


 Sign Out
Sign Out



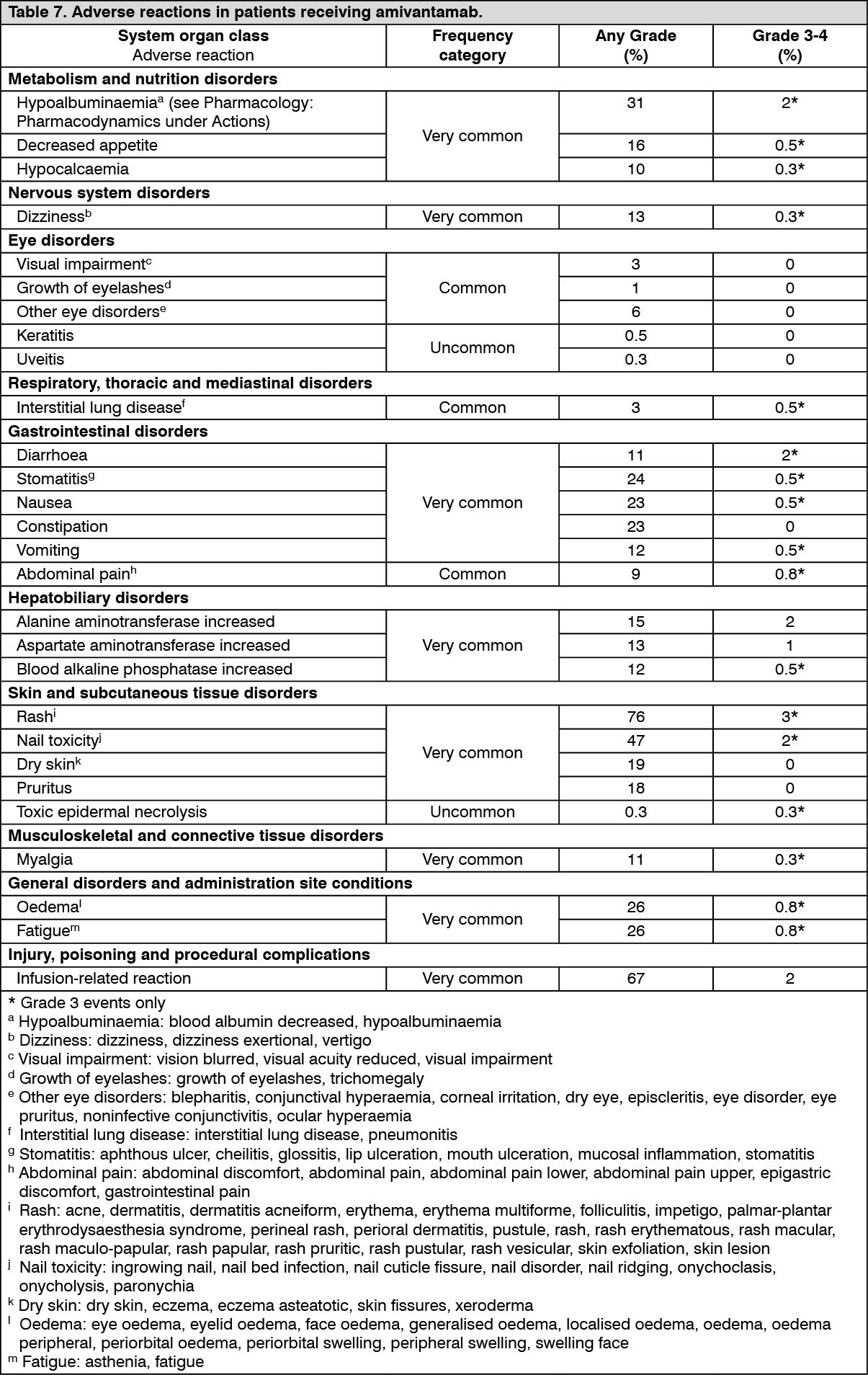
Tabulated list of adverse reactions: Table 7 summarises the adverse drug reactions that occurred in patients receiving amivantamab.
The data reflects exposure to amivantamab in 380 patients with locally advanced or metastatic non-small cell lung cancer after failure of platinum-based chemotherapy. Patients received amivantamab 1,050 mg (for patients < 80 kg) or 1,400 mg (for patients ≥ 80 kg). The median exposure to amivantamab was 4.1 months (range: 0.0 to 39.7 months).
Adverse reactions observed during clinical studies are listed below by frequency category. Frequency categories are defined as follows: very common (≥ 1/10); common (≥ 1/100 to < 1/10); uncommon (≥ 1/1,000 to < 1/100); rare (≥ 1/10,000 to < 1/1,000); very rare (< 1/10,000); and not known (frequency cannot be estimated from the available data).
Within each frequency grouping, adverse reactions are presented in the order of decreasing seriousness. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Infusion-related reactions: Infusion-related reactions occurred in 67% of patients treated with amivantamab. Ninety-eight percent of IRRs were Grade 1-2. Ninety-nine percent of IRRs occurred at the first infusion with a median time to onset of 60 minutes, and the majority occurring within 2 hours of infusion start. The most frequent signs and symptoms include chills, dyspnoea, nausea, flushing, chest discomfort, and vomiting (see Precautions).
Interstitial lung disease: Interstitial lung disease or ILD-like adverse reactions have been reported with the use of amivantamab as well as with other EGFR inhibitors. Interstitial lung disease or pneumonitis was reported in 2.6% of patients. Patients with a medical history of ILD, drug-induced ILD, radiation pneumonitis that required steroid treatment, or any evidence of clinically active ILD were excluded from the clinical study (see Precautions).
Skin and nail reactions: Rash (including dermatitis acneiform), pruritus, and dry skin occurred in 76% of patients treated with amivantamab. Most cases were Grade 1 or 2, with Grade 3 rash events occurring in 3% of patients. Rash leading to amivantamab discontinuation occurred in 0.3% of patients. Rash usually developed within the first 4 weeks of therapy, with a median time to onset of 14 days. Paronychia occurred in patients treated with amivantamab. Most events were Grade 1 or 2, with Grade 3 paronychia occurring in 1.8% of patients (see Precautions).
Eye disorders: Eye disorders, including keratitis (0.5%), occurred in 9% of patients treated with amivantamab. Other reported adverse reactions included growth of eyelashes, visual impairment, and other eye disorders. All events were Grade 1-2 (see Precautions).
Other special populations: Elderly: There are limited clinical data with amivantamab in patients 75 years of age or over (see Pharmacology: Pharmacodynamics under Actions). No overall differences in safety were observed between patients ≥ 65 years of age and patients < 65 years of age.
Immunogenicity: As with all therapeutic proteins, there is the potential for immunogenicity. In a clinical study of patients with locally advanced or metastatic NSCLC treated with amivantamab, 3 (0.9%) of the 347 evaluable patients tested positive for anti-amivantamab antibodies. There was no evidence of an altered pharmacokinetic, efficacy, or safety profile due to anti-amivantamab antibodies.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
View ADR Monitoring Form