Tafluprost, timolol (as maleate).
One mL solution contains: tafluprost 15 micrograms and timolol (as maleate) 5 mg.
A clear, colourless solution with a pH of 6.0-6.7 and an osmolality of 290-370 mOsm/kg.
Excipients/Inactive Ingredients: Glycerol, Disodium phosphate dodecahydrate, Disodium edetate, Polysorbate 80, Hydrochloric acid and/or sodium hydroxide for pH adjustment, Water for injections.
Pharmacotherapeutic group: Antiglaucoma preparations and miotics, beta blocking agents. ATC code: S01ED51.
Pharmacology: Pharmacodynamics: Mechanism of action: Tapcom-S is a fixed combination of two active substances tafluprost and timolol. These two active substances lower intraocular pressure (IOP) by complementary mechanisms of action and the combined effect results in additional IOP reduction compared to either compound alone.
Tafluprost is a fluorinated analogue of prostaglandin F2α. Tafluprost acid, the biologically active metabolite of tafluprost, is a highly potent and selective agonist of the human prostanoid FP receptor.
Pharmacodynamic studies in monkeys indicate that tafluprost reduces intraocular pressure by increasing the uveoscleral outflow of aqueous humour.
Timolol maleate is a non-selective beta-adrenergic receptor blocking agent. The precise mechanism of action of timolol maleate in lowering intraocular pressure is not clearly established at this time, although a fluorescein study and tonography studies indicate that the predominant action may be related to reduced aqueous formation. However, in some studies a slight increase in outflow facility was also observed.
Clinical efficacy: In a 6-month study (n=400) in patients with open-angle glaucoma or ocular hypertension and mean untreated IOPs between 24-26 mmHg, the IOP lowering effect of Tapcom-S (once daily in the morning) was compared to concomitant administration of 0.0015% tafluprost (once daily in the morning) and 0.5% timolol (twice daily). Tapcom-S was non-inferior to the effect of concomitantly used 0.0015% tafluprost and 0.5% timolol at all time points and visits with the generally used non-inferiority margin of 1.5 mmHg. The mean diurnal IOP decrease from baseline was 8 mmHg in both arms at the primary endpoint of 6 months (decreases ranging between 7 to 9 mmHg in both arms at the different time points during the day over the study visits).
Another 6-month study (n=564) compared Tapcom-S with the respective monotherapies in patients with open-angle glaucoma or ocular hypertension and mean untreated IOPs between 26-27 mmHg. Patients insufficiently controlled either with 0.0015% tafluprost (IOP 20 mmHg or greater on treatment) or 0.5% timolol (IOP 22 mmHg or greater on treatment) were randomized to be treated with Tapcom-S or the same monotherapy. The mean diurnal IOP reduction of Tapcom-S was statistically superior to that of tafluprost given once daily in the morning or timolol given twice daily, at visits 6 weeks, 3 months (primary efficacy endpoint) and 6 months. The mean diurnal IOP decrease from baseline of Tapcom-S at 3 months was 9 mmHg, in comparison to 7 mmHg observed for both monotherapies. IOP decreases with Tapcom-S at the different time points during the day over the visits ranged between 8 to 9 mmHg in the tafluprost monotherapy comparison group and between 7 to 9 mmHg in the timolol monotherapy comparison group.
Combined data from Tapcom-S patients with high baseline IOP of 26 mmHg (mean diurnal) or above in these two pivotal studies (n=168) showed that the mean diurnal reduction in the IOP was 10 mmHg at the primary end point (3 or 6 months) ranging between 9 and 12 mmHg at the different time points during the day.
