


 Sign Out
Sign Out

Posology: Treatment should be continued as long as clinical benefit is observed or until unacceptable toxicity occurs.
If a dose is missed the patient should not take an additional dose, but take the usual prescribed next dose.
Posology for Philadelphia chromosome positive CML adult patients: The recommended dose is: 300 mg twice daily in newly diagnosed patients with CML in the chronic phase; 400 mg twice daily in patients with chronic or accelerated phase CML with resistance or intolerance to prior therapy.
For a dose of 300 mg twice daily, 150 mg hard capsules are available.
For a dose of 400 mg once daily (see Dose adjustments or modifications as follows), 200 mg hard capsules are available.
Philadelphia chromosome positive CML patients in chronic phase who have been treated with nilotinib as first-line therapy and who achieved a sustained deep molecular response (MR4.5): Discontinuation of treatment may be considered in eligible Philadelphia chromosome positive (Ph+) CML patients in chronic phase who have been treated with nilotinib at 300 mg twice daily for a minimum of 3 years if a deep molecular response is sustained for a minimum of one year immediately prior to discontinuation of therapy. Discontinuation of nilotinib therapy should be initiated by a physician experienced in the treatment of patients with CML (see Precautions and Pharmacology: Pharmacodynamics under Actions).
Eligible patients who discontinue nilotinib therapy must have their BCR-ABL transcript levels and complete blood count with differential monitored monthly for one year, then every 6 weeks for the second year, and every 12 weeks thereafter. Monitoring of BCR-ABL transcript levels must be performed with a quantitative diagnostic test validated to measure molecular response levels on the International Scale (IS) with a sensitivity of at least MR4.5 (BCR-ABL/ABL ≤0.0032% IS).
For patients who lose MR4 (MR4=BCR-ABL/ABL ≤0.01% IS) but not MMR (MMR=BCR-ABL/ABL ≤0.1% IS) during the treatment-free phase, BCR-ABL transcript levels should be monitored every 2 weeks until BCR-ABL levels return to a range between MR4 and MR4.5. Patients who maintain BCR-ABL levels between MMR and MR4 for a minimum of 4 consecutive measurements can return to the original monitoring schedule.
Patients who lose MMR must re-initiate treatment within 4 weeks of when loss of remission is known to have occurred. Nilotinib therapy should be re-initiated at 300 mg twice daily or at a reduced dose level of 400 mg once daily if the patient had a dose reduction prior to discontinuation of therapy. Patients who re-initiate nilotinib therapy should have their BCR-ABL transcript levels monitored monthly until MMR is re-established and every 12 weeks thereafter (see Precautions).
Dose adjustments or modifications: Tasigna may need to be temporarily withheld and/or dose reduced for haematological toxicities (neutropenia, thrombocytopenia) that are not related to the underlying leukaemia (see Table 8).
