


 Sign Out
Sign Out
Pharmacology: Pharmacodynamics: Mechanism of action: Midostaurin inhibits multiple receptor tyrosine kinases, including FLT3 and KIT kinase. Midostaurin inhibits FLT3 receptor signalling and induces cell cycle arrest and apoptosis in leukaemic cells expressing FLT3 ITD or TKD mutant receptors or over-expressing FLT3 wild type receptors. In vitro data indicate that midostaurin inhibits D816V mutant KIT receptors at exposure levels achieved in patients (average achieved exposure higher than IC50). In vitro data indicate that KIT wild type receptors are inhibited to a much lesser extent at these concentrations (average achieved exposure lower than IC50). Midostaurin interferes with aberrant KIT D816V-mediated signalling and inhibits mast cell proliferation, survival and histamine release.
In addition, midostaurin inhibits several other receptor tyrosine kinases such as PDGFR (platelet-derived growth factor receptor) or VEGFR2 (vascular endothelial growth factor receptor 2), as well as members of the serine/threonine kinase family PKC (protein kinase C). Midostaurin binds to the catalytic domain of these kinases and inhibits the mitogenic signalling of the respective growth factors in cells, resulting in growth arrest.
Midostaurin in combination with chemotherapeutic agents (cytarabine, doxorubicin, idarubicin and daunorubicin) resulted in synergistic growth inhibition in FLT3-ITD expressing AML cell lines.
Pharmacodynamic effects: Two major metabolites have been identified in murine models and humans, i.e. CGP62221 and CGP52421. In proliferation assays with FLT3-ITD expressing cells, CGP62221 showed similar potency compared to the parent compound, however CGP52421 was approximately 10-fold less potent.
Cardiac electrophysiology: A dedicated QT study in 192 healthy subjects with a dose of 75 mg twice daily did not reveal clinically significant prolongation of QT by midostaurin and CGP62221 but the study duration was not long enough to estimate the QTc prolongation effects of the long-acting metabolite CGP52421. Therefore, the change from baseline in QTcF with the concentration of midostaurin and both metabolites was further explored in a phase II study in 116 patients with ASM, SM-AHN or MCL. At the median peak Cmin concentrations attained at a dose of 100 mg twice daily, neither midostaurin, CGP62221 nor CGP52421 showed a potential to cause clinically significant QTcF prolongation, since the upper bounds of predicted change at these concentration levels were less than 10 msecs (5.8, 2.4, and 4.0 msecs, respectively). In the ASM, SM-AHN and MCL population, 25.4% of patients had at least one ECG measurement with a QTcF greater than 450 ms and 4.7% greater than 480 ms.
Clinical efficacy: AML: The efficacy and safety of midostaurin in combination with standard chemotherapy versus placebo plus standard chemotherapy and as single agent maintenance therapy was investigated in 717 patients (18 to 60 years of age) in a randomised, double-blind, phase III study. Patients with newly diagnosed FLT3-mutated AML as determined by a clinical study assay were randomised (1:1) to receive midostaurin 50 mg twice daily (n=360) or placebo (n=357) sequentially in combination with standard daunorubicin (60 mg/m2 daily on days 1-3) / cytarabine (200 mg/m2 daily on days 1-7) induction and high-dose cytarabine (3 g/m2 every 12 hours on days 1, 3, 5) consolidation, followed by continuous midostaurin or placebo treatment according to initial assignment for up to 12 additional cycles (28 days/cycle). While the study included patients with various AML-related cytogenetic abnormalities, patients with acute promyelocytic leukaemia (M3) or therapy-related AML were excluded. Patients were stratified by FLT3 mutation status: TKD, ITD with allelic ratio <0.7, and ITD with allelic ratio ≥0.7.
The two treatment groups were generally balanced with respect to the baseline demographics of disease characteristics. The median age of the patients was 47 years (range: 18 to 60 years), a majority of the patients had ECOG performance status of 0 or 1 (88.3%), and most patients had de novo AML (95%). Of the patients with race information reported, 88.1% were Caucasian. The majority of patients (77.4%) had FLT3-ITD mutations, most of them (47.6%) with a low allelic ratio (<0.7), and 22.6% of patients had FLT3-TKD mutations. Forty-eight per cent were male in the midostaurin arm and 41% in the placebo arm.
Patients who proceeded to haematopoietic stem cell transplant (SCT) stopped receiving study treatment prior to the start of the SCT conditioning regimen. The overall rate of SCT was 59.4% (214/360) of patients in the midostaurin plus standard chemotherapy arm versus 55.2% (197/357) in the placebo plus standard chemotherapy arm. All patients were followed for survival.
The primary endpoint of the study was overall survival (OS), measured from the date of randomisation until death by any cause. The primary analysis was conducted after a minimum follow-up of approximately 3.5 years after the randomisation of the last patient. The study demonstrated a statistically significant improvement in OS with a 23% risk reduction of death for midostaurin plus standard chemotherapy over placebo plus standard chemotherapy (see Table 2 and Figure 1). (See Figure 1.)