Pharmacokinetics: Absorption: Plasma concentrations of tafluprost acid and timolol were investigated in healthy volunteers after single and repeated ocular dosing for eight days of Tapcom-S (once daily), 0.0015% tafluprost (once daily) and 0.5% timolol (twice daily). Tafluprost acid plasma concentrations peaked at 10 minutes after dosing and declined below the lower limit of detection (10 pg/ml) before 30 minutes after Tapcom-S dosing. Accumulation of tafluprost acid was negligible and the tafluprost acid mean AUC0-last (monotherapy: 4.45±2.57 pg·h/ml; Tapcom-S: 3.60±3.70 pg·h/ml) and the mean Cmax (monotherapy: 23.9±11.8 pg/ml; Tapcom-S: 18.7±11.9 pg/ml) were both slightly lower with Tapcom-S as compared to tafluprost monotherapy on Day 8. Timolol plasma concentrations peaked at median Tmax values of 15 and 37.5 minutes after Tapcom-S dosing on Days 1 and 8, respectively. The Day 8 timolol mean AUC0-last (monotherapy: 5750±2440 pg·h/ml; Tapcom-S: 4560±2980 pg·h/ml) and the mean Cmax (monotherapy: 1100±550 pg/ml; Tapcom-S: 840±520 pg/ml) were both somewhat lower with Tapcom-S compared to timolol monotherapy. The lower plasma timolol exposure with Tapcom-S appears to be due to once-daily dosing for Tapcom-S versus twice daily dosing with timolol monotherapy.
Tafluprost and timolol are absorbed through the cornea. In rabbits, corneal penetration of tafluprost from Tapcom-S was similar to that of tafluprost monopreparation after a single instillation while the penetration of timolol was slightly less from the Tapcom-S compared to timolol monopreparation. For tafluprost acid, AUC4h was 7.5 ng·h/ml following administration of Tapcom-S and 7.7 ng·h/ml following administration of tafluprost monopreparation. For timolol, AUC4h was 585 ng·h/ml and 737 ng·h/ml following administration of Tapcom-S and timolol monopreparation, respectively. Tmax for tafluprost acid was 60 minutes for both Tapcom-S and tafluprost monopreparation, while for timolol Tmax was 60 minutes for Tapcom-S and 30 minutes for timolol monopreparation.
Distribution: Tafluprost: In monkeys, there was no specific distribution of radiolabelled tafluprost in the iris-ciliary body or choroid including retinal pigment epithelium, which suggested low affinity for melanin pigment. In a whole body autoradiography study in rats, the highest concentration of radioactivity was observed in the cornea followed by the eyelids, sclera and the iris. Outside the eye radioactivity was distributed to the lacrimal apparatus, palate, oesophagus and gastrointestinal tract, kidney, liver, gall bladder and urinary bladder. The binding of tafluprost acid to human serum albumin in vitro was 99% at 500 ng/ml tafluprost acid.
Timolol: The peak level of timolol-related radioactivity in the aqueous humour was reached after 30 minutes following a single application of 3H-radiolabelled timolol (0.5% solution: 20 μl/eye) to both eyes in rabbits. Timolol is eliminated from the aqueous humour much faster than from the pigmented tissues iris and ciliary body.
Biotransformation: Tafluprost: The principal metabolic pathway of tafluprost in human, which was tested in vitro, is the hydrolysis to the pharmacologically active metabolite, tafluprost acid, which is further metabolized by glucuronidation or beta-oxidation. Products of beta-oxidation, 1,2-dinor and 1,2,3,4-tetranor tafluprost acids, which are pharmacologically inactive, may be glucuronidated or hydroxylated. Cytochrome P450 (CYP) enzyme system is not involved in the metabolism of tafluprost acid. Based on the study in rabbit corneal tissue and with purified enzymes, the main esterase responsible for the ester hydrolysis to tafluprost acid is carboxyl esterase. Butylcholine esterase but not acetylcholine esterase may also contribute to the hydrolysis.
Timolol: Timolol is metabolized in the liver primarily by CYP2D6 enzyme into inactive metabolites, which are excreted primarily through the kidneys.
