centre, randomised, double-blind, placebo-controlled study (N=370). The primary endpoint of the study was met: a statistically significantly higher percentage of subjects in the Resolor group (37.9%) had an average of ≥ 3 SCBMs/week compared with subjects in the placebo treatment group (17.7%) (p<0.0001) over the 12-week double-blind treatment period. The safety profile of Resolor was consistent with that seen in female patients.
Long-term study: The efficacy and safety of Resolor in patients (aged ≥18 or older) with chronic constipation, were evaluated in a 24 week multicentre, randomised, double-blind, placebo controlled study (N=361). The proportion of patients with an average weekly frequency of ≥3 Spontaneous Complete Bowel Movements (SCBMs) per week (i.e., responders) over the 24-week double-blind treatment phase was not statistically different (p=0.367) between the Resolor (25.1%) and placebo (20.7%) treatment groups. The difference between treatment groups in the average weekly frequency of ≥3 SCBMs per week was not statistically significant over Weeks 1-12 which is inconsistent with the 5 other multicentre, randomised, double-blind, 12-week placebo controlled studies demonstrating efficacy at this timepoint in adult patients. The study is therefore considered to be inconclusive with respect to efficacy. However, the totality of the data including the other double-blind placebo controlled 12 week studies support the efficacy of Resolor. The safety profile of prucalopride in this 24 week study was consistent with that seen in the previous 12 week studies.
Resolor has been shown not to cause rebound phenomena, nor to induce dependency.
TQT study: A thorough QT study was performed to evaluate the effects of Resolor on the QT interval at therapeutic (2 mg) and supratherapeutic doses (10 mg) and compared with the effects of placebo and a positive control. This study did not show significant differences between Resolor and placebo at either dose, based on mean QT measurements and outlier analysis. This confirmed the results of two placebo controlled QT studies. In double-blind clinical studies, the incidence of QT-related adverse events and ventricular arrhythmias was low and comparable to placebo.
Paediatric population: The efficacy and safety of Resolor in paediatric patients (aged 6 months to 18 years) with functional constipation, were evaluated in an 8-week double-blind, placebo-controlled trial (N = 213), followed by a 16 week open-label comparator-controlled (Polyethylene glycol 4000) study of up to 24 weeks (N = 197). The starting dose administered was 0.04 mg/kg/day titrated between 0.02 and 0.06 mg/kg/day (to a maximum of 2 mg daily) for children weighing ≤ 50 kg given as an oral solution of Resolor or matching placebo. Children weighing > 50 kg received 2 mg/day Resolor tablets or matching placebo.
Response to the treatment was defined as having an average of ≥ 3 spontaneous bowel movements (SBMs) per week and an average number of faecal incontinence episodes of ≤ 1 per 2 weeks. The results of the study showed no difference in efficacy between Resolor and placebo with response rates of 17% and 17.8% respectively (P= 0.9002). Resolor was generally well tolerated. The incidence of subjects with at least 1 treatment-emergent adverse event (TEAE) was similar between the Resolor treatment group (69.8%) and the placebo treatment group (60.7%). Overall, the safety profile of Resolor in children was the same as in adults.
Pharmacokinetics: Absorption: Prucalopride is rapidly absorbed; after a single oral dose of 2 mg in healthy subjects, Cmax was attained in 2-3 hours. The absolute oral bioavailability is >90%. Concomitant intake of food does not influence the oral bioavailability of prucalopride.
Distribution: Prucalopride is extensively distributed, and has a steady-state volume of distribution (Vdss) of 567 litres. The plasma protein binding of prucalopride is about 30%.
Biotransformation: Metabolism is not the major route of elimination of prucalopride. In vitro, human liver metabolism is very slow and only minor amounts of metabolites are found. In an oral dose study with radiolabelled prucalopride in man, small amounts of seven metabolites were recovered in urine and faeces. The quantitatively most important metabolite in excreta, R107504, accounted for 3.2% and 3.1% of the dose in urine and faeces, respectively. Other metabolites identified and quantified in urine and faeces were R084536 (formed by N-dealkylation) accounting for 3% of the dose and products of hydroxylation (3% of the dose) and N-oxidation (2% of the dose). Unchanged active substance made up about 92-94% of the total radioactivity in plasma. R107504, R084536 and R104065 (formed by O-demethylation) were identified as minor plasma metabolites.