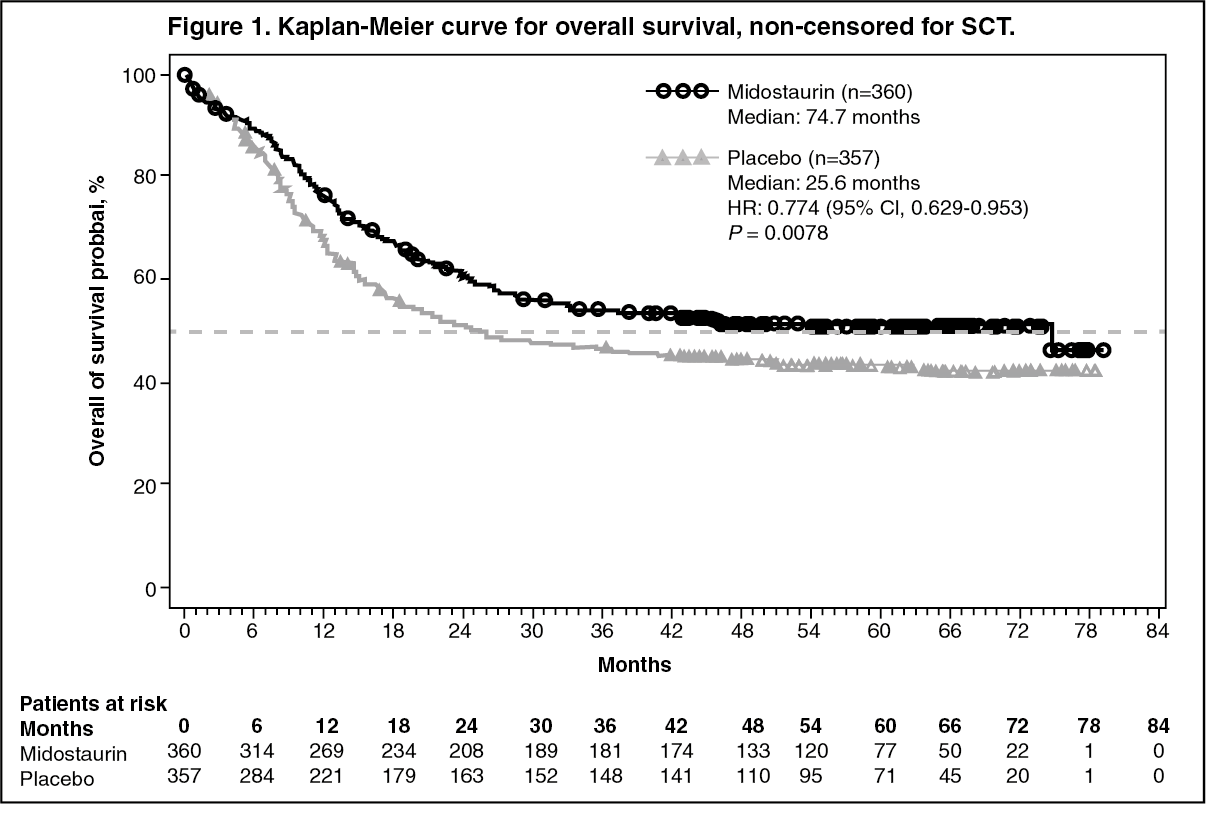 Click on icon to see table/diagram/image
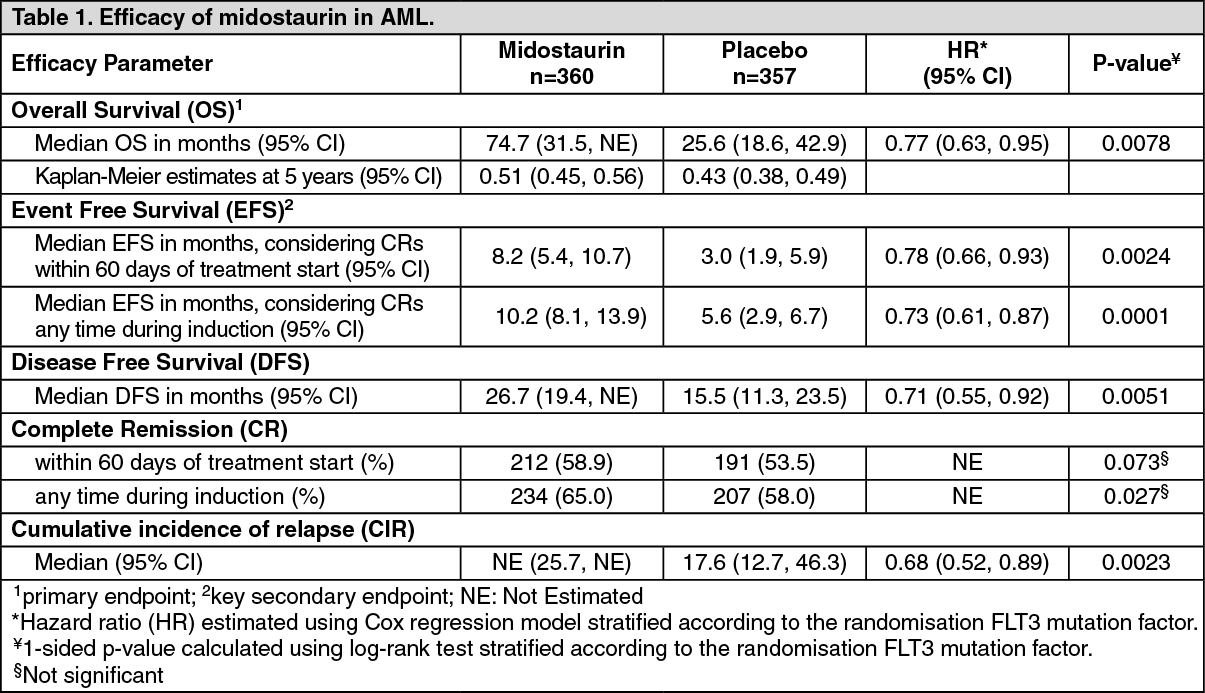
Click on icon to see table/diagram/imageThe key secondary endpoint was event-free survival (EFS; an EFS event is defined as a failure to obtain a complete remission (CR) within 60 days of initiation of protocol therapy, or relapse, or death from any cause). The EFS showed a statistically significant improvement for midostaurin plus standard chemotherapy over placebo plus standard chemotherapy (HR: 0.78 [95% CI, 0.66 to 0.93] p = 0.0024), and a median EFS of 8.2 months and 3.0 months, respectively; see Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThere was a trend favouring midostaurin for CR rate by day 60 for the midostaurin arm (58.9% versus 53.5%; P = 0.073) that continued when considering all CRs during induction (65.0% versus 58.0%; p = 0.027). In addition, in patients who achieved complete remission during induction, the cumulative incidence of relapse at 12 months was 26% in the midostaurin arm versus 41% in the placebo arm.