Elimination: Tafluprost: Following once daily administration of 3H-tafluprost (0.005% ophthalmic solution; 5 μl/eye) for 21 days to both eyes in rats, approximately 87% of the total radioactive dose was recovered in the excreta. Percent of the total dose excreted in urine was approximately 27-38% and approximately 44-58% of the dose was excreted in the faeces.
Timolol: Apparent elimination half-life from the human plasma is about 4 hours. Timolol is extensively metabolised in the liver and the metabolites are excreted in the urine in addition to 20% unchanged timolol following oral administration.
Toxicology: Preclinical safety data: Tapcom-S: Non-clinical data reveal no special hazard for humans based on repeated dose toxicity study and ocular pharmacokinetic studies. The ocular and systemic safety profile of the individual components is well established.
Tafluprost: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, systemic repeated dose toxicity, genotoxicity and carcinogenic potential. As with other PGF2 agonists, repeated dose topical ocular administration of tafluprost to monkeys produced irreversible effects on iris pigmentation and reversible enlargement of the palpebral fissure.
Increased contraction of rat and rabbit uteri in vitro was observed at tafluprost acid concentrations that exceeded 4 to 40 times, respectively, the maximum plasma concentrations of tafluprost acid in humans. Uterotonic activity of tafluprost has not been tested in human uterus preparations.
Reproduction toxicity studies were performed in the rat and rabbit with intravenous administration. In rats, no adverse effects on fertility or early embryonic development were observed at systemic exposure over 12,000 times the maximum clinical exposure based on Cmax or greater than 2,200 times based on AUC.
In conventional embryo-foetal development studies, tafluprost caused reductions in foetal body weights and increases in post-implantation losses. Tafluprost increased the incidence of skeletal abnormalities in rats as well as the incidence of skull, brain and spine malformations in rabbits. In the rabbit study, plasma levels of tafluprost and its metabolites were below the level of quantification.
In a pre- and postnatal development study in rats, increased mortality of newborns, decreased body weights and delayed pinna unfolding were observed in offspring at tafluprost doses greater than 20 times the clinical dose.
The experiments in rats with radiolabelled tafluprost showed that around 0.1% of the topically applied dose on eyes was transferred into milk. As the half-life of active metabolite (tafluprost acid) in plasma is very short (not detectable after 30 minutes in humans), most of the radioactivity probably represented metabolites with little, or no pharmacologic activity. Based on metabolism of tafluprost and natural prostaglandins, the oral bioavailability is expected to be very low.
Timolol: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction.
Reduction of intraocular pressure (IOP) in adult patients with open angle glaucoma or ocular hypertension who are insufficiently responsive to topical monotherapy with beta-blockers or prostaglandin analogues and require a combination therapy, and who would benefit from preservative free eye drops.
Posology: Recommended therapy is one eye drop in the conjunctival sac of the affected eye(s) once daily.
If one dose is missed, treatment should continue with the next dose as planned. The dose should not exceed one drop in the affected eye(s) daily.
Tapcom-S is a preservative free sterile solution packaged in a single-dose container. For single use only, one container is sufficient to treat both eyes. Any unused solution should be discarded immediately after use.
Paediatric population: The safety and efficacy of Tapcom-S in children and adolescents below the age of 18 years have not been established. No data are available.
Tapcom-S is not recommended for use in children and adolescents below the age of 18 years.
Use in elderly: No dosage alteration in elderly patients is necessary.
Use in renal/hepatic impairment: Tafluprost and timolol eye drops have not been studied in patients with renal/hepatic impairment and Tapcom-S should therefore be used with caution in such patients.
Method of Administration: Ocular use.
To reduce the risk of darkening of the eyelid skin the patients should wipe off any excess solution from the skin.
When using nasolacrimal occlusion or closing the eyelids for 2 minutes, the systemic absorption is reduced. This may result in a decrease in systemic side effects and an increase of local activity.
If more than one topical ophthalmic medicinal product is being used, each one should be administered at least 5 minutes apart.
Contact lenses should be removed before instillation of the eye drops and may be reinserted after 15 minutes.
