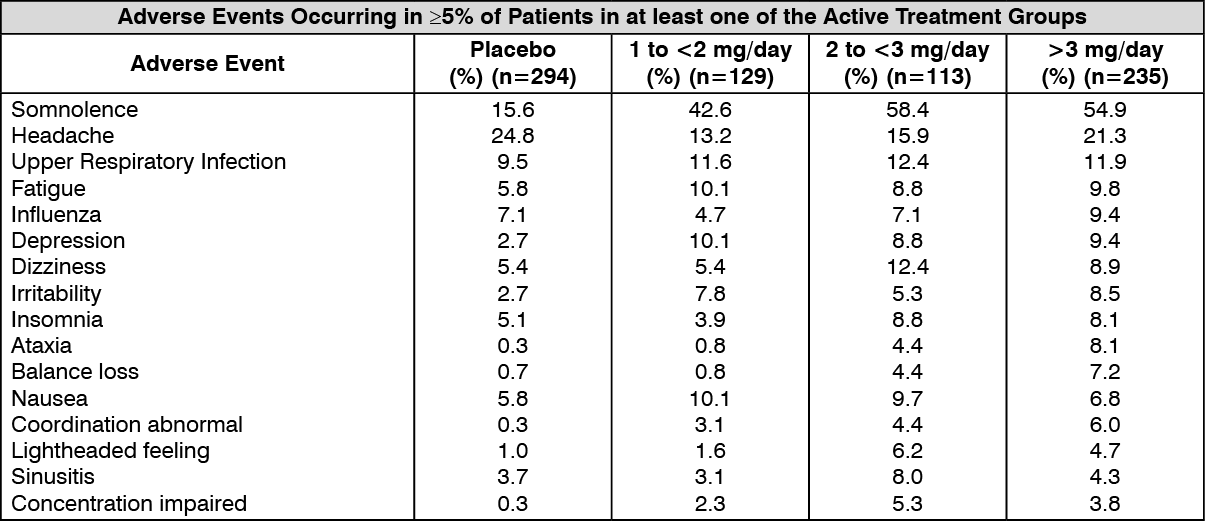
Clinical Trials: Panic Disorder: Data from 3 placebo-controlled clinical trials including 477 patients on active treatment in total are presented in the following table. Adverse events occurring in ≥5% of patients in at least one of the active treatment groups are included. (See table.)
 Click on icon to see table/diagram/image
Post Marketing: Immune System Disorders:
Click on icon to see table/diagram/image
Post Marketing: Immune System Disorders: Allergic reactions and very few cases of anaphylaxis have been reported to occur with benzodiazepines.
Endocrine Disorders: Isolated cases of reversible development of premature secondary sex characteristics in children (incomplete precocious puberty) have been reported.
Psychiatric Disorders: Impaired concentration, restlessness, confusional state, disorientation have been observed. Depression may occur in patients treated with Rivotril, but it may be also associated with the underlying disease.
The following paradoxical reactions have been observed: excitability, irritability, aggression, agitation, nervousness, hostility, anxiety, sleep disturbances, nightmares and vivid dreams.
In rare cases, loss of libido may occur.
Dependence and withdrawal (see Drug Abuse and Dependence under Precautions).
Nervous System Disorders: Somnolence, slowed reaction, muscular hypotonia, dizziness, ataxia. These undesirable effects occur relatively frequently and are usually transient and generally disappear spontaneously in the course of the treatment or on reduction of the dosage. They can be partially prevented by increasing the dose slowly at the start of treatment.
Headache was observed in rare cases.
Particularly in long-term or high-dose treatment, reversible disorders such as dysarthria, reduced coordination of movements and gait disorder (ataxia) and nystagmus may occur.
Anterograde amnesia may occur using benzodiazepines at therapeutic dosages, the risk increasing at higher dosages. Amnestic effects may be associated with inappropriate behaviour.
With certain forms of epilepsy, an increase in the frequency of seizures during long-term treatment is possible.
Eye Disorders: Particularly in long-term or high-dose treatment, reversible disorders of vision (diplopia) may occur.
Cardiac Disorders: Cardiac failure including cardiac arrest has been reported.
Respiratory, Thoracic and Mediastinal System Disorders: Respiratory depression may occur. This effect may be aggravated by pre-existing airways obstruction or brain damage or if other medications which depress respiration have been given. As a rule, this effect can be avoided by careful adjustment of the dose to individual requirements.
In infants and young children, Rivotril may cause increased production of saliva or of bronchial secretion. Particular attention should therefore be paid to maintaining patency of the airways.
Gastrointestinal Disorders: The following effects have been reported in rare cases: nausea and epigastric symptoms.
Skin and Subcutaneous Tissue Disorders: The following effects may occur in rare cases: urticaria, pruritus, rash, transient hair loss, pigmentation changes.
Musculoskeletal and Connecting Tissue Disorders: Muscle weakness. This undesirable effect occurs relatively frequently and is usually transient and generally disappears spontaneously in the course of the treatment or on reduction of the dosage. It can be partially prevented by increasing the dose slowly at the start of treatment.
Renal and Urinary Disorders: In rare cases, urinary incontinence may occur.
Reproductive System and Breast Disorders: In rare cases, erectile dysfunction may occur.
General Disorders and Administration Site Conditions: Fatigue (tiredness, lassitude). This undesirable effect occurs relatively frequently and is usually transient and generally disappears spontaneously in the course of the treatment or on reduction of the dosage. It can be partially prevented by increasing the dose slowly at the start of treatment.
Paradoxical reactions including irritability have been observed (see also Psychiatric Disorders as previously mentioned). If the injection is rapid or the caliber of the vein insufficient, there is a risk of thrombophlebitis, which may in turn lead to thrombosis.
Injury, Poisoning and Procedural Complications: There have been reports of falls and fractures in benzodiazepine users. The risk is increased in those taking concomitant sedatives (including alcoholic beverages) and in the elderly.
Investigations: In rare cases, decreased platelet count may occur.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out