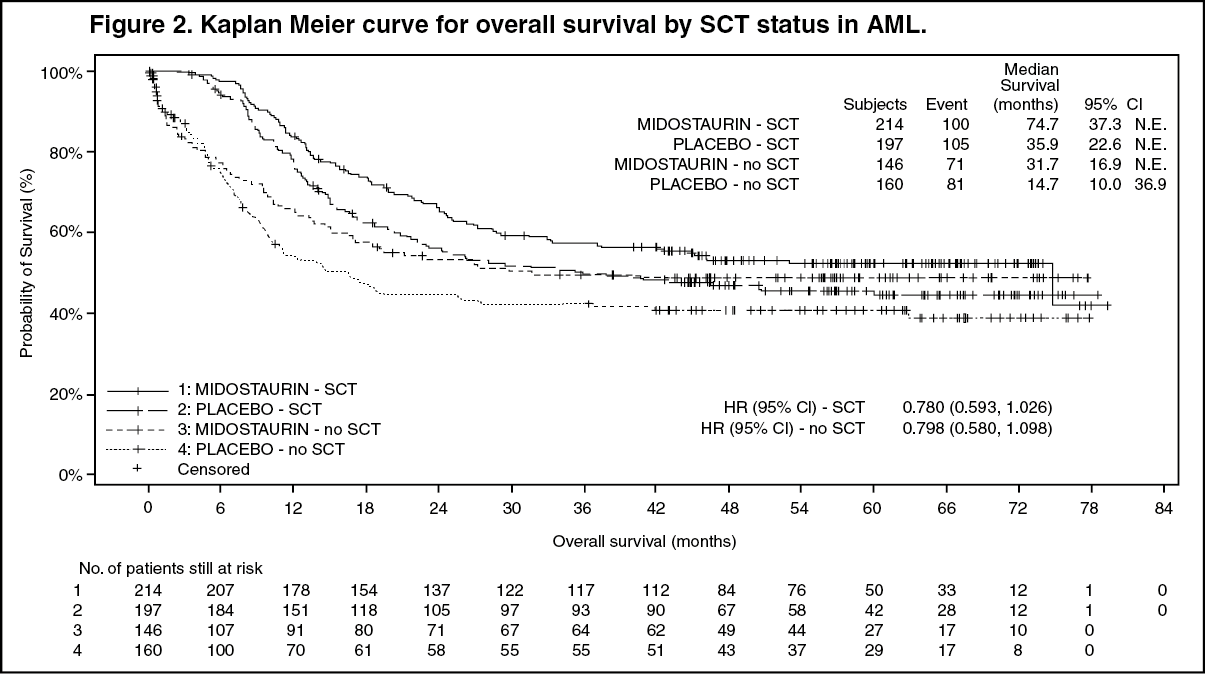
Sensitivity analyses for both OS and EFS when censored at the time of SCT also supported the clinical benefit with midostaurin plus standard chemotherapy over placebo.
Results for OS by SCT status are shown in Figure 2. For EFS, considering complete remissions within 60 days of study treatment start, the HR was 0.602 (95% CI: 0.372, 0.974) for patients with SCT and 0.827 (95% CI: 0.689, 0.993) for patients without SCT, favouring midostaurin. (See Figure 2.)