Patients should be instructed to avoid allowing the container to come into contact with the eye or surrounding structures as this could cause injury to the eye.
Patients should also be instructed that ocular solutions, if handled improperly, can become contaminated by common bacteria known to cause ocular infections. Serious damage to the eye and subsequent loss of vision may result from using contaminated solutions.
A topical overdose with tafluprost is not likely to occur or to be associated with toxicity.
There have been reports of inadvertent overdosage with timolol resulting in systemic effects similar to those seen with systemic beta-adrenergic blocking agents such as dizziness, headache, shortness of breath, bradycardia, bronchospasm, and cardiac arrest (see also Adverse Reactions).
If overdose with Tapcom-S occurs, treatment should be symptomatic and supportive. Timolol does not dialyse readily.
Hypersensitivity to the active substances or to any of the excipients listed in Description.
Reactive airway disease including bronchial asthma, or a history of bronchial asthma, severe chronic obstructive pulmonary disease.
Sinus bradycardia, sick sinus syndrome, including sino-atrial block, second or third degree atrioventricular block not controlled with pace-maker. Overt cardiac failure, cardiogenic shock.
Systemic effects: Like other topically applied ophthalmic agents, tafluprost and timolol are absorbed systemically. Due to the beta-adrenergic component timolol, the same types of cardiovascular, pulmonary and other adverse reactions as seen with systemic beta-adrenergic blocking agents may occur. Incidence of systemic adverse reactions after topical ophthalmic administration is lower than for systemic administration. To reduce the systemic absorption, see Dosage & Administration.
Cardiac disorders: In patients with cardiovascular diseases (e.g. coronary heart disease, Prinzmetal's angina and cardiac failure) and hypotension, therapy with beta-blockers should be critically assessed and the therapy with other active substances should be considered. Patients with cardiovascular diseases should be watched for signs of deterioration of these diseases and of adverse reactions.
Due to its negative effect on conduction time, beta-blockers should only be given with caution to patients with first degree heart block.
Vascular disorders: Patients with severe peripheral circulatory disturbance/disorders (i.e. severe forms of Raynaud's disease or Raynaud's syndrome) should be treated with caution.
Respiratory disorders: Respiratory reactions, including death due to bronchospasm in patients with asthma have been reported following administration of some ophthalmic beta-blockers. Tapcom-S should be used with caution, in patients with mild/moderate chronic obstructive pulmonary disease (COPD) and only if the potential benefit outweighs the potential risk.
Hypoglycaemia/diabetes: Beta-blockers should be administered with caution in patients subject to spontaneous hypoglycaemia or to patients with labile diabetes, as beta-blockers may mask the signs and symptoms of acute hypoglycaemia.
Beta-blockers may also mask the signs of hyperthyroidism. Abrupt withdrawal of beta-blocker therapy may precipitate a worsening of symptoms.
Corneal diseases: Ophthalmic beta-blockers may induce dryness of eyes. Patients with corneal diseases should be treated with caution.
Other beta-blocking agents: The effect on intra-ocular pressure or the known effects of systemic beta-blockade may be potentiated when timolol (a component of Tapcom-S) is given to the patients already receiving a systemic beta-blocking agent. The response of these patients should be closely observed. The use of two topical β-adrenergic blocking agents is not recommended.
Angle-closure glaucoma: In patients with angle-closure glaucoma, the immediate objective of treatment is to reopen the angle. This requires constricting the pupil with a miotic. Timolol has little or no effect on the pupil. When timolol is used to reduce elevated intraocular pressure in angle-closure glaucoma it should be used with a miotic and not alone.
Anaphylactic reactions: While taking beta-blockers, patients with a history of atopy or a history of severe anaphylactic reaction to a variety of allergens may be more reactive to repeated challenge with such allergens and unresponsive to the usual doses of adrenaline used to treat anaphylactic reactions.
