


 Sign Out
Sign Out
Pharmacology: Pharmacodynamics: Mechanism of action: Spesolimab is a humanised antagonistic monoclonal immunoglobulin G1 (IgG1) antibody blocking human IL36R signalling. Binding of spesolimab to IL36R prevents the subsequent activation of IL36R by cognate ligands (IL36 α, β and γ) and downstream activation of pro-inflammatory pathways.
Pharmacodynamic effects: Following treatment with spesolimab in patients with GPP, reduced levels of C-reactive protein (CRP), IL6, T helper cell (Th1/Th17) mediated cytokines, keratinocyte-mediated inflammation, neutrophilic mediators, and proinflammatory cytokines were observed in serum and skin at week 1 compared to baseline and was associated with a decrease in clinical severity. These reductions in biomarkers became more pronounced at the last measurement at week 8 in Effisayil 1.
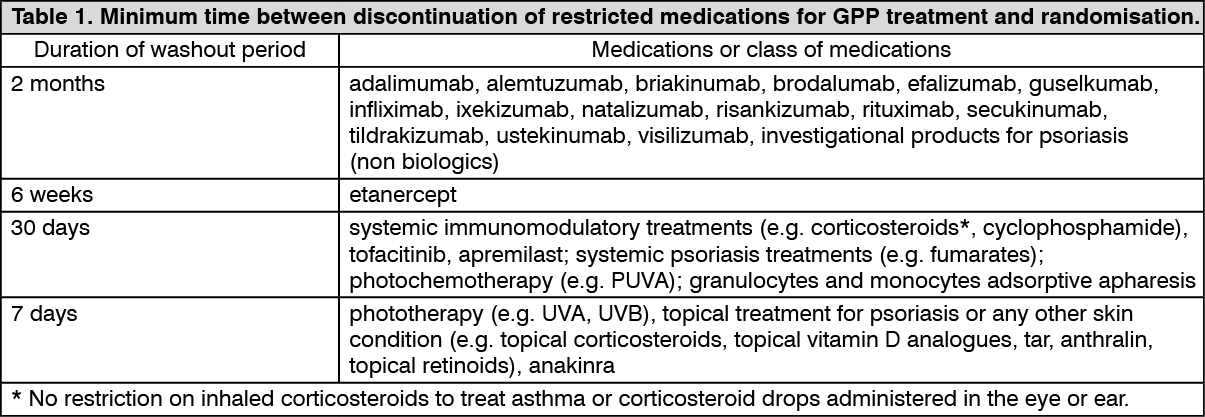
Clinical efficacy and safety: Effisayil 1 (1368-0013): A randomised, double-blind, placebo-controlled study (Effisayil 1) was conducted to evaluate the clinical efficacy and safety of spesolimab in adult patients with flares of Generalised Pustular Psoriasis (GPP), as diagnosed per European Rare And Severe Psoriasis Expert Network (ERASPEN) criteria, regardless of IL36RN mutation status. Patients were randomised if they had a flare of GPP of moderate-to-severe intensity, as defined by a Generalised Pustular Psoriasis Physician Global Assessment (GPPGA) total score (which ranges from 0 [clear] to 4 [severe]) of at least 3 (moderate), presence of fresh pustules (new appearance or worsening of pustules), GPPGA pustulation sub score of at least 2 (mild), and at least 5% of body surface area covered with erythema and the presence of pustules. Patients were required to discontinue systemic and topical therapy for GPP prior to randomisation (see Table 1). Patients with an immediate life-threatening flare of GPP or requiring intensive care treatment were excluded from the study. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe primary endpoint of the study was the proportion of patients with a GPPGA pustulation sub score of 0 (indicating no visible pustules) at week 1 after treatment. The key secondary endpoint of the study was the proportion of patients with a GPPGA total score of 0 or 1 (clear or almost clear skin) at week 1. For the GPPGA pustulation sub score of 0, the GPPGA total score of 0/1 and the GPPASI 75, non-responder imputation was used to handle the occurrence of escape (treatment at the investigator's choice if the disease worsened) and rescue (single 900 mg dose of intravenous spesolimab) medication use and missing data.
A total of 53 patients were randomised (2:1) to receive a single intravenous dose of 900 mg spesolimab (n = 35) or placebo (n = 18). Patients in either treatment arm who still experienced flare symptoms at week 1 were eligible to receive a single intravenous dose of open-label 900 mg spesolimab, resulting in 12 patients (34%) in the spesolimab arm receiving a second dose of spesolimab and 15 patients (83%) in the placebo arm receiving one dose of spesolimab on day 8. In addition, 6 patients (4 spesolimab arm; 2 placebo arm) received rescue treatment with a single 900 mg dose of intravenous spesolimab for reoccurrence of a flare after day 8.
The study population consisted of 32% men and 68% women. The mean age was 43 (range: 21 to 69) years; 55% of patients were Caucasian and 45% were Asian. Most patients included in the study had a GPPGA pustulation sub score of 3 (43%) or 4 (36%), and patients had a GPPGA total score of 3 (81%) or 4 (19%). 24.5% of patients had been previously treated with biologic therapy for GPP.