 Click on icon to see table/diagram/image
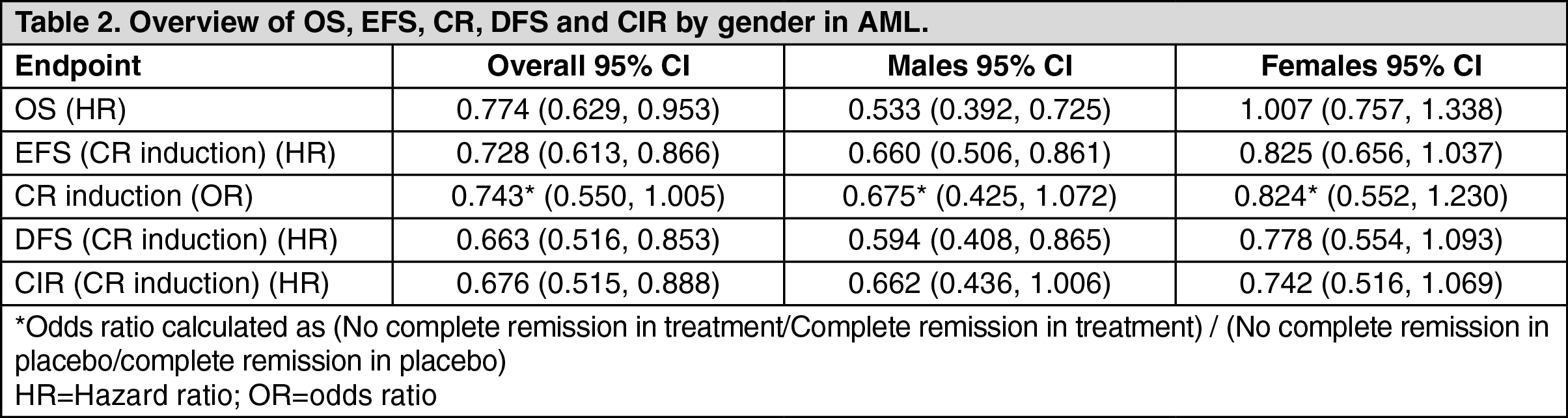
Click on icon to see table/diagram/imageIn a subgroup analysis, no apparent OS benefit was observed in females, however, a treatment benefit was observed in females in all secondary efficacy endpoints (see Table 2).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageEfficacy and safety in patients 60-70 years old were evaluated in a phase II, single-arm, investigator-initiated study of midostaurin in combination with intensive induction, consolidation including allogenic SCT and single-agent maintenance in patients with FLT3-ITD mutated AML. Based on an interim analysis, the EFS rate at 2 years (primary endpoint) was 27.1% (95% CI: 16.6, 44.1) and the median OS was 15.5 months in patients older than 60 years of age (46 out of 145 patients).
ASM, SM-AHN and MCL: The efficacy of midostaurin in patients with ASM, SM-AHN and MCL, collectively referred to as advanced systemic mastocytosis (SM), was evaluated in two open-label, single-arm, multicentre studies (142 patients in total).
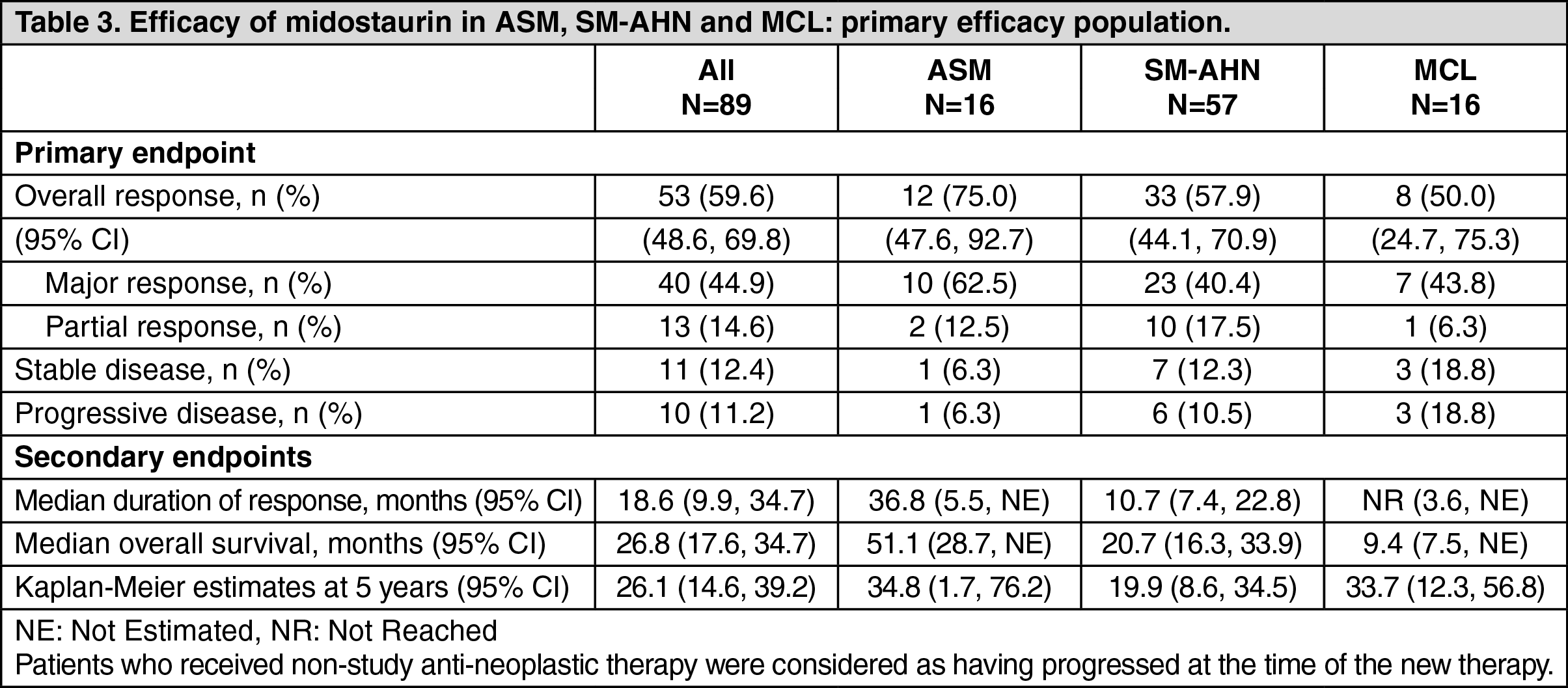
The pivotal study was a multicentre, single-arm phase II study in 116 patients with advanced SM (Study CPKC412D2201). Midostaurin was administered orally at 100 mg twice daily until disease progression or intolerable toxicity. Of the 116 patients enrolled, 89 were considered eligible for response assessment and constituted the primary efficacy population. Of these, 73 patients had ASM (57 with an AHN) and 16 patients had MCL (6 with an AHN). The median age in the primary efficacy population was 64 years with approximately half of the patients ≥65 years. Approximately one third (36%) received prior anti-neoplastic therapy for ASM, SM-AHN or MCL. At baseline in the primary efficacy population, 65% of the patients had >1 measurable C finding (thrombocytopenia, hypoalbuminaemia, anaemia, high total bilirubin, transfusion-dependent anaemia, weight loss, neutropenia, high ALT or high AST). The KIT D816V mutation was detected in 82% of patients.