Choroidal detachment: Choroidal detachment has been reported with administration of aqueous suppressant therapy (e.g. timolol, acetazolamide) after filtration procedures.
Surgical anaesthesia: Beta-blocking ophthalmological preparations may block systemic beta-agonist effects e.g. of adrenaline. The anaesthesiologist should be informed when the patient is receiving timolol.
Before treatment is initiated, patients should be informed of the possibility of eyelash growth, darkening of the eyelid skin and increased iris pigmentation which are related to tafluprost therapy. Some of these changes may be permanent, and may lead to differences in appearance between the eyes when only one eye is treated.
The change in iris pigmentation occurs slowly and may not be noticeable for several months. The change in eye colour has predominantly been seen in patients with mixed coloured irises, e.g. blue-brown, grey-brown, yellow-brown and green-brown. The risk of lifelong heterochromia between the eyes in unilateral cases is obvious.
There is a potential for hair growth to occur in areas where tafluprost solution comes repeatedly in contact with the skin surface.
There is no experience with tafluprost in neovascular, angle-closure, narrow-angle or congenital glaucoma. There is only limited experience with tafluprost in aphakic patients and in pigmentary or pseudoexfoliative glaucoma.
Caution is recommended when using tafluprost in aphakic patients, pseudophakic patients with torn posterior lens capsule or anterior chamber lenses, or in patients with known risk factors for cystoid macular oedema or iritis/uveitis.
Effects on ability to drive and use machines: No studies on the effects of Tapcom-S on the ability to drive and use machines have been performed. If adverse reactions such as transient blurred vision occurs at instillation, the patient should not drive or operate machinery until the patient feels well and has clear vision.
Pregnancy: There are no or limited amount of data from the use of Tapcom-S in pregnant women.
Women of childbearing potential have to use effective contraception during Tapcom-S treatment.
Tapcom-S should not be used during pregnancy unless clearly necessary (in case no other treatment options are available).
Tafluprost: There are no adequate data for the use of tafluprost in pregnant women. Tafluprost can have harmful pharmacologic effects on pregnancy and/or the foetus/newborn child. Studies in animals have shown reproductive toxicity (see Pharmacology: Toxicology: Preclinical safety data under Actions). The potential risk for humans is unknown.
Timolol: There are no adequate data for the use of timolol in pregnant women. Timolol should not be used during pregnancy unless clearly necessary. To reduce the systemic absorption, see Dosage & Administration.
Epidemiological studies have not revealed malformative effects but show a risk for intra uterine growth retardation when beta-blockers are administered by the oral route. In addition, signs and symptoms of beta-blockade (e.g. bradycardia, hypotension, respiratory distress and hypoglycaemia) have been observed in the neonate when beta-blockers have been administered until delivery. If Tapcom-S is administered until delivery, the neonate should be carefully monitored during the first days of life.
Lactation: Beta-blockers are excreted in breast milk. However, at therapeutic doses of timolol in eye drops it is not likely that sufficient amounts would be present in breast milk to produce clinical symptoms of beta-blockade in the infant. To reduce the systemic absorption, see Dosage & Administration.
It is unknown whether tafluprost and/or its metabolites are excreted in human milk. Available toxicological data in animals have shown excretion of tafluprost and/or its metabolites in milk (for details, see Pharmacology: Toxicology: Preclinical safety data under Actions). However, at therapeutic doses of tafluprost in eye drops it is not likely that sufficient amounts would be present in breast milk to produce clinical symptoms in the infant.
As a precautionary measure lactation is not recommended if treatment with Tapcom-S is required.
Fertility: There are no data on the effects of Tapcom-S on human fertility.
In clinical studies, over 484 patients have been treated with Tapcom-S. The most frequently reported treatment-related adverse event was conjunctival/ocular hyperaemia. It occurred in approximately 7% of the patients participating in the clinical studies in Europe, was mild in most cases, and was associated with discontinuation of treatment in 1.2% of patients.