Elimination: A large fraction of the active substance is excreted unchanged (60-65% of the administered dose in urine and about 5% in faeces). Renal excretion of unchanged prucalopride involves both passive filtration and active secretion. The plasma clearance of prucalopride averages 317 ml/min. Its terminal half-life is about one day. Steady-state is reached within three to four days. On once daily treatment with 2 mg prucalopride, steady-state plasma concentrations fluctuate between trough and peak values of 2.5 and 7 ng/ml, respectively. The accumulation ratio after once daily dosing ranged from 1.9 to 2.3. The pharmacokinetics of prucalopride is dose-proportional within and beyond the therapeutic range (tested up to 20 mg). Prucalopride o.d. displays time-independent kinetics during prolonged treatment.
Special populations: Population pharmacokinetics: A population pharmacokinetic analysis showed that the apparent total clearance of prucalopride was correlated with creatinine clearance, but that age, body weight, sex or race had no influence.
Older people: After once daily dosing of 1 mg, peak plasma concentrations and AUC of prucalopride in older people were 26% to 28% higher than in young adults. This effect can be attributed to a diminished renal function in older people.
Renal impairment: Compared to subjects with normal renal function, plasma concentrations of prucalopride after a single 2 mg dose were on average 25% and 51% higher in subjects with mild (ClCR 50-79 ml/min) and moderate (ClCR 25-49 ml/min) renal impairment, respectively. In subjects with severe renal impairment (ClCR ≤ 24 ml/min), plasma concentrations were 2.3 times the levels in healthy subjects (see Dosage & Administration and Precautions).
Hepatic impairment: Non-renal elimination contributes to about 35% of total elimination. In a small pharmacokinetic study, the Cmax and AUC of prucalopride were, on average, 10-20% higher in patients with moderate to severe hepatic impairment compared with healthy subjects (see Dosage & Administration and Precautions).
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, and toxicity to reproduction and development. An extended series of safety pharmacology studies with special emphasis on cardiovascular parameters showed no relevant changes in haemodynamic and ECG derived parameters (QTc) with the exception of a modest increase in heart rate and blood pressure observed in anaesthetised pigs after intravenous administration, and an increase in blood pressure in conscious dogs after bolus intravenous administration, which was not observed either in anaesthetised dogs or after oral administration in dogs reaching similar plasma levels. A subcutaneous neonatal/juvenile toxicity study performed in rats 7-55 days of age resulted in a NOAEL of 10 mg/kg/day. The AUC0-24h exposure ratios at the NOAEL versus human children (dosed at approximately 0.04 mg/kg daily) ranged between 21 and 71 providing adequate safety margins for the clinical dose.
Resolor is indicated for symptomatic treatment of chronic constipation in adults in whom laxatives fail to provide adequate relief.
Posology: Adults: 2 mg once daily with or without food, at any time of the day.
Due to the specific mode of action of prucalopride (stimulation of propulsive motility), exceeding the daily dose of 2 mg is not expected to increase efficacy.
If the intake of once daily prucalopride is not effective after 4 weeks of treatment, the patient should be re-examined and the benefit of continuing treatment reconsidered.
The efficacy of prucalopride has been established in double-blind, placebo-controlled studies for up to 3 months. Efficacy beyond three months has not been demonstrated in placebo-controlled studies (see Pharmacology: Pharmacodynamics under Actions). In case of prolonged treatment, the benefit should be reassessed at regular intervals.
Special populations: Older people (>65 years): Start with 1 mg once daily (see Pharmacology: Pharmacokinetics under Actions); if needed the dose can be increased to 2 mg once daily.
Patients with renal impairment: The dose for patients with severe renal impairment (GFR < 30 ml/min/1.73 m2) is 1 mg once daily (see Contraindications and Pharmacology: Pharmacokinetics under Actions). No dose adjustment is required for patients with mild to moderate renal impairment.
Patients with hepatic impairment: Patients with severe hepatic impairment (Child-Pugh class C) start with 1 mg once daily which may be increased to 2 mg if required to improve efficacy and if the 1 mg dose is well tolerated (see Precautions and Pharmacology: Pharmacokinetics under Actions). No dose adjustment is required for patients with mild to moderate hepatic impairment.