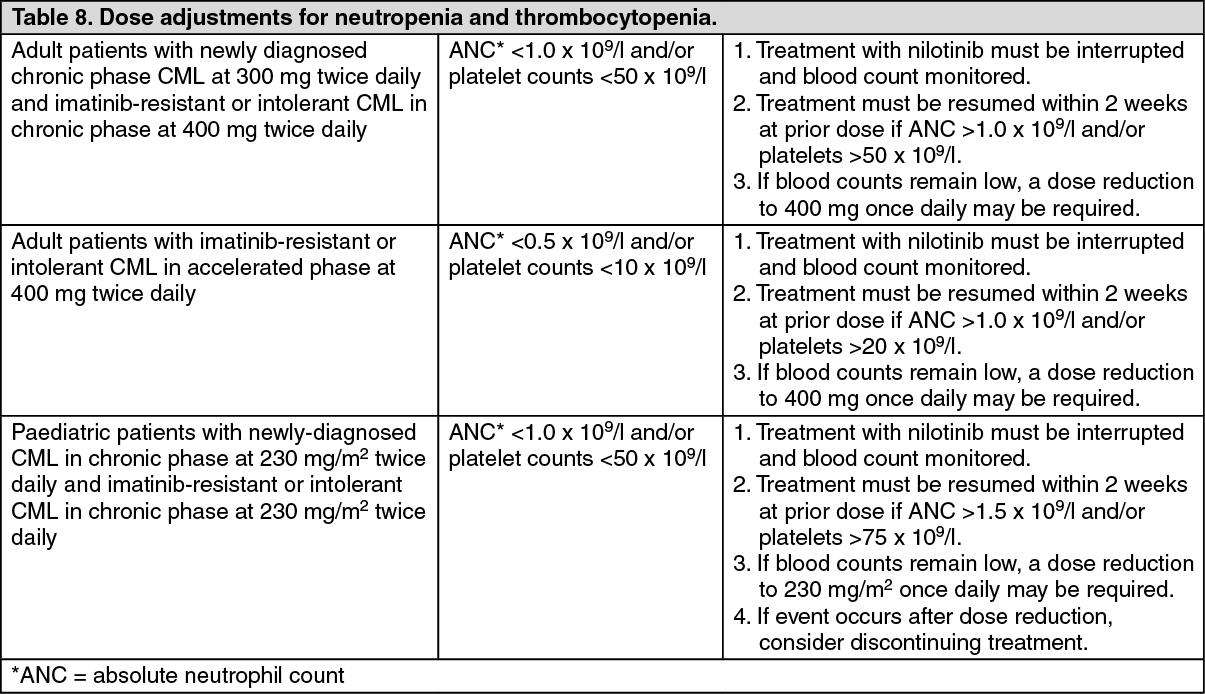 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIf clinically significant moderate or severe non-haematological toxicity develops, dosing should be interrupted, and patients should be monitored and treated accordingly. If the prior dose was 300 mg twice daily in adult newly diagnosed patients with CML in the chronic phase, or 400 mg twice daily in adult patients with imatinib-resistant or intolerant CML in chronic or accelerated phase, or 230 mg/m2 twice daily in paediatric patients, dosing may be resumed at 400 mg once daily in adult patients and at 230 mg/m2 once daily in paediatric patients once the toxicity has resolved. If the prior dose was 400 mg once daily in adult patients or 230 mg/m2 once daily in paediatric patients, treatment should be discontinued. If clinically appropriate, re-escalation of the dose to the starting dose of 300 mg twice daily in adult newly diagnosed patients with CML in the chronic phase or to 400 mg twice daily in adult patients with imatinib-resistant or intolerant CML in chronic or accelerated phase or to 230 mg/m2 twice daily in paediatric patients should be considered.
Elevated serum lipase: For Grade 3-4 serum lipase elevations, doses in adult patients should be reduced to 400 mg once daily or interrupted. In paediatric patients, treatment must be interrupted until the event returns to Grade ≤1. Thereafter, if the prior dose was 230 mg/m2 twice daily, treatment can be resumed at 230 mg/m2 once daily. If the prior dose was 230 mg/m2 once daily, treatment should be discontinued. Serum lipase levels should be tested monthly or as clinically indicated (see Precautions).
Elevated bilirubin and hepatic transaminases: For Grade 3-4 bilirubin and hepatic transaminase elevations in adult patients, doses should be reduced to 400 mg once daily or interrupted. For Grade ≥2 bilirubin elevations or Grade ≥3 hepatic transaminase elevations in paediatric patients, treatment must be interrupted until the levels return to Grade ≤1. Thereafter, if the prior dose was 230 mg/m2 twice daily, treatment can be resumed at 230 mg/m2 once daily. If the prior dose was 230 mg/m2 once daily, and recovery to Grade ≤1 takes longer than 28 days, treatment should be discontinued. Bilirubin and hepatic transaminases levels should be tested monthly or as clinically indicated.
Special populations: Elderly: Approximately 12% of subjects in the Phase III study in patients with newly diagnosed CML in chronic phase and approximately 30% of subjects in the Phase II study in patients with imatinib-resistant or intolerant CML in chronic phase and accelerated phase were 65 years of age or over. No major differences were observed for safety and efficacy in patients ≥65 years of age as compared to adults aged 18 to 65 years.
Renal impairment: Clinical studies have not been performed in patients with impaired renal function.
Since nilotinib and its metabolites are not renally excreted, a decrease in total body clearance is not anticipated in patients with renal impairment.
Hepatic impairment: Hepatic impairment has a modest effect on the pharmacokinetics of nilotinib. Dose adjustment is not considered necessary in patients with hepatic impairment. However, patients with hepatic impairment should be treated with caution (see Precautions).
Cardiac disorders: In clinical studies, patients with uncontrolled or significant cardiac disease (e.g. recent myocardial infarction, congestive heart failure, unstable angina or clinically significant bradycardia) were excluded. Caution should be exercised in patients with relevant cardiac disorders (see Precautions).