The primary endpoint was overall response rate (ORR). Response rates were assessed based on the modified Valent and Cheson criteria and responses were adjudicated by a study steering committee. Secondary endpoints included duration of response, time to response, and overall survival. Responses to midostaurin are shown in Table 3. Activity was observed regardless of number of prior therapies, and presence or absence of an AHN. Confirmed responses were observed in both KIT D816V mutation positive patients (ORR=63%) and KIT D816V wild type or unknown patients (ORR=43.8%). However, the median survival for KIT D816V positive patients was longer, i.e. 33.9 months (95% CI: 20.7, 42), than for KIT D816V wild type or unknown patients, i.e. 10 months (95% CI: 6.9, 17.4). Forty-six percent of patients had a decrease in bone marrow infiltration that exceeded 50% and 58% had a decrease in serum tryptase levels that exceeded 50%. Spleen volume decreased by ≥10% in 68.9% of patients with at least 1 post-baseline assessment (26.7% of patients had a reduction of ≥35%, which correlates with a 50% decrease by palpation).
The median time to response was 0.3 months (range: 0.1 to 3.7 months). The median duration of follow-up was 43 months. (See Table 3.)
 Click on icon to see table/diagram/image
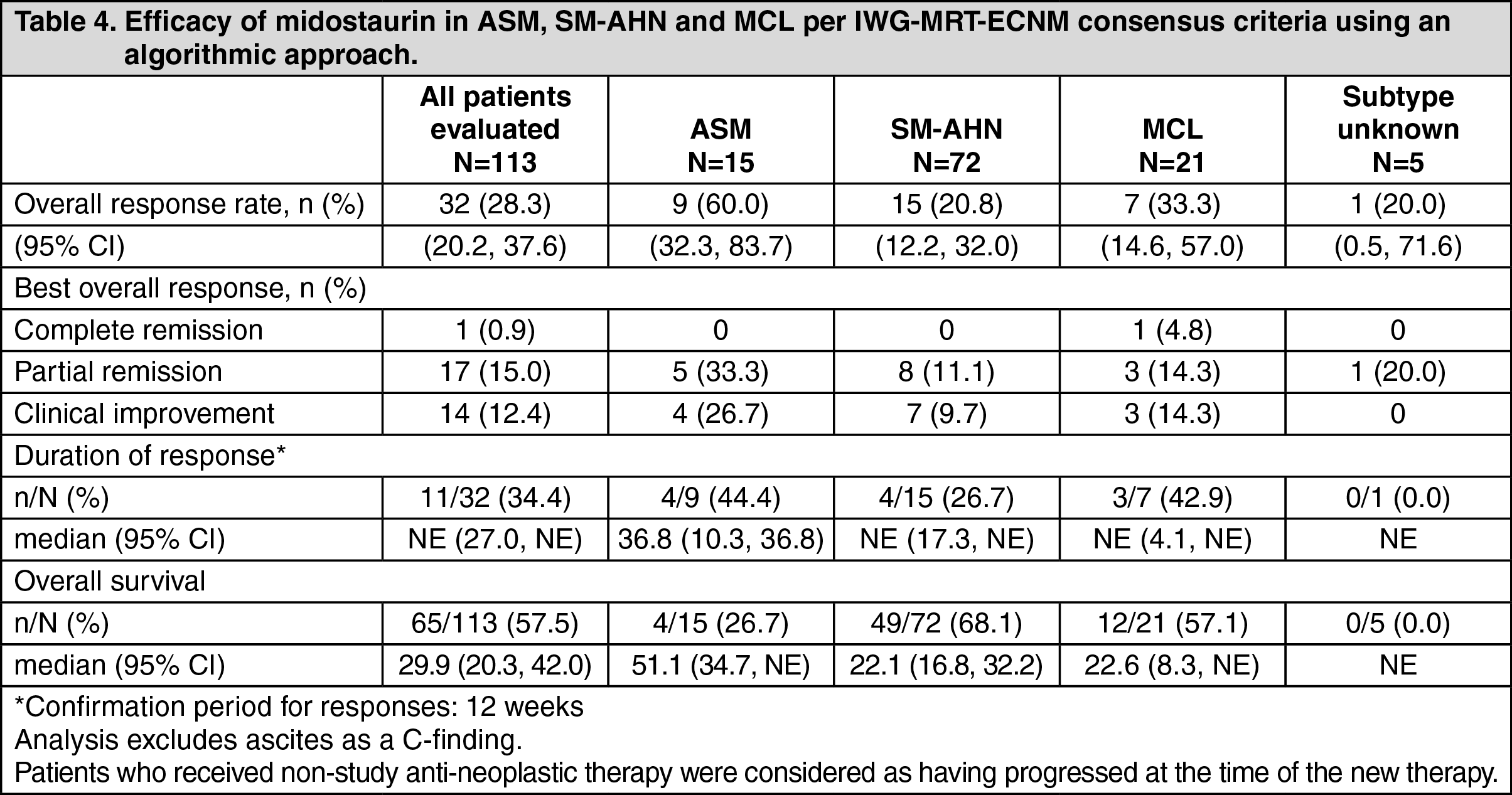
Click on icon to see table/diagram/imageAlthough the study was designed to be assessed with the modified Valent and Cheson criteria, as a post-hoc exploratory analysis, efficacy was also assessed per the 2013 International Working Group - Myeloproliferative Neoplasms Research and Treatment - European Competence Network on Mastocytosis (IWG-MRT-ECNM) consensus criteria. Response to Rydapt was determined using a computational algorithm applied without any adjudication. Out of 116 patients, 113 had a C-finding as defined by IWG response criteria (excluding ascites as a C-finding). All responses were considered and required a 12-week confirmation (see Table 4).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe supportive study was a single-arm, multicentre, open-label phase II study of 26 patients with ASM, SM-AHN and MCL (CPKC412A2213). Midostaurin was administered orally at 100 mg twice daily in cycles of 28 days. Lack of a major response (MR) or partial response (PR) by the end of the second cycle required discontinuation from the study treatment. Twenty (76.9%) patients had ASM (17 [85%] with AHN) and 6 patients (23.1%) had MCL (2 [33.3%] with AHN). The median age was 64.5 years with half of the patients ≥65 years). At baseline, 88.5% had >1 C finding and 69.2% had received at least one prior anti-neoplastic regimen.