The adverse reactions reported in the clinical studies using Tapcom-S were limited to those earlier reported for either of the single active substances tafluprost or timolol. No new adverse reactions specific for Tapcom-S were observed in the clinical studies. The majority of adverse reactions reported were ocular, mild or moderate in severity and none were serious.
Like other topically applied ophthalmic agents, tafluprost and timolol are absorbed systemically. This may cause similar undesirable effects as seen with systemic beta-blocking agents. Incidence of systemic adverse reactions after topical ophthalmic administration is lower than for systemic administration. Listed adverse reactions include reactions seen within the class of ophthalmic beta-blockers.
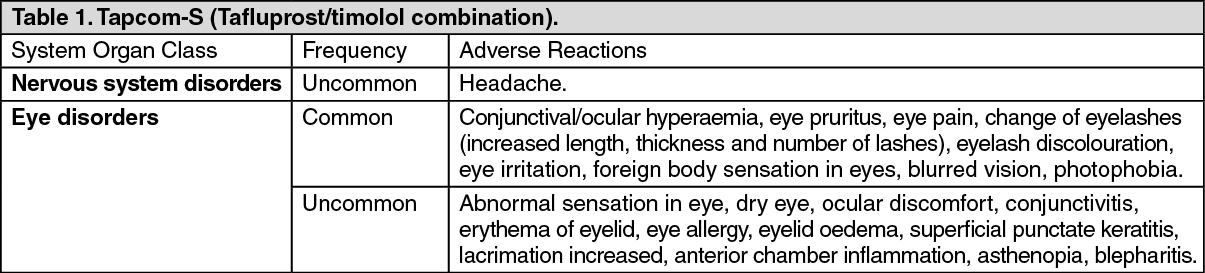
The following adverse reactions have been reported with Tapcom-S during clinical trials (within each frequency grouping, adverse reactions are presented in order of decreasing frequency).
The frequency of possible adverse reactions listed as follows is defined using the following convention: Very common: ≥1/10; common: ≥1/100 to <1/10; uncommon: ≥1/1,000 to <1/100; rare: ≥1/10,000 to <1/1,000; very rare: <1/10,000; not known: frequency cannot be estimated from the available data. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Additional adverse reactions that have been seen with either of the active substances (tafluprost or timolol), and may potentially occur also with this product are listed as follows: See Tables 2 and 3.
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Cases of corneal calcification have been reported very rarely in association with the use of phosphate containing eye drops in some patients with significantly damaged corneas.
No interaction studies have been performed.
There is a potential for additive effects resulting in hypotension and/or marked bradycardia when ophthalmic beta blockers solution is administered concomitantly with oral calcium channel blockers, beta-adrenergic blocking agents, antiarrhythmics (including amiodarone), digitalis glycosides, parasympathomimetics, guanethidine.
Oral β-adrenergic blocking agents may exacerbate the rebound hypertension which can follow the withdrawal of clonidine.
Potentiated systemic beta-blockade (e.g., decreased heart rate, depression) has been reported during combined treatment with CYP2D6 inhibitors (e.g. quinidine, fluoxetine, paroxetine) and timolol.
Mydriasis resulting from concomitant use of ophthalmic beta-blockers and adrenaline (epinephrine) has been reported occasionally.
Incompatibilities: Not applicable.
Store in a refrigerator (2°C - 8°C).
After opening the foil pouch: Keep the single-dose containers in the original foil pouch in order to protect from light. Do not store above 25°C. Discard an opened single-dose container with any remaining solution immediately after use.
Shelf life: 3 years.
After first opening a foil pouch: 28 days.
S01ED51 - timolol, combinations ; Belongs to the class of beta blocking agents. Used in the treatment of glaucoma.