Paediatric population: Resolor should not be used in children and adolescents younger than 18 years (see Pharmacology: Pharmacodynamics under Actions).
Method of administration: Oral use.
In a study in healthy volunteers, treatment with prucalopride was well tolerated when given in an up-titrating scheme up to 20 mg once daily (10 times the recommended therapeutic dose). An overdose may result in symptoms resulting from an exaggeration of prucalopride's known pharmacodynamic effects and include headache, nausea and diarrhoea. Specific treatment is not available for Resolor overdose. Should an overdose occur, the patient should be treated symptomatically and supportive measures instituted, as required. Extensive fluid loss by diarrhoea or vomiting may require correction of electrolyte disturbances.
Hypersensitivity to the active substance or to any of the excipients listed in Description.
Renal impairment requiring dialysis.
Intestinal perforation or obstruction due to structural or functional disorder of the gut wall, obstructive ileus, severe inflammatory conditions of the intestinal tract, such as Crohn's disease, and ulcerative colitis and toxic megacolon/megarectum.
Renal excretion is the main route of elimination of prucalopride (see Pharmacology: Pharmacokinetics under Actions). A dose of 1 mg is recommended in subjects with severe renal impairment (see Dosage & Administration).
Caution should be exercised when prescribing Resolor to patients with severe hepatic impairment (Child-Pugh class C) due to limited data in patients with severe hepatic impairment (see Dosage & Administration).
There is limited information on the safety and efficacy of Resolor for use in patients with severe and clinically unstable concomitant disease (e.g. cardiovascular or lung disease, neurological or psychiatric disorders, cancer or AIDS and other endocrine disorders). Caution should be exercised when prescribing Resolor to patients with these conditions especially when used in patients with a history of arrhythmias or ischaemic cardiovascular disease.
In case of severe diarrhoea, the efficacy of oral contraceptives may be reduced and the use of an additional contraceptive method is recommended to prevent possible failure of oral contraception (see the prescribing information of the oral contraceptive).
The tablets contain lactose. Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicinal product.
Effects on ability to drive and use machines: Resolor may have a minor influence on the ability to drive and use machines, since dizziness and fatigue have been observed in clinical studies, particularly during the first day of treatment (see Adverse Reactions).
Women of childbearing potential: Women of childbearing potential have to use effective contraception during treatment with prucalopride.
Pregnancy: There is a limited amount of data from the use of prucalopride in pregnant women. Cases of spontaneous abortion have been observed during clinical studies, although, in the presence of other risk factors, the relationship to prucalopride is unknown. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity (including pregnancy, embryonal/foetal development, parturition or postnatal development) (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Resolor is not recommended during pregnancy and in women of childbearing potential not using contraception.
Breast-feeding: A human study has shown that prucalopride is excreted in breast milk. At therapeutic doses of Resolor, no effects on breast-fed newborns/infants are anticipated. In the absence of human data in women who actively breast fed while taking Resolor, a decision should be made whether to discontinue breast feeding or to discontinue Resolor therapy taking into account the benefit of breast feeding for the child and the benefit of therapy for the woman.
Fertility: Animal studies indicate that there is no effect on male or female fertility.
Summary of the safety profile: In an integrated analysis of 17 double-blind placebo-controlled studies, Resolor was given orally to approximately 3,300 patients with chronic constipation. Of these, over 1,500 patients received Resolor at the recommended dose of 2 mg per day, while approximately 1,360 patients were treated with 4 mg prucalopride daily. The most frequently reported adverse reactions associated with Resolor 2 mg therapy are headache (17.8%) and gastrointestinal symptoms (abdominal pain (13.7%), nausea (13.7%) and diarrhoea (12.0%)). The adverse reactions occur predominantly at the start of therapy and usually disappear within a few days with continued treatment. Other adverse reactions have been reported occasionally. The majority of adverse events were mild to moderate in intensity.