The primary endpoint was ORR evaluated by the Valent criteria during the first two cycles of treatment. Nineteen patients (73.1%; 95% CI = [52.2, 88.4]) achieved a response during the first two cycles of treatment (13 MR; 6 PR). The median duration of follow-up was 73 months, and the median duration of response has not been reached. Median overall survival was 40.0 months (patients were only followed up for one year after treatment discontinuation for survival).
Paediatric population: The European Medicines Agency has waived the obligation to submit the results of studies with Rydapt in all subsets of the paediatric population in the treatment of malignant mastocytosis and mast cell leukaemia (see Dosage & Administration for information on paediatric use).
The European Medicines Agency has deferred the obligation to submit the results of studies with Rydapt in one or more subsets of the paediatric population in the treatment of acute myeloid leukaemia (see Dosage & Administration for information on paediatric use).
Pharmacokinetics: Midostaurin is a compound with good absorption and poor solubility. Two of its metabolites demonstrated pharmacological activities (CGP52421 and CGP62221). Following multiple doses, the pharmacokinetics of midostaurin and CGP62221 were time-dependent, with an initial increase observed in the first week followed by a decline of concentrations until reaching steady state on day 28. CGP52421 concentrations do not appear to decline as significantly as for midostaurin and CGP62221.
Absorption: The absolute bioavailability of midostaurin following oral administration is not known.
In humans, the absorption of midostaurin was rapid after oral administration, with Tmax of total radioactivity observed at 1-3 hours post dose. The population pharmacokinetic analysis indicated that the absorption in patients was less than dose proportional at doses >50 mg twice daily.
In healthy subjects, after administration of a single dose of 50 mg midostaurin with food, AUC of midostaurin was increased to 20800 ng*h/ml and Cmax was decreased to 963 ng/ml (see Interactions). Similarly, for CGP52421 and CGP62221 AUC increased to 19000 and 29200 ng*h/ml and Cmax decreased to 172 and 455 ng/ml, respectively. Time to peak concentration was also delayed in the presence of a high-fat meal. Tmax was delayed for all entities, midostaurin median Tmax was 3 h, and for CGP52421 and CGP62221 Tmax was delayed to 6 and 7 hours respectively.