Tapcom-S ophth soln
0.3 mL x 30 × 1's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image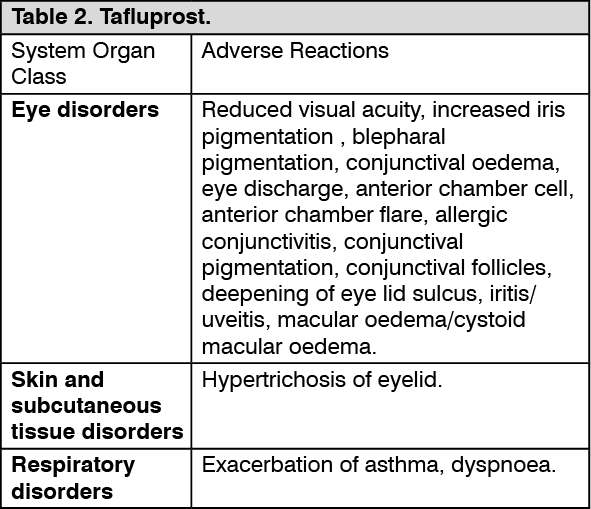 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image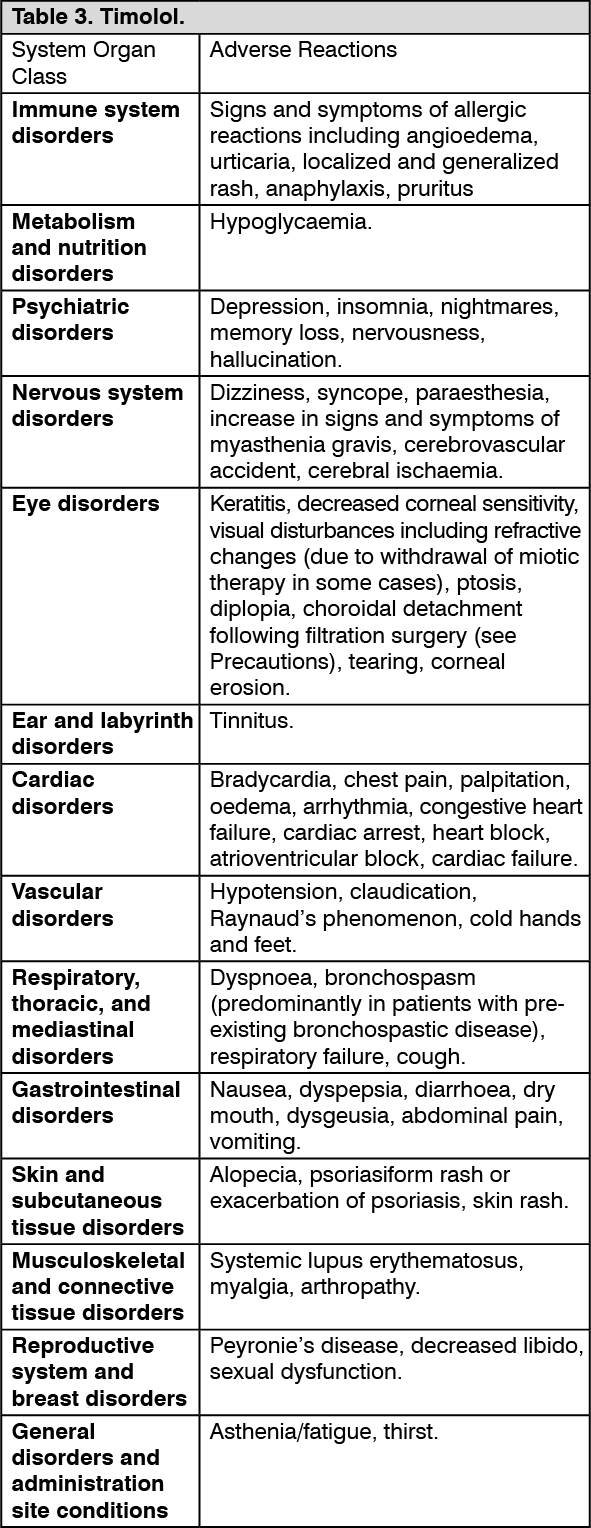 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