Increases in total serum cholesterol levels have been reported with nilotinib therapy (see Precautions). Lipid profiles should be determined prior to initiating nilotinib therapy, assessed at month 3 and 6 after initiating therapy and at least yearly during chronic therapy.
Increases in blood glucose levels have been reported with nilotinib therapy (see Precautions). Blood glucose levels should be assessed prior to initiating nilotinib therapy and monitored during treatment.
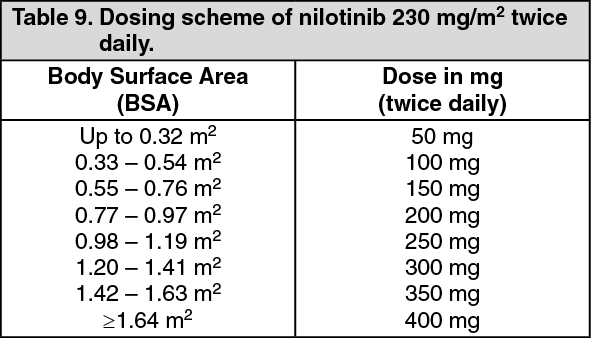
200 mg: Posology for Philadelphia chromosome positive CML paediatric patients: Dosing in paediatric patients is individualised and is based on body surface area (mg/m2). The recommended dose of nilotinib is 230 mg/m2 twice daily, rounded to the nearest 50 mg dose (to a maximum single dose of 400 mg) (see Table 9). Different strengths of Tasigna hard capsules can be combined to attain the desired dose.
There is no experience with treatment of paediatric patients below 2 years of age. There are no data in newly diagnosed paediatric patients below 10 years of age and limited data in imatinib-resistant or intolerant paediatric patients below 6 years of age. (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePhiladelphia chromosome positive CML patients in chronic phase who have achieved a sustained deep molecular response (MR 4.5) on nilotinib following prior imatinib therapy: Discontinuation of treatment may be considered in eligible Philadelphia chromosome positive (Ph+) CML patients in chronic phase who have been treated with nilotinib for a minimum of 3 years if a deep molecular response is sustained for a minimum of one year immediately prior to discontinuation of therapy. Discontinuation of nilotinib therapy should be initiated by a physician experienced in the treatment of patients with CML (see Precautions and Pharmacology: Pharmacodynamics under Actions).
Eligible patients who discontinue nilotinib therapy must have their BCR-ABL transcript levels and complete blood count with differential monitored monthly for one year, then every 6 weeks for the second year, and every 12 weeks thereafter. Monitoring of BCR-ABL transcript levels must be performed with a quantitative diagnostic test validated to measure molecular response levels on the International Scale (IS) with a sensitivity of at least MR4.5 (BCR-ABL/ABL ≤0.0032% IS).
Patients with confirmed loss of MR4 (MR4=BCR-ABL/ABL ≤0.01% IS) during the treatment-free phase (two consecutive measures separated by at least 4 weeks showing loss of MR4) or loss of major molecular response (MMR=BCR-ABL/ABL ≤0.1% IS) must re-initiate treatment within 4 weeks of when loss of remission is known to have occurred. Nilotinib therapy should be re-initiated at either 300 mg or 400 mg twice daily. Patients who re-initiate nilotinib therapy should have their BCR-ABL transcript levels monitored monthly until previous major molecular response or MR4 level is re-established and every 12 weeks thereafter (see Precautions).
Special populations: Paediatric population: The safety and efficacy of Tasigna in paediatric patients with Philadelphia chromosome positive CML in chronic phase from 2 to less than 18 years of age have been established (see Adverse Reactions and Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions). There is no experience in paediatric patients below 2 years of age or in paediatric patients with Philadelphia chromosome positive CML in accelerated phase or blast crisis. There are no data in newly diagnosed paediatric patients below 10 years of age and limited data in imatinib-resistant or intolerant paediatric patients below 6 years of age.
Method of administration: Tasigna should be taken twice daily approximately 12 hours apart and must not be taken with food. The hard capsules should be swallowed whole with water. No food should be consumed for 2 hours before the dose is taken and no food should be consumed for at least one hour after the dose is taken.
For patients who are unable to swallow hard capsules, the content of each hard capsule may be dispersed in one teaspoon of apple sauce (puréed apple) and should be taken immediately. Not more than one teaspoon of apple sauce and no food other than apple sauce must be used (see Precautions and Pharmacology: Pharmacokinetics under Actions).