In clinical studies, the efficacy and safety of Rydapt were investigated following administration with a light meal. After oral administration of a single 100 mg dose of midostaurin under fed conditions in ASM, SM-AHN and MCL patients, AUCinf, Cmax and Tmax were 49600 ng*h/ml, 2940 ng/ml and 3 h, respectively, for midostaurin. For CGP52421, AUC0-12h and Cmax were 2770 ng*h/ml and 299 ng/ml, respectively. AUC0-12h and Cmax for CGP62221 were 8700 ng*h/ml and 931 ng/ml, respectively. After 100 mg bid multiple oral doses of midostaurin the Cmin,ss plasma midostaurin in AML and ASM, SM-AHN, MCL patients were 919 and 1060 ng/ml, respectively. The CGP62221 Cmin,ss in the AML and the ASM, SM-AHN, MCL population were 1610 ng/ml and 2020 ng/ml, respectively. The CGP52421, Cmin,ss in the AML and the ASM, SM-AHN, MCL population were 8630 ng/ml and 2860 ng/ml, respectively.
Distribution: Midostaurin has a tissue distribution of geometric mean of 95.2 l (Vz/F). Midostaurin and its metabolites are distributed mainly in plasma rather than red blood cells. In vitro data showed midostaurin is more than 98% bound to plasma proteins, such as albumin, α1-acid glycoprotein (AGP) and lipoprotein.
Biotransformation: Midostaurin is metabolised by CYP3A4 mainly via oxidative pathways. The major plasma components included midostaurin and two major active metabolites, CGP62221 (via O-demethylation) and CGP52421 (via hydroxylation), accounting for 27.7±2.7% and 38.0±6.6%, respectively, of the total plasma exposure at 96 hours after a single 50 mg dose of midostaurin.
Elimination: The median terminal half-lives of midostaurin, CGP62221 and CGP52421 in plasma are approximately 20.5, 32.3 and 482 hours. The mean apparent plasma clearance (CL/F) was 2.4-3.1 l/h in healthy subjects. In AML and ASM, SM-AHN and MCL patients, population pharmacokinetic estimates for clearance of midostaurin at steady state were 5.9 l/h and 4.4 l/h, respectively. The Human Mass Balance study results indicated that faecal excretion is the major route of excretion (78% of the dose), and mostly as metabolites (73% of the dose), while unchanged midostaurin accounts for 3% of the dose. Only 4% of the dose is recovered in urine.
Linearity/non-linearity: In general, midostaurin and its metabolites showed no major deviation from dose-proportionality after a single dose in the range of 25 mg to 100 mg. However, there was a less than dose-proportional increase in exposure after multiple doses within the dose range of 50 mg to 225 mg daily.
Following multiple oral doses, midostaurin displayed time-dependent pharmacokinetics with an initial increase in plasma concentrations during the first week (peak Cmin) followed by a decline with time to a steady-state after approximately 28 days (2.5-fold decrease). While the exact mechanism for the declining concentration of midostaurin is unclear, it is likely due to the auto-induction properties of midostaurin and its two active metabolite CGP52421 and CGP62221 on CYP3A4. The pharmacokinetics of the CGP62221 metabolite showed a similar trend. However, CGP52421 concentrations increased up to 2.5-fold for ASM, SM-AHN and MCL and up to 9-fold for AML, compared to midostaurin after one month of treatment.
In vitro evaluation of drug-drug interaction potential: Enzyme drug-drug interactions: Cytochrome P450 inhibition: Based on in vitro data, midostaurin and its active metabolites, CGP52421 and CGP62221, are considered inhibitors and may potentially cause increases in exposure of co-administered medicinal products primarily cleared by CYP1A2, CYP2D6, CYP2C8, CYP2C9, CYP2E1 and CYP3A4/5. In addition, a time-dependent inhibition of CYP3A4/5 by midostaurin, CGP52421 and CGP62221 was also observed in vitro.
Cytochrome P450 induction: Based on in vitro data, midostaurin and its active metabolites, CGP52421 and CGP62221, are also considered inducers and may cause decreases in exposure of co-administered medicinal products primarily cleared by CYP1A2, CYP2B6, CYP2C8, CYP2C9, CYP2C19 and CYP3A4 (see Interactions).
Transporter drug-drug interactions: In vitro experiments demonstrated that midostaurin, CGP52421 and CPG62221 can potentially inhibit P-gp, BCRP and OATP1B1.
Special populations: Elderly patients: Based on population pharmacokinetic analyses no significant impact of age on the pharmacokinetics of midostaurin and its two active metabolites was identified for patients aged between 65 and 85 years. In adult patients with ASM, SM-AHN and MCL or AML, no midostaurin dose adjustment is required based on age.
Paediatric patients: Rydapt is not recommended to be used in children and adolescents (see Dosage & Administration). The pharmacokinetics of midostaurin in paediatric patients were explored in a phase I dose escalation monotherapy study with 22 patients (12 aged 0-2 years and 10 aged 10-17 years) with AML or MLL-rearranged ALL using a population pharmacokinetic approach. The pharmacokinetics of midostaurin were less than dose proportional with the doses of 30 mg/m2 and 60 mg/m2 after single and multiple doses. Due to the limited pharmacokinetic data in paediatric patients, no comparison with midostaurin pharmacokinetics in adults can be made.
Gender: Based on population pharmacokinetic model analyses of the effect of gender on clearance of midostaurin and its active metabolites, there was no statistically significant finding and the anticipated changes in exposure (<20%) were not deemed to be clinically relevant. No midostaurin dose adjustment is required based on gender.