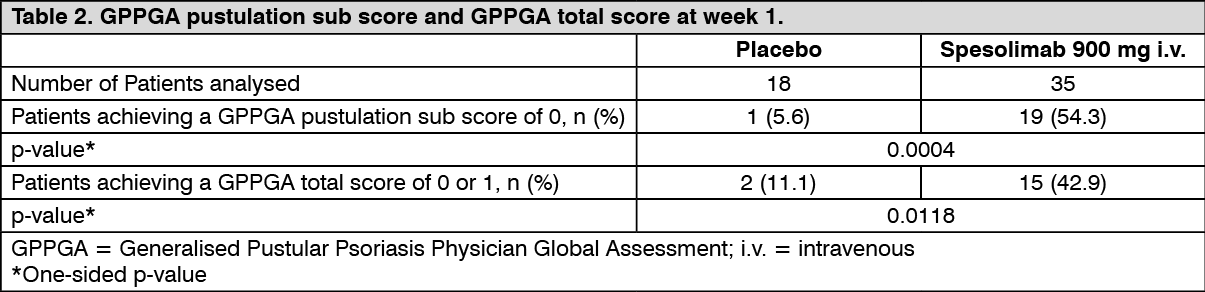
Primary and key secondary efficacy: At week 1, there was a statistically significant difference in the proportion of patients achieving a GPPGA pustulation sub score of 0 (indicating no visible pustules) and GPPGA total score of 0 or 1 (clear or almost clear skin) in the spesolimab arm compared with placebo (see Table 2).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageFor both the primary and the key secondary endpoint, treatment effect was observed for all patients regardless of the IL36RN mutation status.
Paediatric population: See Dosage & Administration for information on paediatric use.
Pharmacokinetics: A population pharmacokinetic model was developed based on data collected from healthy subjects, patients with GPP and patients with other diseases. After a single intravenous dose of 900 mg, the population PK model-estimated AUC0-∞ (95% CI) and Cmax (95% CI) in a typical ADA-negative patient with GPP were 4,750 (4,510, 4,970) μg·day/mL and 238 (218, 256) μg/mL, respectively. In some patients with ADA titer values > 4,000, plasma spesolimab concentrations were reduced, with no apparent impact on pharmacokinetics at ADA titers below 4,000 (see Adverse Reactions).
Distribution: Based on the population pharmacokinetic analysis, the typical volume of distribution at steady state was 6.4 L.
Biotransformation: The metabolic pathway of spesolimab has not been characterised. As a humanised IgG1 monoclonal antibody, spesolimab is expected to be degraded into small peptides and amino acids via catabolic pathways in a manner similar to endogenous IgG.
Elimination: In the linear dose range (0.3-20 mg/kg), based on the population PK model, spesolimab clearance (95% CI) in a typical ADA-negative patient with GPP, weighing 70 kg was 0.184 L/day. The terminal-half-life was 25.5 days. Clearance of spesolimab was increased in some patients with ADA titer values > 4,000.
Linearity/non-linearity: At low doses, spesolimab exhibited target-mediated drug disposition (TMDD) kinetics after single intravenous dose administration. At doses from 0.01 to 0.3 mg/kg, both clearance (CL) and terminal half-life were dose dependent, and systemic exposure (AUC) increased more than dose proportionally with dose. The saturation of the nonlinear elimination pathway occurred at about 0.3 mg/kg as spesolimab AUC increased approximately linearly with dose from 0.3 to 20 mg/kg, and CL and terminal half-life were independent of dose.
Body weight: Spesolimab concentrations were lower in subjects with higher body weight. The impact of body weight on spesolimab exposure is not expected to be clinically meaningful up to approximately 130 kg. The clinical relevance of higher body weight greater than 130 kg is unknown.
Elderly / gender / race: Based on population pharmacokinetic analyses, age, gender and race do not have an effect on the pharmacokinetics of spesolimab.
Hepatic and renal impairment: As a monoclonal antibody, spesolimab is not expected to undergo hepatic or renal elimination. No formal trial of the effect of hepatic or renal impairment on the pharmacokinetics of spesolimab was conducted.
Population PK analysis did not identify mild hepatic impairment or mild or moderate renal impairment as having an influence on the systemic exposure of spesolimab.
Paediatric population: The pharmacokinetics of spesolimab in paediatric patients has not yet been studied.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on repeated dose toxicity studies.
Developmental and reproductive toxicity: Non-clinical studies conducted in mice using a surrogate antibody directed towards murine IL36R do not indicate direct or indirect harmful effects with respect to pregnancy, embryonic/foetal development or fertility.
Genotoxicity: Genotoxicity studies have not been conducted with spesolimab.
Carcinogenicity: Carcinogenicity and mutagenicity studies have not been conducted with spesolimab.