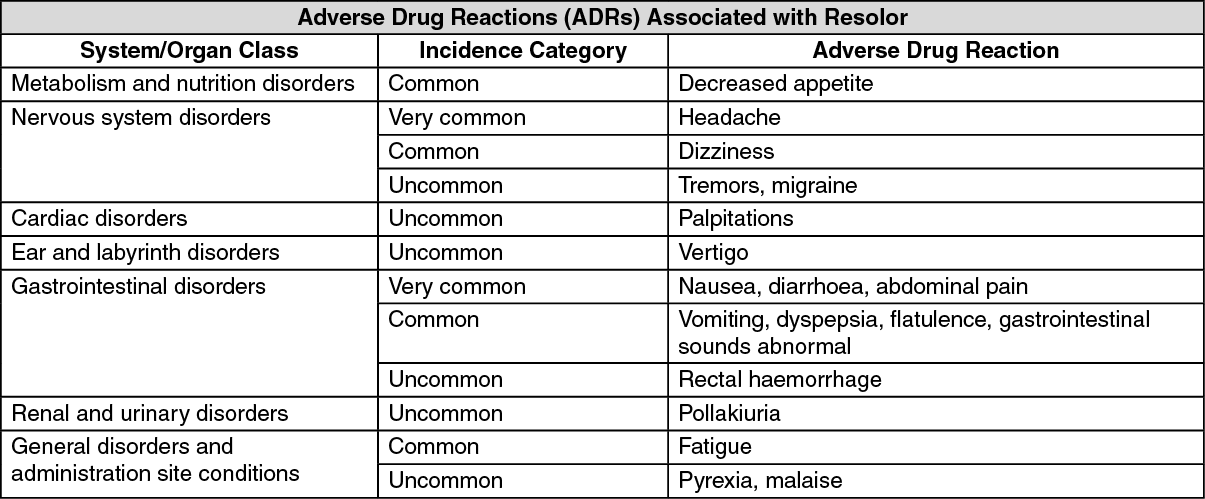
Tabulated list of adverse reactions: The following adverse reactions were reported in controlled clinical studies at the recommended dose of 2 mg with frequencies corresponding to very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000) and not known (cannot be estimated from the available data). Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. Frequencies are calculated based on the integrated analysis of 17 double-blind placebo-controlled clinical studies. (See table.)
 Click on icon to see table/diagram/image
Description of selected adverse reactions:
Click on icon to see table/diagram/image
Description of selected adverse reactions: After the first day of treatment, the most common adverse reactions were reported in similar frequencies (incidence no more than 1% different between prucalopride and placebo) during Resolor therapy as during placebo, with the exception of nausea and diarrhoea that still occurred more frequently during Resolor therapy, but less pronounced (differences in incidence between Resolor and placebo of 1.3% and 3.4%, respectively).
Palpitations were reported in 0.7% of the placebo patients, 0.9% of the 1 mg prucalopride patients, 0.9% of the 2 mg prucalopride patients and 1.9% of the 4 mg prucalopride patients. The majority of patients continued using prucalopride. As with any new symptom, patients should discuss the new onset of palpitations with their physician.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via local guideline.
Prucalopride has a low pharmacokinetic interaction potential. It is extensively excreted unchanged in urine (approximately 60% of the dose) and in vitro metabolism is very slow.
Prucalopride did not inhibit specific CYP450 activities in in vitro studies in human liver microsomes at therapeutically relevant concentrations.
Although prucalopride may be a weak substrate for P-glycoprotein (P-gp), it is not an inhibitor of P-gp at clinically relevant concentrations.
Effects of prucalopride on pharmacokinetics of other medicinal products: A 30% increase in plasma concentrations of erythromycin was found during prucalopride co-administration. The mechanism for this interaction is not clear.
Prucalopride had no clinically relevant effects on the pharmacokinetics of warfarin, digoxin, alcohol, paroxetine or oral contraceptives.
Effects of other medicinal products on pharmacokinetics of prucalopride: Ketoconazole (200 mg twice daily), a potent inhibitor of CYP3A4 and of P-gp, increased the systemic exposure to prucalopride by approximately 40%. This effect is too small to be clinically relevant.
Interactions of similar magnitude may be expected with other potent inhibitors of P-gp such as verapamil, cyclosporine A and quinidine.
Therapeutic doses of probenecid, cimetidine, erythromycin and paroxetine did not affect the pharmacokinetics of prucalopride.
Special precautions for disposal: No special requirements.
Incompatibilities: Not applicable.
Do not store above 30°C.
Store in the original blister in order to protect from moisture.
A06AX05 - prucalopride ; Belongs to the class of other laxatives.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out