Race/ethnicity: There are no differences in the pharmacokinetic profile between Caucasian and Black subjects. Based on a phase I study in healthy Japanese volunteers, pharmacokinetic profiles of midostaurin and its metabolites (CGP62221 and CGP52421) are similar compared to those observed in other pharmacokinetic studies conducted in Caucasians and Blacks. No midostaurin dose adjustment is required based on ethnicity.
Hepatic impairment: A dedicated hepatic impairment study assessed the systemic exposure of midostaurin after oral administration of 50 mg twice daily for 6 days in subjects with baseline mild or moderate hepatic impairment (Child-Pugh Class A or B, respectively) and control subjects with normal hepatic function. The maximum concentration was reached between 2 and 3 hours after administration after single or repeated doses for all groups. On day 1, the AUC0-12 and Cmax were 8130 ng*h/ml and 1206 ng/ml, respectively, for healthy subjects. AUC0-12 was decreased by 39% and 36% in subjects with mild and moderate hepatic impairment, respectively. On day 7, AUCCtrough (exposure under the curve of Ctrough from day 1 to day 7) was 5410 ng*h/ml in healthy subjects and was decreased by 35% and 20% in subjects with mild and moderate hepatic impairment, respectively. AUCtau was decreased by 28% and 20% on day 7, respectively. Finally, the long-term data from patients were analysed using a population pharmacokinetic approach. No impact of hepatic impairment could be identified in patients with mild or moderate hepatic impairment in the ASM, SM-AHN, MCL and AML populations.
Overall, there was no clinically relevant increase in exposure (AUC) to plasma midostaurin in subjects with mild or moderate hepatic impairment compared to subjects with normal hepatic function. No dosage adjustment is necessary for patients with baseline mild or moderate hepatic impairment. The pharmacokinetics of midostaurin have not been assessed in patients with baseline severe hepatic impairment (Child-Pugh Class C) (see Precautions).
Renal impairment: Renal elimination is a minor route of elimination for midostaurin. No dedicated renal impairment study was conducted for midostaurin. Population pharmacokinetic analyses were conducted using data from clinical studies in patients with AML (n=180) and ASM, SM-AHN and MCL (n=141). Out of the 321 patients included, 177 patients showed pre-existing mild (n=113), moderate (n=60) or severe (n=4) renal impairment (15 ml/min ≤ creatinine clearance [CrCL] <90 ml/min). 144 patients showed normal renal function (CrCL >90 ml/min) at baseline. Based on the population pharmacokinetic analyses, midostaurin clearance was not significantly impacted by renal impairment and therefore no dosage adjustment is necessary for patients with mild or moderate renal impairment.
Toxicology: Preclinical safety data: Due to dose-limiting toxicity, clinical therapeutic exposure levels could not be reached in animals. All animal findings described below were observed at midostaurin exposure significantly lower than therapeutic levels.
Safety pharmacology and single/repeat dose toxicity: Safety pharmacology studies indicate that midostaurin is unlikely to interfere with vital functions of the central nervous system. In vitro, midostaurin did not inhibit hERG channel activity up to the limit of solubility of 12 μM. The two major human metabolites GGP52421 and CGP62221 (also tested at the limit of solubility) inhibited hERG current with moderate safety margins. In the repeat-dose studies in dogs, a decrease in heart rate, prolongation of the P-Q interval, and sporadically occurring atrioventricular blocks were seen in individual animals.
In the repeat-dose studies, target organs for toxicity were the gastrointestinal tract (emesis in dogs and monkeys, diarrhoea and mucosal alteration), testes (decreased spermatogenesis), bone marrow (hypocellularity) and lymphoid organs (depletion/atrophy). The effect on the bone marrow and lymphoid organs was accompanied by haematological changes of decreased white blood cells, lymphocytes and erythrocytic parameters. An increase in liver enzymes (ALT and AST) was seen consistently in rats, and in dogs and monkeys in long-term studies of ≥3 months duration, without histopathological correlates.
Reproductive toxicity: In a fertility study in rats, midostaurin was associated with reduced fertility, testicular degeneration and atrophy, reduced sperm motility, oligo- and aspermia, increased resorptions, decreased pregnancy rate, number of implants and live embryos.
In embryo-foetal development studies in rats and rabbits, increased numbers of late resorptions, reduced foetal weight and reduced skeletal ossification were observed.
In a pre- and post-natal developmental study, maternal dystocia and reduced litter size, lower pup body weights, delay in eye opening and auricular startle ontogeny were noted.
Juvenile animal studies: In a toxicity study in juvenile rats, midostaurin was administered from days 7 to 70 postpartum. A reduction in body weight, haemorrhage and mixed cell infiltration in the lungs, and erythrocytosis/erythrophagocytosis in the mesenteric lymph nodes were seen. There were no effects on physical development, sensory function or behavioural function. Mating index, fertility index and conception rates were reduced at 0, 5 and 15 mg/kg/day, but not at 2 mg/kg/day.
Genotoxicity: In vitro and in vivo genotoxicity studies covering relevant genotoxicity endpoints showed no evidence of mutagenic or clastogenic activity. No carcinogenicity studies have been performed.
Environmental Risk Assessment (ERA): Environmental risk assessment studies have shown that midostaurin has the potential to be persistent, bioaccumulative and toxic to the environment.